
Abstract
Background
Vascular graft infection is a very complex disease. Although complete excision of the infected grafts with extra-anatomic bypass or in situ reconstruction is a general treatment strategy, some concerns including reinfection in the new graft remain.
Case Report
An 88 year-old man presented to the hospital with abdominal swelling and bleeding. The patient had undergone revascularization for aorto-iliac occlusive disease twice in the past. The first procedure had been performed 15 years previously, with right ilio-femoral bypass grafting for right iliac artery occlusion and stent implantation for left iliac artery stenosis. The second procedure had been performed 10 years previously, with aorta-to-left femoral and left-to-right femoro-femoral bypass grafting because the terminal aorta, the first ilio-femoral bypass graft, and the stent of the left iliac artery had been occluded. The patient was diagnosed with vascular graft infection, and endovascular therapy was selected as the revascularization method prior to graft excision. It was successfully performed using various devices and techniques, followed by graft excision without critical limb ischemia.
Conclusion
This case demonstrates that endovascular therapy prior to graft excision can be an alternative revascularization method for vascular graft infection after bypass surgery for aorto-iliac occlusive disease.
Keywords
Introduction
Vascular graft infection (VGI) is a very complex disease with high morbidity and mortality rates. 1 Although complete excision of the infected grafts with extra-anatomic bypass or in situ reconstruction is a general treatment strategy,2,3 some concerns including reinfection in the new graft remain.
