
Abstract
Common carotid artery pseudoaneurysm is the formation of a hematoma outside the vessel wall resulting from a transmural rupture. Its causes include open or blunt trauma, infections, or previous surgical procedures. These lesions usually present with a wide range of symptoms due to mass effect, and the diagnosis relies on a high index of suspicion and imaging methods. Treatment remains controversial; however, surgical management—either open or endovascular—is generally preferred. This report presents the case of a 19-year-old patient with a history of gunshot wound in neck. Imaging revealed a pseudoaneurysm of the right common carotid artery, which was surgically treated through resection and interposition of an ePTFE graft. This article discusses the etiology, diagnosis, and treatment of post-traumatic carotid artery pseudoaneurysm, with the aim of increasing awareness of this condition and its clinical presentations, thereby promoting timely diagnosis and appropriate therapeutic intervention to prevent fatal outcomes.
Introduction
A pseudoaneurysm is a condition characterized by a pulsatile, encapsulated hematoma that forms following a tear or injury to the arterial wall, resulting in blood leakage from the artery into the surrounding tissue while maintaining communication with the vessel lumen.1–3
The incidence of common carotid artery pseudoaneurysms is rare; among all extracranial aneurysms, they account for only 0.1%-0.4%, and represent less than 1% of all peripheral aneurysms.2–6
Several mechanisms can lead to the development of this condition, including blunt and/or penetrating trauma (with an incidence of approximately 0.08%-0.33%), 6 direct arterial injury, atherosclerosis, infection, carotid dissection, post-radiation therapy, iatrogenic causes (such as post-endarterectomy, with an incidence of approximately 0.3%-0.6%, or stent placement), connective tissue diseases, and fibromuscular dysplasia.1–3,5–10 Post-traumatic pseudoaneurysms resulting from penetrating or blunt neck trauma are typically due to damage to the intimal or medial layer, leading to blood extravasation into the surrounding tissues.1,5,9 The most common site for extracranial carotid artery pseudoaneurysm is the external or common carotid artery. 1
Patients with this condition may remain asymptomatic or present with a pulsatile neck mass, which is the most frequent manifestation.1,7,9 Depending on the size and location, symptoms may arise due to compression of the airway or adjacent structures. Clinical presentations may include dyspnea, dysphagia, hoarseness, recurrent laryngeal nerve palsy, Horner’s syndrome, headache, neck pain, epistaxis, embolism and cerebral ischemia, syncope, and hemorrhage.1,7,9–11
Diagnosing pseudoaneurysms requires a high index of suspicion. Confirmation can be achieved through Doppler ultrasound, CT angiography, magnetic resonance imaging, or conventional angiography. Angiography remains the gold standard, although it is invasive and costly.1,5,6,9
Management of this condition is complex and remains a significant surgical challenge. Treatment depends on the nature, location, and morphology of the lesion, as well as patient-specific factors and available resources. Therapeutic options include conservative management with expectant management through close monitoring and serial imaging studies, ultrasound guidance thrombin injection, open surgical repair (resection and anastomosis, primary repair, graft interposition (vein or synthetic), or arterial ligation), endovascular intervention (stent placement or embolization), or combined approaches.1,2,4,5,7–10,12–14 Traditionally, open surgery has been the treatment of choice; however, endovascular techniques have gained increasing relevance in recent years.5,9,11
We present the case of a patient who developed a right common carotid artery pseudoaneurysm secondary to a gunshot wound, which was treated with interposition of an ePTFE graft. The objective of this report is to highlight the key features, diagnosis, and treatment of this condition.
Clinical Case
A 19-year-old male patient with no history of chronic degenerative diseases. The only relevant medical history is daily marijuana use since the age of 12, averaging 2 cigarettes per day.
