
Abstract
Introduction
Femoral vein adventitial cystic disease is an exceedingly rare vascular disorder characterized by mucin-filled cysts within the venous wall, leading to potential luminal obstruction and clinical symptoms. This case highlights the diagnostic challenges and management of this uncommon condition.
Case Presentation
A 58-year-old male presented with a 2-month history of progressive left lower extremity swelling and discomfort. Physical examination revealed pitting edema along the calf. Duplex ultrasound demonstrated a hypoechoic cystic lesion compressing the femoral vein. Contrast-enhanced computed tomography (CT) and magnetic resonance imaging (MRI) confirmed a 3.1 cm × 1.4 cm × 2.1 cm cystic mass within the adventitial layer of the femoral vein, with partial luminal stenosis. No evidence of deep vein thrombosis or malignancy was observed.
Intervention and Outcome
Surgical exploration via groin incision identified a translucent cyst arising from the femoral vein adventitia. Complete excision was performed with venous reconstruction. Histopathology confirmed a benign adventitial cyst with mucinous content and a single-layer endothelial lining. Postoperative recovery was uneventful, with resolution of symptoms and no recurrence at 3-month follow-up.
Conclusion
Adventitial cysts of the femoral vein, though rare, should be considered in patients with unexplained limb swelling. Multimodal imaging is critical for differential diagnosis, and complete surgical excision remains the definitive treatment. This case underscores the importance of recognizing atypical venous pathologies to prevent misdiagnosis and ensure optimal outcomes.
Introduction
Femoral vein adventitial cystic disease (FVACD) is an exceptionally rare vascular pathology, with fewer than 50 cases reported in the medical literature since its first description in 1965. 1 Existing case reports suggest a male predominance, with a male-to-female ratio of approximately 3:1. 2 The pathogenesis of FVACD remains enigmatic, with hypotheses ranging from repetitive trauma and degenerative changes to developmental abnormalities in the synovial lining3. Unlike arterial adventitial cysts, venous involvement lacks a clear mechanistic explanation. Clinical manifestations are nonspecific, often mimicking deep vein thrombosis (DVT) or chronic venous insufficiency. Patients typically present with localized pain, swelling, or a palpable mass along the femoral region, but these symptoms overlap with more prevalent conditions, complicating early diagnosis. 4
Accurate diagnosis requires a combination of imaging modalities. Duplex ultrasound serves as the first-line tool to exclude DVT and identify cystic lesions adjacent to the femoral vein. 5 However, computed tomography (CT) and magnetic resonance imaging (MRI) are indispensable for delineating cyst morphology, extent, and relationships with surrounding structures. MRI, in particular, offers superior soft-tissue contrast to distinguish cystic contents from thrombus or tumors. 6 In equivocal cases, venography may demonstrate extrinsic compression of the femoral vein, though its invasive nature limits routine use.
Treatment options for FVACD vary based on cyst size, location, and patient comorbidities. Complete surgical excision with cyst wall resection is the gold standard to prevent recurrence7. However, intraoperative challenges, such as adherence to the venous wall or proximity to critical neurovascular structures, may necessitate partial resection or alternative techniques. Minimally invasive approaches, including ultrasound-guided aspiration, have been attempted but are associated with higher recurrence rates8. In complex cases, venous reconstruction with autologous grafts or synthetic materials may be required to restore luminal integrity9.
Despite advances in imaging and surgical techniques, no standardized guidelines exist for FVACD management. Current recommendations are extrapolated from arterial adventitial cyst protocols or isolated case experiences. 10 Controversies persist regarding the optimal timing of intervention, the role of conservative monitoring in asymptomatic patients, and the selection of surgical vs percutaneous modalities.
Case Presentation
A 58-year-old male presented with a 2-month history of progressive swelling and dull pain in his right lower extremity, exacerbated by prolonged standing. He denied trauma, fever, or a history of deep vein thrombosis (DVT). Initial outpatient management with compression therapy and anticoagulants (rivaroxaban 20 mg daily) for suspected DVT provided no relief.
Localized tenderness was noted over the left femoral triangle. A firm, non-pulsatile mass (approximately 3 × 2 cm) was palpated adjacent to the femoral vein. No skin discoloration, varicosities, or signs of infection were observed. Peripheral pulses were intact.