We report the case of an elderly man with VGI after multiple bypass surgeries for aorto-iliac occlusive disease. Endovascular therapy (EVT) was selected as the revascularization method prior to graft excision. It was successfully performed using various devices and techniques, followed by graft excision without critical limb ischemia.
Case Report
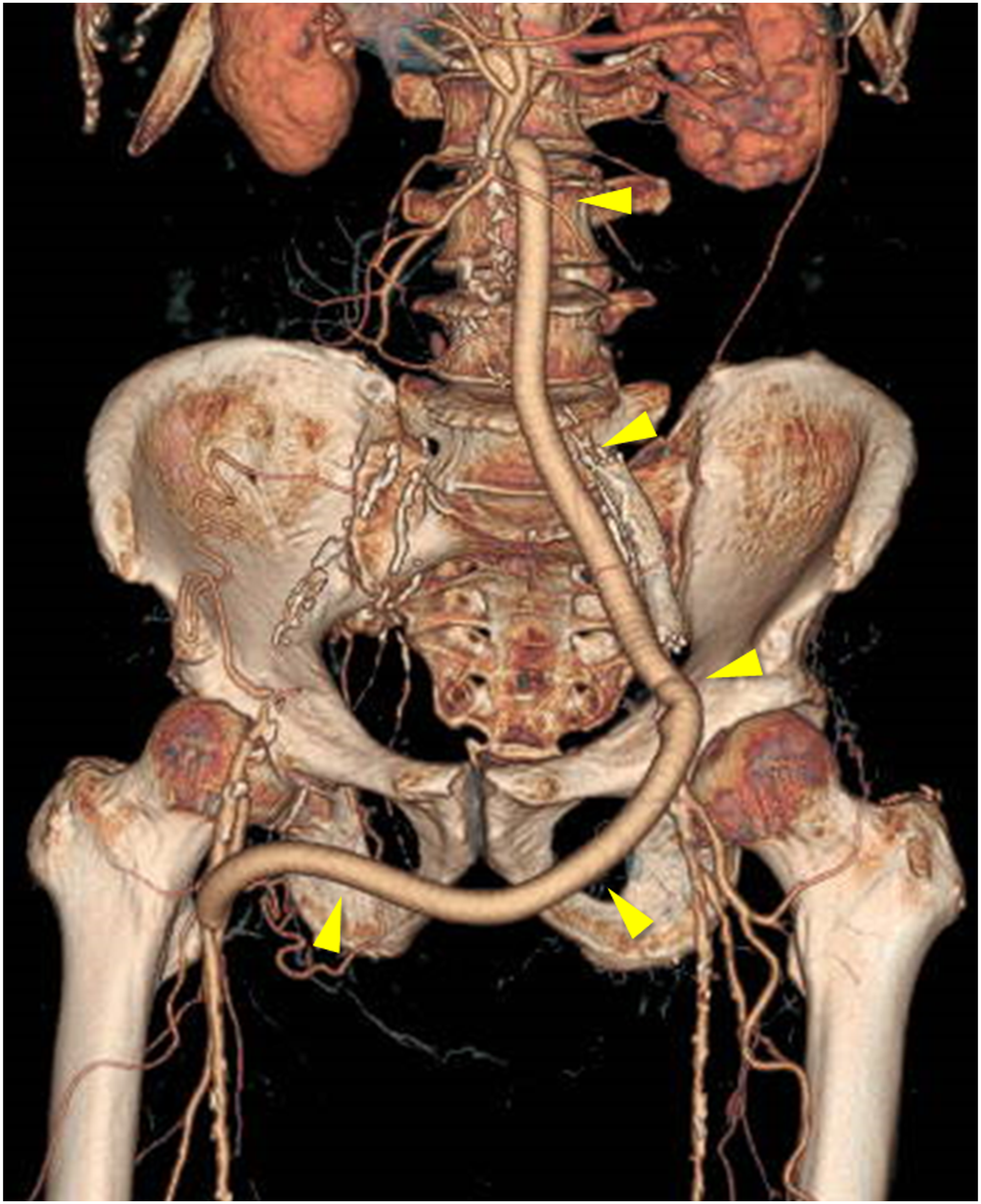
An 88 year-old man presented to the hospital with abdominal swelling and bleeding. The patient had undergone revascularization for aorto-iliac occlusive disease twice in the past. The first procedure had been performed 15 years previously, with right ilio-femoral bypass grafting for right iliac artery occlusion and stent implantation for left iliac artery stenosis. The second procedure had been performed 10 years previously, with aorta-to-left femoral and left-to-right femoro-femoral bypass grafting because the terminal aorta, the first ilio-femoral bypass graft, and the stent of the left iliac artery had been occluded. Computed tomography (CT) demonstrated massive abscess with air bubbles around the patent left-to-right femoro-femoral bypass graft and a fistula to the abdominal skin (Figure 1). The abscess involved the bifemoral anastomoses of the left-to-right femoro-femoral bypass graft and partially extended to the aorta-to-left femoral bypass graft. CT angiography demonstrated patency of the infected aorto-femoro-femoral bypass graft supplying the bilateral femoral arteries (Figure 2). As a diagnosis of VGI, antibiotic treatment was initiated immediately, followed by drainage and irrigation. Although Clostridium