The current condition began 5 days prior to admission after sustaining multiple gunshot wounds to the hand, neck, chest, and back, resulting in blood loss but without loss of consciousness. He initially presented to a General Hospital, where a chest tube was placed to drain a hemothorax. A computed tomography (CT) scan reported a probable carotid artery aneurysm, prompting referral to the Emergency Department of the XXI Century National Medical Center for evaluation by the Vascular and Endovascular Surgery Department.
Focused physical examination revealed a symmetric, cylindrical neck with carotid pulses 3/3, without bruit or thrill. A gunshot wound was noted in Zone 2 of the right side of the neck, approximately 2 cm in diameter with regular edges and no signs of active bleeding or expanding hematoma. Gunshot wounds were also present on the chest, back, gluteal region, and right upper extremity, without signs of active bleeding. A right chest tube was in place, draining 800 cc of hematic fluid. The remainder of the physical examination was unremarkable.
The physical examination referred to was performed at our center; prior to the patient’s arrival, such findings were not documented in the medical notes, and the exact reasons for this are unknown to us.
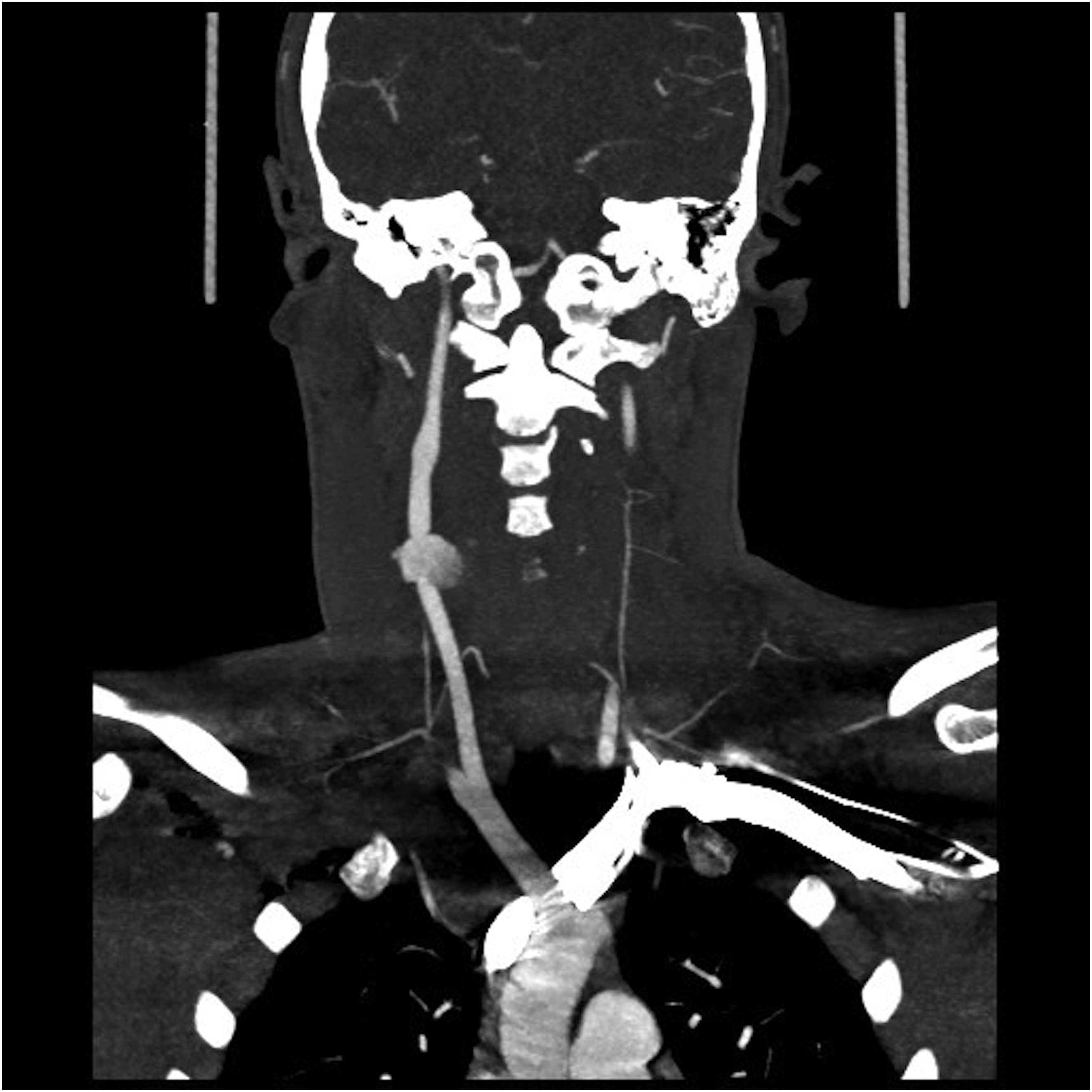
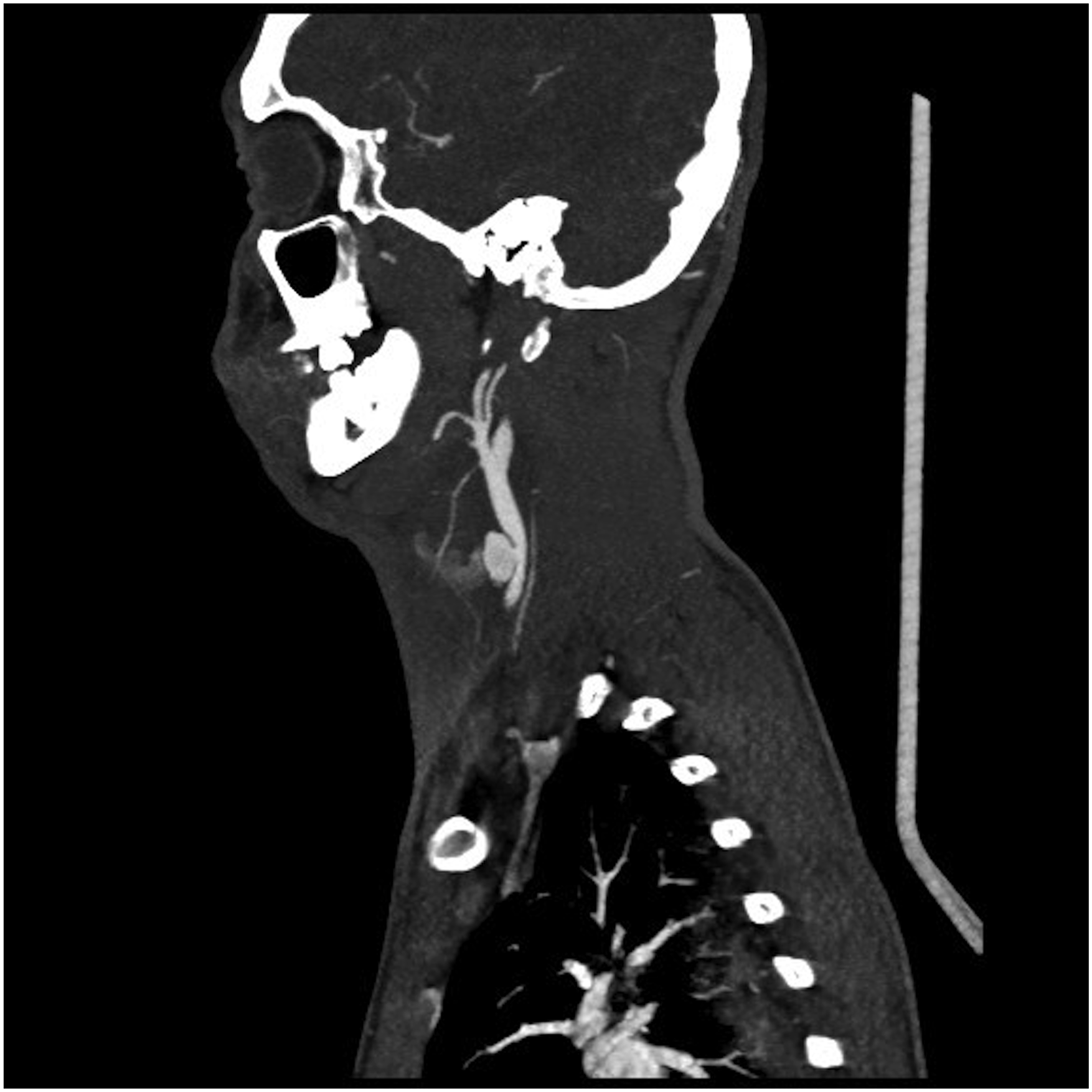
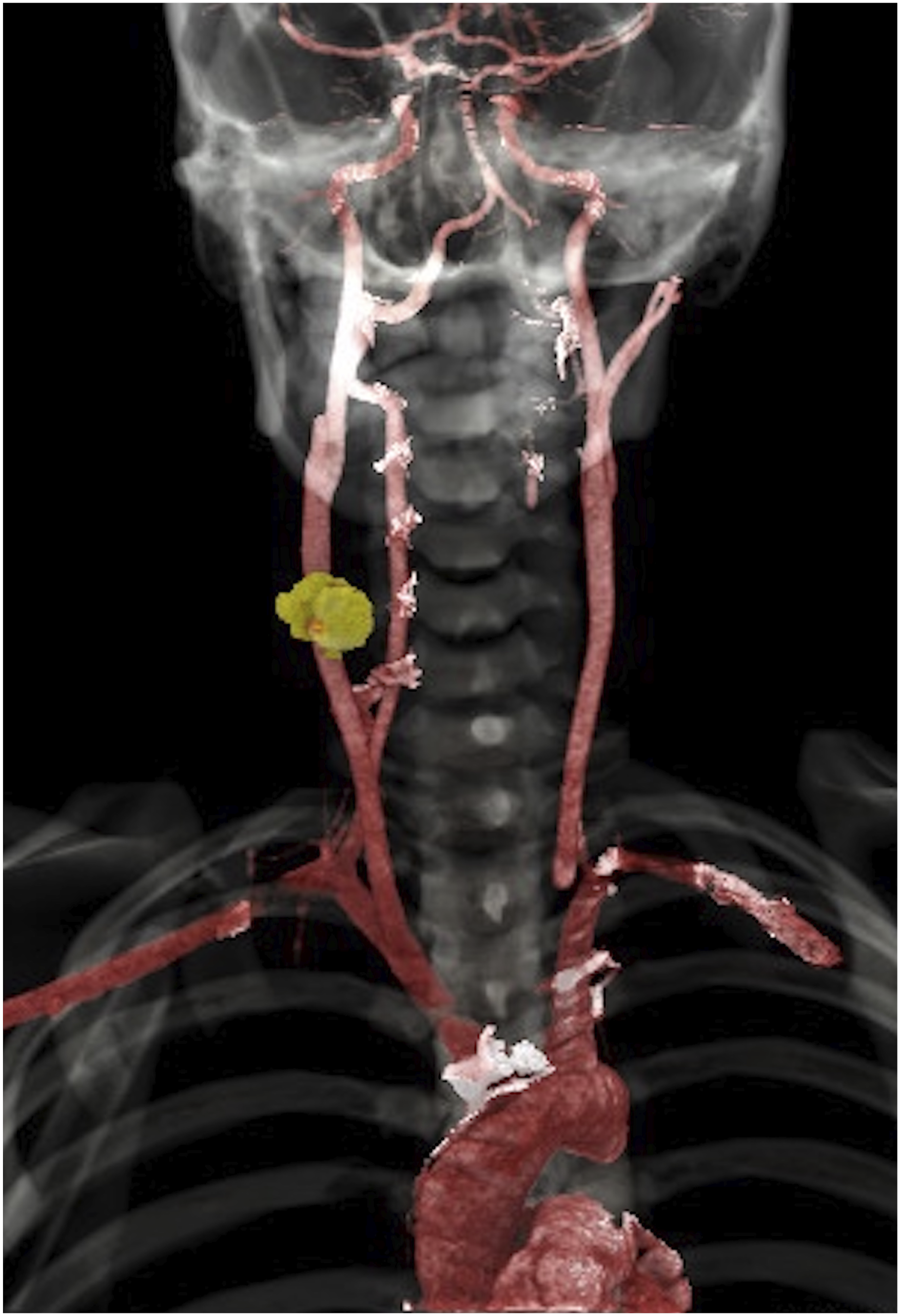
A CT angiography of the supra-aortic trunks revealed a contrast extravasation was observed in the anterior wall of the mid-segment of the right common carotid artery, suggestive of a pseudoaneurysm measuring approximately 16 × 12 mm. The internal and external carotid arteries appeared unremarkable. (Figure 