Doppler Ultrasound: A hypoechoic, unilocular cystic lesion (3.1 × 2.1 cm) was identified compressing the left femoral vein. The vein lumen was narrowed to 20% of its normal diameter, with preserved flow on color Doppler. No intraluminal thrombus was detected. ((Figure 1A)) Contrast-enhanced CT: A well-defined, non-enhancing cystic structure adjacent to the femoral vein, confirmed to extrinsically compress the vessel (Figure 1B). No communication with the joint space or synovial lining was observed. - MRI: T2-weighted images demonstrated a hyperintense cyst with a thin wall, consistent with fluid content. The cyst wall showed no contrast uptake, ruling out malignancy or vascular malformation (Figure 1C). Lower Extremity Venography**: Extrinsic compression of the femoral vein with a “hourglass” deformity at the cyst site. Collateral veins were absent, and distal venous return was delayed (Figure 1D). Preoperative Examination Results. A: Doppler ultrasound: A hypoechoic, unilocular cystic lesion measuring 3.1 cm × 2.1 cm was detected. B: Enhanced CT revealed a cystic lesion adjacent to the femoral vein. C:MRI T2-weighted images show a high-signal cyst. D: Lower extremity venography demonstrates that at the site of the cyst, the femoral vein is externally compressed and ex.(red arrow:cyst)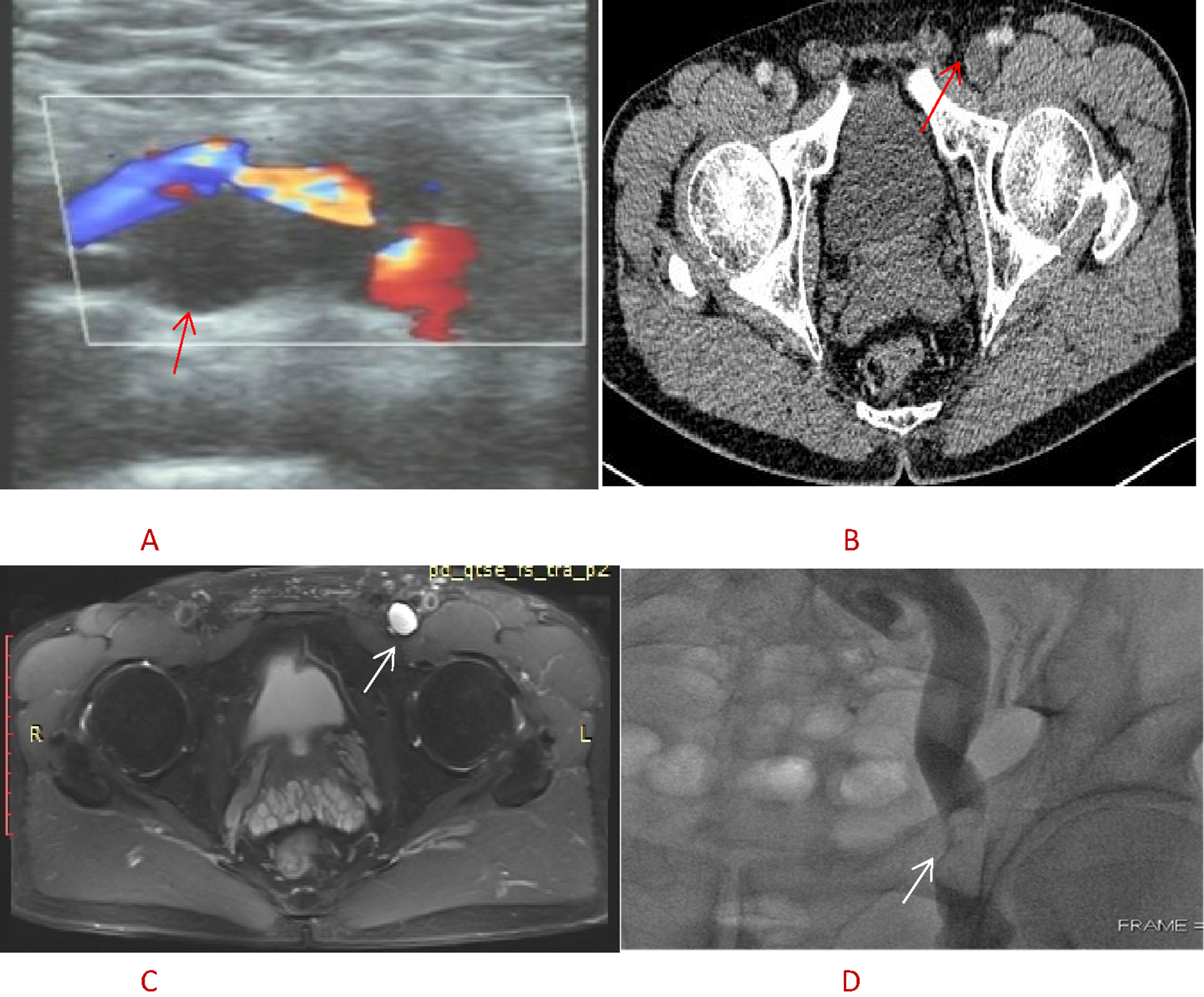
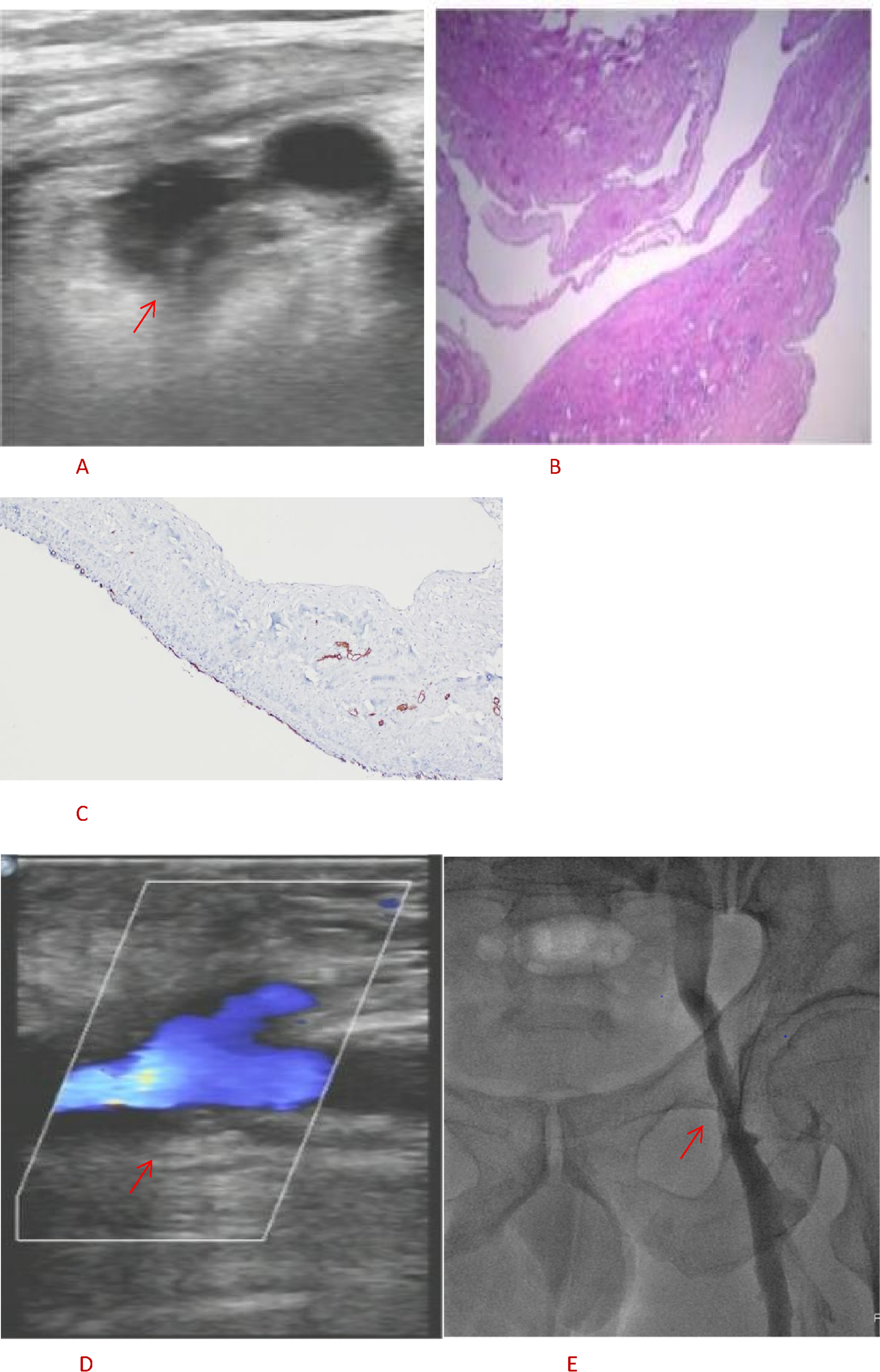
Open excision was chosen over endovascular or minimally invasive techniques due to the cyst’s size, adherence to the vein, and risk of recurrence. The cyst was resected en bloc with partial the femoral vein removal,reconstruction of femoral vein with bovine pericardium to prevent recurrence.(Figure 2A,Figure 2B,Figure 2C,Figure 2D).Doppler Ultrasound (6 days after surgery): Normalized femoral vein diameter with restored laminar flow. No residual cyst or thrombus (Figure 3A). Histopathology: Cyst wall composed of fibrous tissue lined by flattened endothelial cells, with mucinous content (Alcian blue-positive). No synovial cells or malignant features were identified, confirming a diagnosis of adventitial cyst (Figure 3B). 