perfringens and multidrug-resistant Staphylococcus epidermidis were detected in the swab of the abscess, the blood culture was negative. Axial (A) and sagittal (B) CT images on admission. Massive abscess with air bubbles (blue arrows) around the patent left-to-right femoro-femoral bypass graft (yellow arrowheads) and a fistula to the abdominal skin (red arrow) are demonstrated. Three-dimensional imaging of CT angiography on admission. Patency of the infected aorto-femoro-femoral bypass (yellow arrowheads) is demonstrated.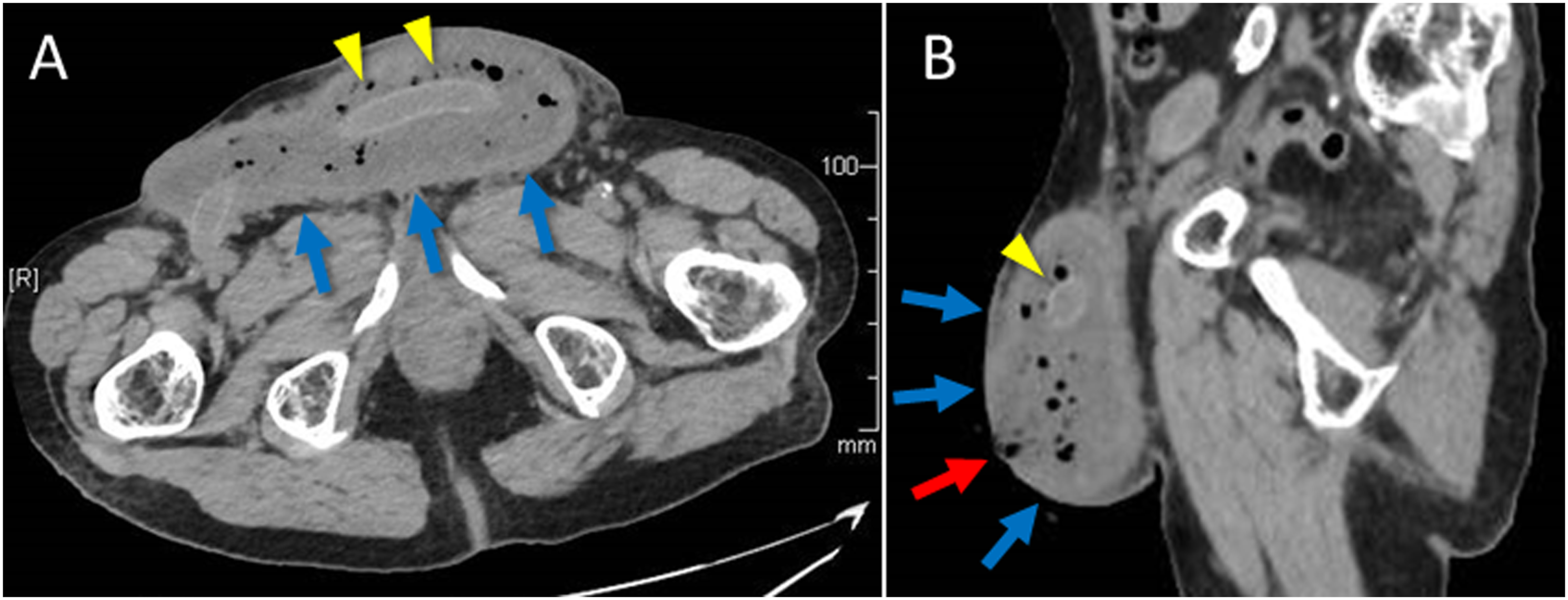
Although excision of the infected graft with extra-anatomic axillo-femoral bypass grafting was considered reasonable, concerns of reinfection in the new graft and life-threatening aortic stump blowout accompanied it. It was considered that EVT was extremely challenging but was an option by which these concerns could be avoided. Although the native right iliac artery was found to have been cut and ligated in the past surgery, the occluded right ilio-femoral bypass graft that was not infected could be an alternative target of revascularization.
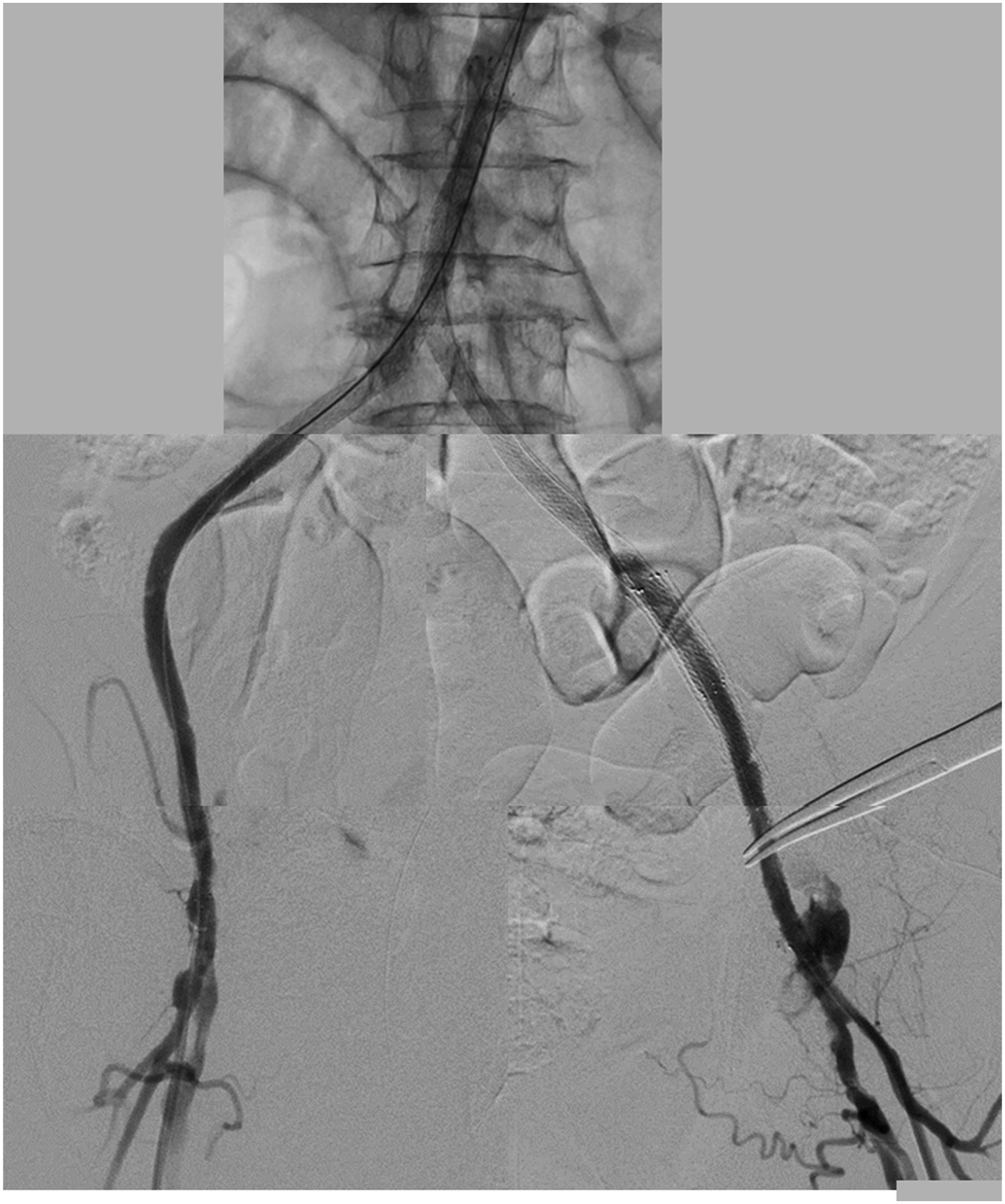
EVT for the occluded terminal aorta, right ilio-femoral bypass graft, and left native iliac artery was performed. Bilateral common femoral arteries were punctured with ultrasound-guided and 6-French short sheaths were inserted as bilateral retrograde systems. 6-French 98-cm Parent Plus sheath (Medikit, Tokyo, Japan) was also inserted from the left brachial artery to the distal part of the descending aorta as an antegrade system. From the antegrade system, .014-inch VASSALO NS3 guidewire (Cordis, Tokyo, Japan) entered