1-4), prompting emergency surgical intervention. CT Angiography. Axial Section Showing Pseudoaneurysm of the Common Carotid Artery CT Angiography. Coronal Section Showing Pseudoaneurysm of the Common Carotid Artery CT Angiography. Sagital Section Showing Pseudoaneurysm of the Common Carotid Artery CT Angiography. 3D Reconstruction Showing Pseudoaneurysm of the Common Carotid Artery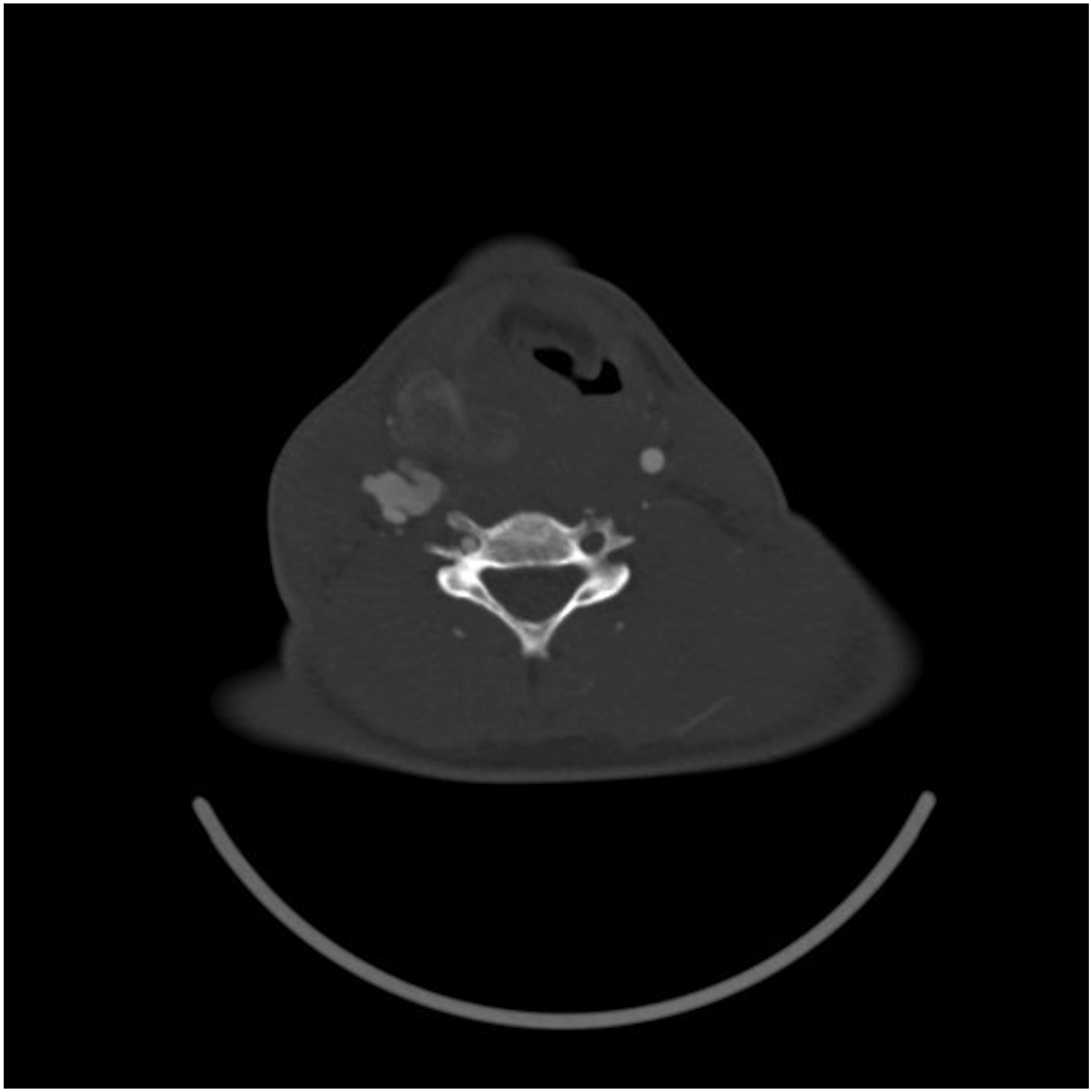
Treatment
Surgical treatment included right cervical exploration and end-to-end anastomosis of the right common carotid artery with interposition of a 6 mm straight ring-reinforced ePTFE graft. Intraoperative findings included a 6 mm pulsatile common carotid artery with a pseudoaneurysm in the mid-segment measuring approximately 2 × 2 cm. A 3 cm segment of the common carotid artery was resected, with good antegrade