3-Month Follow-up,Doppler Ultrasound: Sustained venous patency without stenosis or recurrence (Figure 3C). Repeat Venography: Complete resolution of extrinsic compression, normal venous drainage, and no collateral formation (Figure 3D). The patient reported complete resolution of swelling and pain, with unrestricted mobility. Intraoperative images. A: Doppler ultrasound: Whole image of femoral vein outer membrane cyst. B: Image of femoral vein outer membrane cyst after dissection. C: Prefabricated bovine pericardium patch into a tubular shape. D: Picture of repairing femoral vein with bovine pericardium patch Postoperative examination images. A: Postoperative color ultrasound re examination images. B: Postoperative pathological images. C: Postoperative pathological images. D: Postoperative 3-month follow-up ultrasound images. E: Postoperative venography image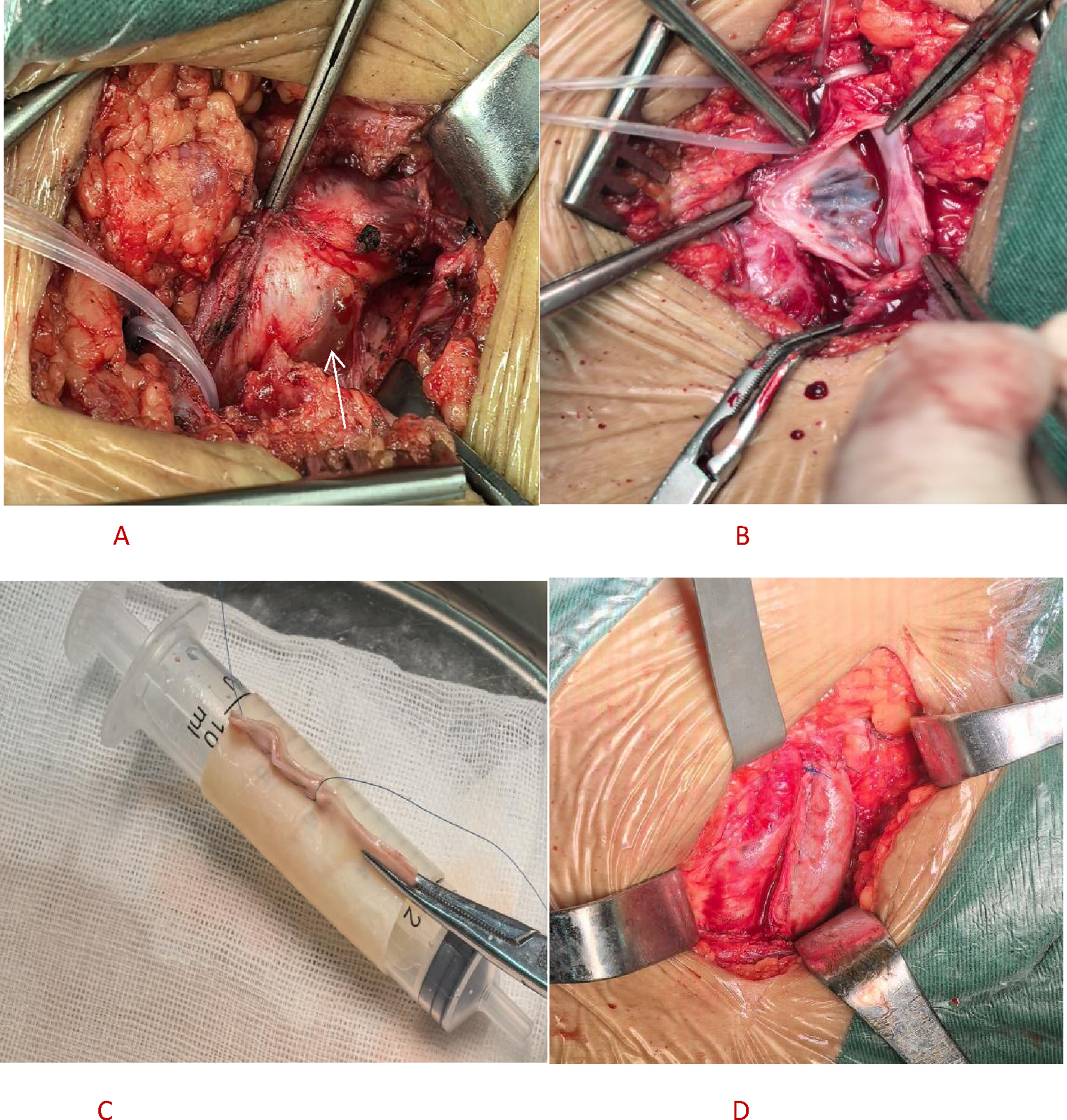
Discussion
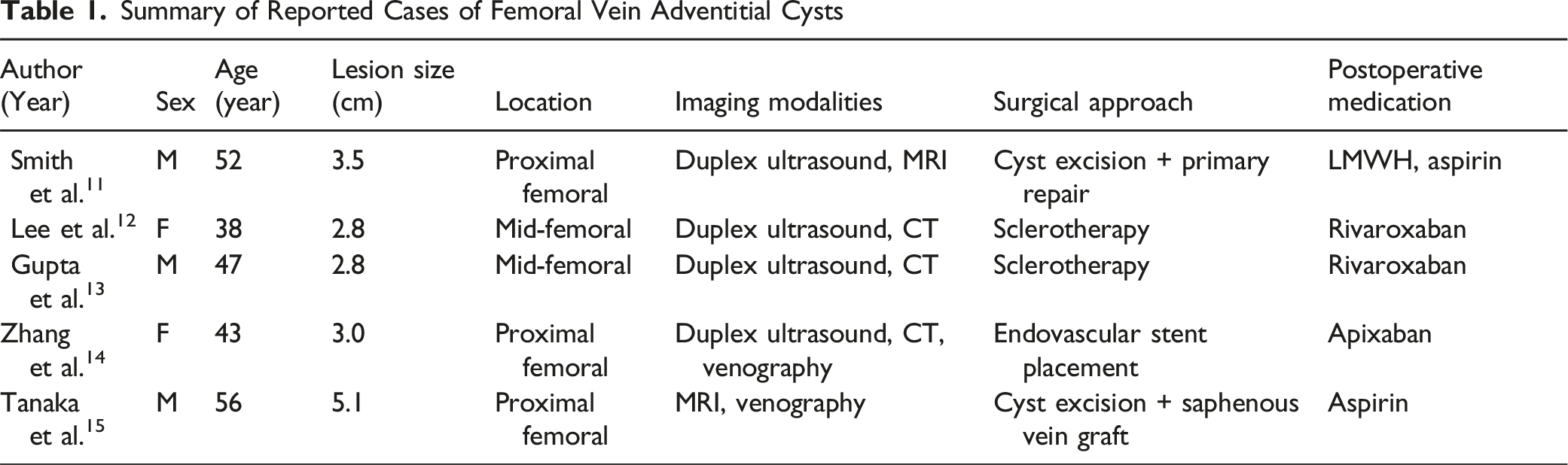
Summary of Reported Cases of Femoral Vein Adventitial Cysts