the occluded terminal aorta and advanced to the in-stent part of the left iliac artery with the support of a 7-French Guide Liner PV guide-extension catheter (Teleflex, Wayne, United States of America; Supplemental Video 1). From the left retrograde system, .014-inch Gladius ES guidewire (ASAHI INTECC, Aichi, Japan) with 2.2/2.5-French X SUPPORT microcatheter (ZEON MEDICAL, Tokyo, Japan) entered the left iliac artery and could rendezvous with the antegrade catheter (Supplemental Video 2). From the right retrograde system, .014-inch VASSALLO 14 guidewire (Cordis, Tokyo, Japan) with 2.2/2.5-French X SUPPORT microcatheter entered the occluded graft but hardly advanced because of the strong resistance of the vessel. Using the knuckle wire technique, .035-inch Radifocus Guidewire M half stiff type angle (Terumo, Tokyo, Japan) with 4.0-French CXI Support Catheter curved type (Cook Medical Japan, Tokyo, Japan) advanced to the subintimal space of the terminal aorta (Supplemental Video 3). Finally, .014-inch Astato XS 9-40 guidewire (ASAHI INTECC, Aichi, Japan) could advance to the intraplaque lumen and rendezvous with the antegrade catheter using the intravenous ultrasound (IVUS) -guided technique (Figure 3; Supplemental Video 4). Although the vessels were dilated with balloons, their antegrade flow was not confirmed angiographically (Supplemental Video 5). In consideration of blood flow competition with the infected graft, a small incision was made in the lower left abdomen under local anesthesia, and the distal part of the aorta-to-left femoral bypass graft was directly clamped. Then, the antegrade flow of the infected graft disappeared, and that