and retrograde flow observed. The graft was placed and found to be pulsatile. The internal jugular vein was intact, though tributary veins were avulsed and subsequently ligated and divided. Estimated blood loss was 200 cc. Heparin 5000 IU was administered, with a total vascular clamp time of 51 minutes. (Figure 5). End-to-end Anastomosis of the Right Common Carotid Artery With Interposition of a 6 mm Straight Ringed ePTFE Graft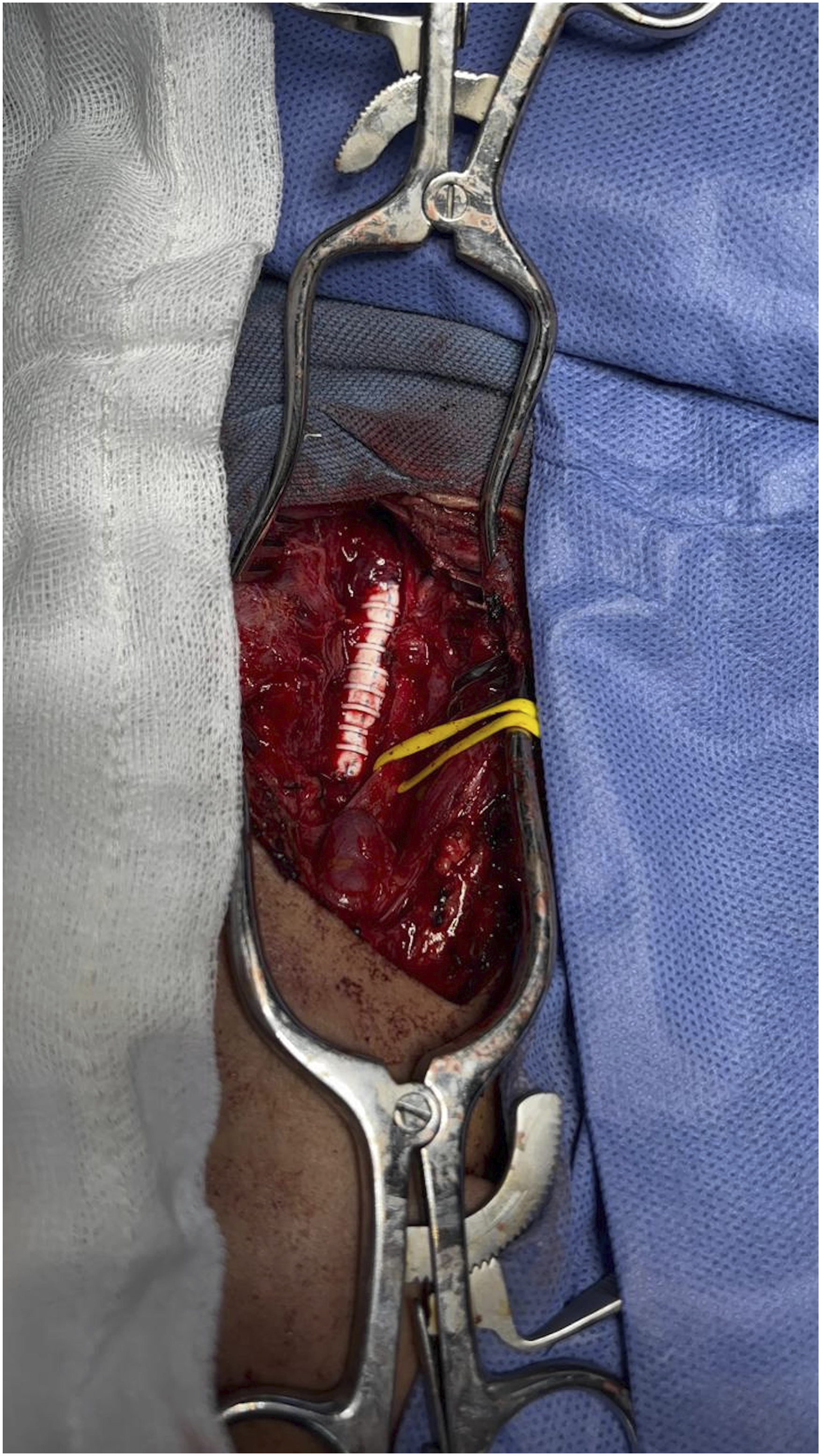
During the surgery, intraoperative electroencephalogram monitoring was conducted, by the anesthesiology team, and showed no significant abnormalities. In addition, strict blood pressure control was maintained throughout the procedure, and hypotension was avoided during clamping through the use of vasoactive agents.