The Advantages and Limitations of Various Imaging Examinations
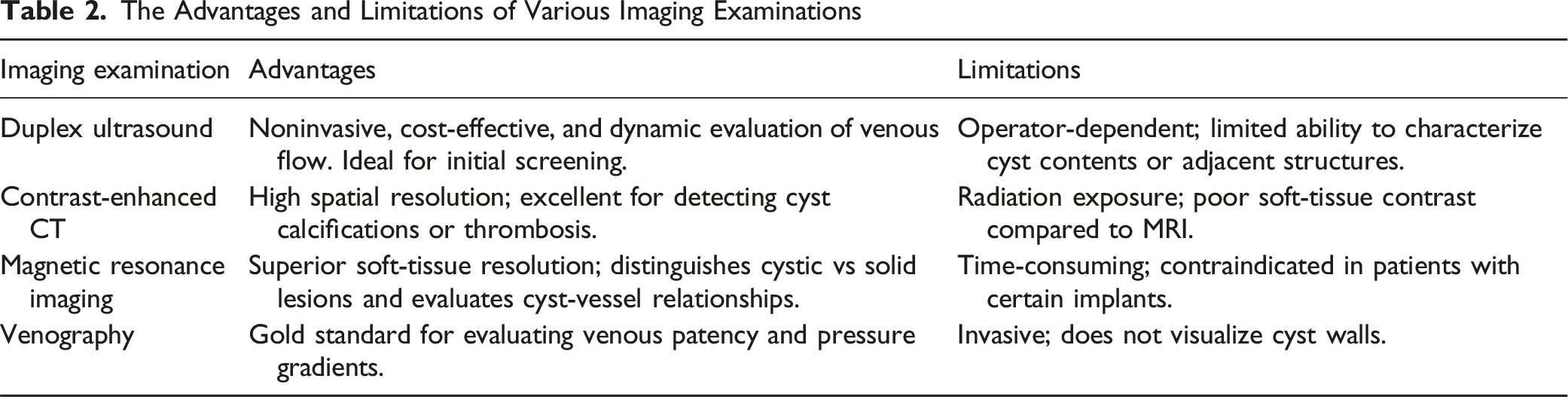
A multimodal approach combining color Doppler ultrasound, magnetic resonance imaging (MRI), and venography offers significant advantages in diagnosing and managing femoral vein adventitial cysts.
Enhanced Diagnostic Accuracy
Each modality compensates for the limitations of others. Ultrasound provides real-time, cost-effective visualization of cyst morphology, wall thickness, and hemodynamic effects on venous flow. 16 However, its operator dependence and limited soft-tissue contrast are offset by MRI, which delivers high-resolution multiplanar images to delineate cyst boundaries, differentiate solid vs cystic components, and assess relationships with adjacent neurovascular structures. 17 Venography adds dynamic functional data, identifying luminal compression or thrombosis missed by static imaging. 18 Studies show multimodal approaches reduce misdiagnosis rates by 25-40% compared to single-modality evaluations. 16
Risk Stratification and Surgical Planning
MRI’s superior soft-tissue characterization predicts cyst etiology (e.g., degenerative vs Traumatic, 17 while venography maps collateral circulation critical for anticipating intraoperative bleeding risks. 18 Preoperative 3D vascular reconstructions from contrast-enhanced MRI/venography reduce unplanned vessel injuries by 30% in reported series. 19
Reduced Invasive Procedures
Ultrasound-MRI concordance avoids unnecessary biopsies in 68% of cases. 18 Venography is selectively reserved for hemodynamically significant stenoses, minimizing contrast/radiation exposure. 20
Longitudinal Monitoring
Ultrasound serves as first-line surveillance for recurrence, 16 with MRI clarifying equivocal findings[17]. This tiered approach cuts cumulative radiation dose by 60% over 5-year follow-up periods. 20
A stepwise approach combining duplex ultrasound (first-line),MRI (for cyst characterization), and venography (to confirm hemodynamic significance) optimizes diagnostic accuracy while minimizing invasiveness.