of the dilated vessels appeared angiographically. Two identical self-expanding nitinol stents (8.0-mm-diameter 150-mm-length S.M.A.R.T; Cordis, Tokyo, Japan) were simultaneously implanted from the terminal aorta to the right graft and the left common iliac artery. Additional stents were consecutively implanted to cover the residual lesions on the right (8.0-mm-diameter 100-mm-length S.M.A.R.T; Cordis, Tokyo, Japan) and left sides (8.0-mm-diameter 100-mm-length Misago; Terumo, Tokyo, Japan). After dilation of the stents with 6.0-mm-diameter balloons, sufficient flow of the target vessels was angiographically confirmed (Figure 4; Supplemental Videos 6-8). At the end of the procedure, the distal part of the aorta-to-left femoral bypass graft was surgically ligated. Fluoroscopic image during EVT. From the right retrograde system, .014-inch Astato XS 9-40 guidewire (yellow arrows) could advance to the intraplaque lumen and rendezvous with the antegrade catheter (green arrows) using the IVUS-guided technique. The IVUS catheter (blue arrows) was inserted from the left retrograde system. Synthesized image of the final angiography. Sufficient flow of the target vessels was confirmed.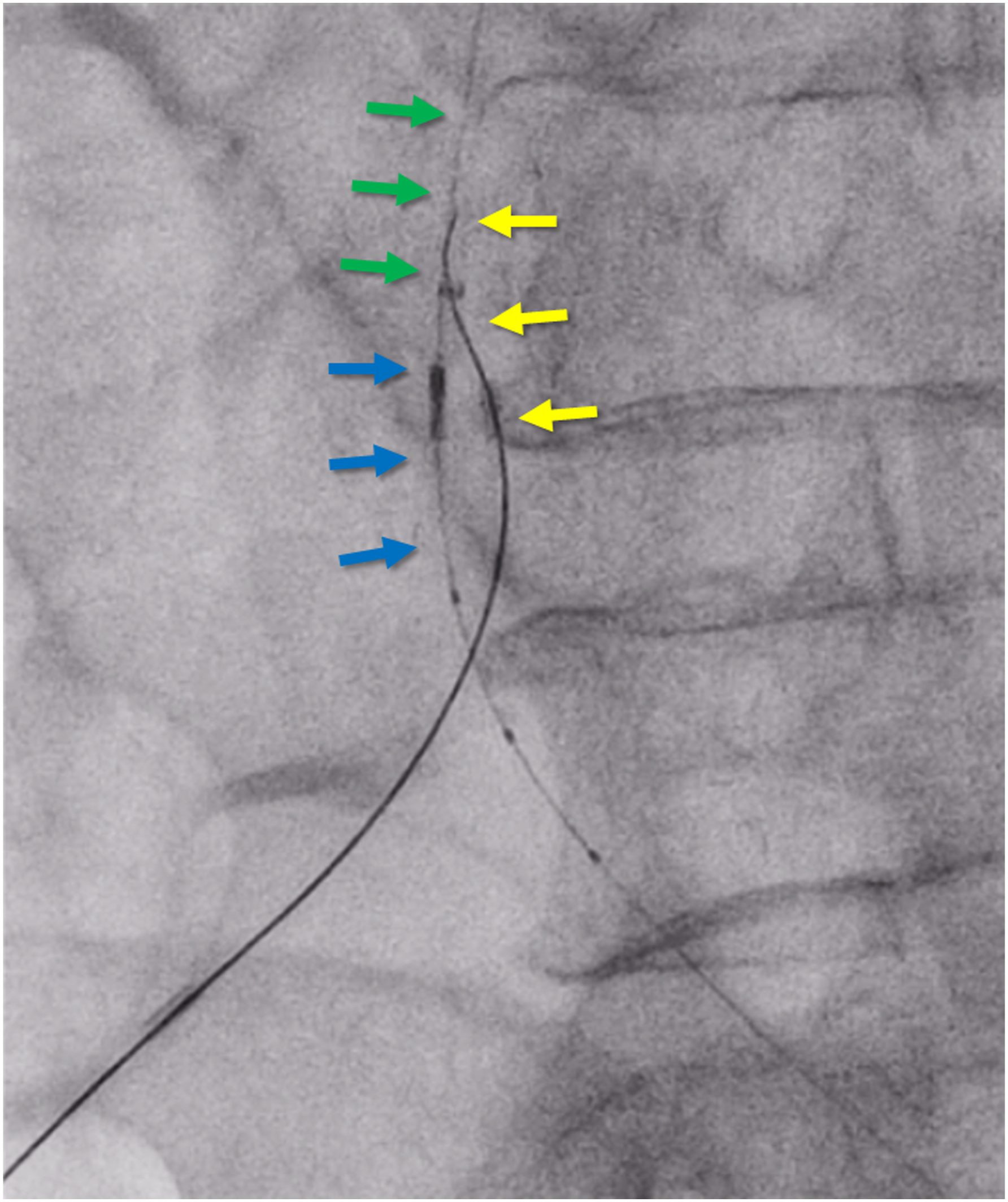
3 days later, surgery with excision of the infected graft and debridement was performed without critical limb ischemia. The patient was discharged 6 weeks later and was asymptomatic with a preserved ankle-brachial index at a 3-month follow-up clinic visit. Although the patient died because of non-cardiovascular disease approximately 2 months after the clinic visit, lower limb ischemia and reinfection were not found clinically until then.