As an intraoperative event, an emergency tracheostomy was performed due to difficulty with endotracheal intubation secondary to significant airway edema, as reported by the anesthesiology team.
Follow-Up
Postoperatively, the patient showed favorable evolution without focal neurological deficits or clinical deterioration. He was discharged on postoperative day 2 and transferred back to the General Hospital for continued management of multiple trauma and monitoring of the chest tube.
Outpatient follow-up showed satisfactory clinical progress.
Discussion
Cervical trauma may result from blunt or penetrating mechanisms (such as gunshot wounds, as in our patient) and can lead to arterial injury. Carotid artery injury occurs in approximately 3%-11% of penetrating neck traumas and accounts for about 3% of all traumatic arterial injuries.11,15 The mortality associated with traumatic carotid artery injury exceeds 40% 5 . Despite the high mortality rate, the patient described in this case survived the injury.
The most commonly affected segments are the common carotid artery, as in our case, and the internal carotid artery. 15
As previously mentioned, many patients with penetrating neck trauma have a high risk of mortality. However, among those who survive, like our patient, they may remain asymptomatic or present with a wide range of signs and symptoms, the most common being a pulsatile mass or pseudoaneurysm.1,7,9 In this case, the patient’s symptoms were mainly related to associated injuries such as clavicle fractures, limb and back wounds, and cervical edema secondary to trauma. Nonetheless, the pseudoaneurysm was identified during imaging as part of the trauma protocol, despite the absence of compressive symptoms at the time of diagnosis.