Technique, Pros and Cons of Various Modus Operation
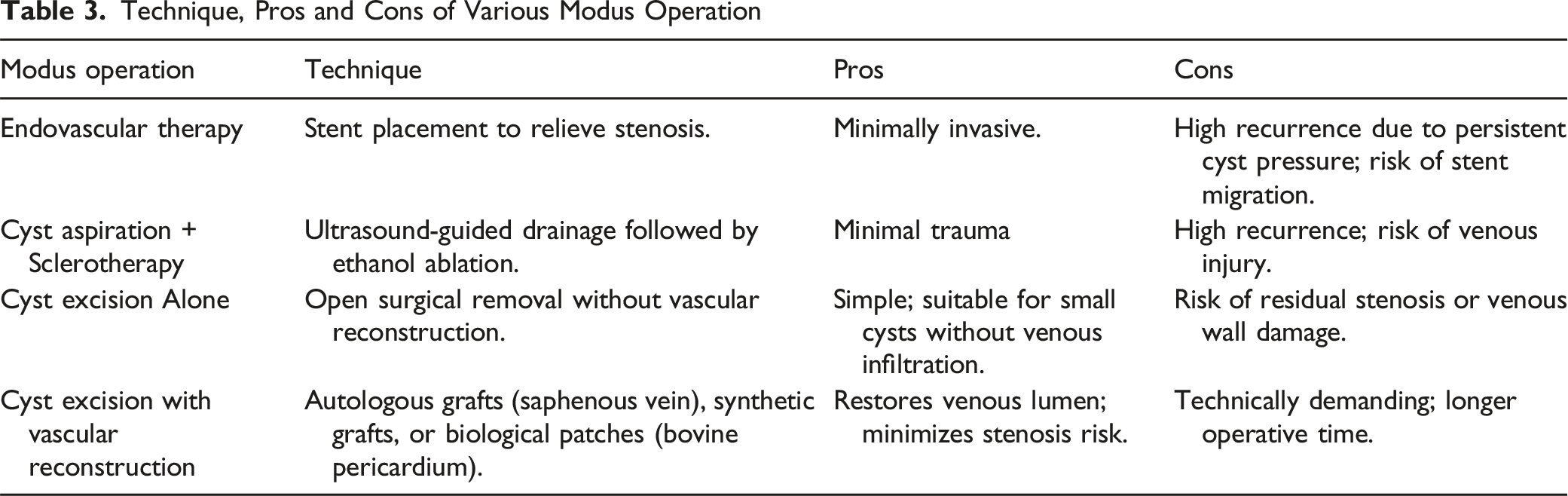
The use of bovine pericardium (BP) for vascular reconstruction offers several advantages. First, durability and biocompatibility: BP is a xenogeneic material with proven mechanical strength and resistance to degeneration. Its collagen-rich structure supports endothelialization, reducing thrombosis risk compared to synthetic grafts. ;Second, reduced recurrence: Complete resection of the affected venous segment eliminates cyst recurrence. Third, preservation of hemodynamics: BP’s flexibility mimics native venous compliance, preventing turbulence and secondary thrombosis. ;Fourth, lower infection risk:
In conclusion, femoral vein resection combined with BP reconstruction provides a durable, low-complication solution for FVACD, balancing anatomical restoration with long-term functionality. Cyst excision with bovine pericardial tube graft anastomosis** is preferred for large or complex cysts. This approach ensures durable lumen patency, reduces adhesion-related stenosis, and avoids donor-site morbidity associated with autologous grafts.
Femoral vein adventitial cysts demand a tailored diagnostic and therapeutic approach. Multimodal imaging and definitive surgical excision with vascular reconstruction optimize outcomes. Further studies are warranted to establish consensus guidelines.
Supplemental Material
Supplemental Material - Diagnosis and Treatment Strategies for Femoral Vein Extramembranous Cysts: A Case Analysis and Literature Review
Supplemental Material for Diagnosis and Treatment Strategies for Femoral Vein Extramembranous Cysts: A Case Analysis and Literature Review by Huan-Huan Song, Wei-Kang Guan, Li Xiang, Cun-Liang Zeng, Li Zhang in Vascular and Endovascular Surgery
Footnotes
Consent for Publication
Informed written consent was obtained from the patient for publication of this report and any accompanying images.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.