Discussion
VGI is a very complex disease with high morbidity and mortality rates. It has been reported that the frequency of VGI ranges from 1% to 6% in patients who underwent vascular graft implantation.1,4 The mortality rate is estimated to be 10%-25% within 30 days after the diagnosis, and the risk of amputation is estimated to be 4%-14%. 1
The clinical manifestations of VGI are variable and relate to whether the location is extracavitary or intracavitary, the pathogenesis of infection, and the duration of time since surgery. 3 In patients with intracavitary VGI, in situ reconstruction with venous autografts, arterial allografts or rifampin-bonded synthetic grafts is generally recommended. 3 Venous autografts are particularly superior in terms of durability and reinfection rates.3,5 On the other hand, in cases caused by MRSA, Pseudomonas, or multidrug-resistant microorganisms, extra-anatomic bypass revascularization followed by graft excision is recommended rather than in situ reconstruction because of recurrent infection. 3 However, this procedure has several disadvantages as follows: a 2-stage invasive procedure with general anesthesia is required; conduit failure with amputation of the lower extremities has been observed in 20%-30% of patients; blood supply is decreased with ischemia to the inferior mesenteric and internal iliac arteries; and residual infection of the aortic stump with blowout occurs in 10%-20% of patients.3,5
Although the efficacy of EVT as a revascularization method for VGI is unclear and can be challenging in most cases, it can be an alternative method by which the above-mentioned problems can be avoided. In addition, it has been reported that early and midterm outcomes of EVT with primary stenting for complex aortoiliac lesions are acceptable. 6 Covered stents are superior to bare nitinol stents in durability, 7 but they have a risk of reinfection and require long-term dual antiplatelet therapy. For patients with VGI who must undergo surgery with graft excision within a few days, the use of bare nitinol stents would be reasonable. As a point to be noted regarding EVT, blood flow competition with the revascularized vessel and infected graft may occur, as in this case. Therefore, surgical clamping of the infected graft is probably necessary to avoid acute occlusion of the revascularized vessel.
In this case, the situation was very complex because VGI caused by multidrug-resistant microorganisms extended to the intracavitary region and the native right iliac artery had been cut in the past surgery. EVT for this case was considered extremely challenging but was successfully performed using various devices and techniques, including high-trackability guide wires, combined use of support catheters, bidirectional and IVUS-guided technique, followed by graft excision without critical limb ischemia.
Conclusion
EVT was successfully performed for VGI after multiple bypass surgeries for aorto-iliac occlusive disease. This case demonstrates that EVT prior to graft excision can be an alternative revascularization method for VGI, even in such a complex situation.
Supplemental Material
Supplemental Material
Supplemental Material
Supplemental Material
Supplemental Material
Supplemental Material
Supplemental Material
Supplemental Material
Footnotes
Acknowledgements
We thank Dr Yoshiki Nagata and Dr Naoki Saito for their clinical support.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
Informed consent for publication, including the patient’s data, was obtained from the patient.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.