CT angiography was the diagnostic modality used at our institution, due to its accessibility and lower invasiveness compared to conventional angiography—the gold standard. CT angiography also has a high sensitivity (reported up to 100% for detecting aneurysms and pseudoaneurysms) and specificity of approximately 90%. 9 It typically shows a contrast-enhancing mass in continuity with the artery and visible contrast extravasation, as observed in our patient’s imaging, providing valuable information about the affected artery and surrounding structures. Other diagnostic modalities include Doppler ultrasound, magnetic resonance imaging (MRI), and conventional angiography.1,5,6,9
One of the most serious complications of pseudoaneurysms is rupture, which can be life-threatening. Therefore, prompt therapeutic intervention is essential once the diagnosis is established. Treatment depends on the nature and anatomy of the lesion as well as the patient’s clinical profile. Management options include conservative therapy, ultrasound guidance thrombin injection, open surgical repair, endovascular intervention, or a combined approach.1,4,5,7,8,13 Conservative management involves the use of anticoagulants, antiplatelet agents, and antihypertensives and is generally reserved for asymptomatic patients or small pseudoaneurysms.1,10,14
Endovascular techniques have gained importance in recent years for the treatment of this condition. Options include placement of bare-metal or covered stents and coil embolization, especially when cerebral perfusion is adequate.4,7–9,12 These approaches have shown favorable outcomes and are preferred in patients with high surgical risk, surgically inaccessible lesions, or hostile neck anatomy. 5
Traditionally, open surgical repair remains the treatment of choice for post-traumatic pseudoaneurysms, as was the case with our patient. 9 The first surgical management of an extracranial carotid aneurysm was performed in 1808 by Sir Astley Cooper, who ligated the common carotid artery—a technique now abandoned due to its high morbidity.5,7
Open surgical options include vessel clamping, resection with end-to-end anastomosis, resection with graft interposition (as performed in our case), extracranial-to-intracranial bypass, and carotid artery ligation.1,5,9 In our case, resection with interposition of a synthetic ePTFE graft was performed. According to the literature, synthetic grafts have a 5-year primary patency rate of 88.9%, compared to 66.4% for vein grafts. 5 Therefore, in patients with acceptable surgical risk and anatomically accessible lesions, synthetic graft interposition represents an excellent option.
The main factors influencing our decision to perform open repair were long-term survival of our patient and graft patency at a 5 years described in the literature. Additionally, whenthe patient arrived at our center and we were faced with a surgical emergency. In this case, The decision to use a synthetic graft was based on the fact that the surrounding veins (except for the internal jugular vein) were in poor condition due to the thermal damage caused by the bullet—some were even thrombosed. The major saphenous vein, after a rapid intraoperative bilateral limb venous scan, was found to have a diameter below the optimal threshold for use in bypass procedures. Additionally, the upper limbs veins were unsuitable due to the presence of multiple peripheral lines. Moreover, the patient was hemodynamically unstable, and a prompt repair was necessary.
In conclusion, although endovascular approaches continue to evolve and show promising results, open surgery remains a reliable and often preferred treatment modality depending on individual patient characteristics.
Conclusions
Post-traumatic carotid pseudoaneurysm remains a rare clinical entity. In our patient, the diagnosis was made following incidental detection on imaging performed shortly after sustaining gunshot wounds. This allowed for early identification and timely intervention, which helped prevent complications associated with the condition. Although endovascular treatment options are available, open surgical repair continues to be the cornerstone of management, particularly in young patients without significant surgical risk, as it offers favorable medium- and long-term patency rates.
Therefore, it is crucial to maintain a high index of suspicion for the development of carotid artery pseudoaneurysms following either open or closed trauma. Identify of the possible clinical presentations is essential to avoid missing the diagnosis, as delayed or missed treatment may represent a serious threat to the patient’s life.
Footnotes
Acknowledgments
The patient kindly gave verbal consent for the publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.