
Abstract
Although some people with spinal cord injury (SCI) return to outdoor recreation, many have low activity levels and encounter significant environmental barriers. The purpose of the study was to describe how people with SCI engage in outdoor recreation activities, what meaning they attribute to these, and to inform occupational therapists in promoting outdoor recreation post-SCI. The study used qualitative, descriptive phenomenology. Thirteen participants completed semi-structured interviews, and data were analyzed using thematic analysis. Outdoor recreation contributes to personal well-being. It is a way to share life with loved ones and other disabled people. Having the right equipment and using a trial-and-error approach facilitated participation, which was sometimes supported and frequently constrained by physical, built, and information environments. Findings suggest implications for occupational therapists in the areas of direct intervention, entrepreneurship, and advocacy. These are consistent with the American Occupational Therapy Association Vision 2025 to collaborate for inclusion and accessibility in occupational performance.
An estimated 18,000 people each year in the United States sustain a traumatic injury or damage to the spinal cord, often resulting in permanent full or partial paralysis below the level of the injury (National Spinal Cord Injury Statistical Center, 2020). People living with SCI experience loss of motor and sensory functions and immediate mobility limitations impacting all areas of life from daily self-care to accessing work, social, and community spaces, and participating in leisure activities. Results of an early study conducted by Carpenter and Clark (1994) described SCI as creating a split between the changed external self and the unchanged internal self, and it is well understood that recovery is not only physical, but mental, emotional, and social as well (Menzies et al., 2021; Price et al., 2011; Williams et al., 2014).
Inactivity After SCI
While learning to live with an SCI is highly individual, people who were physically active prior to their injuries often become physically inactive, tending to participate in passive indoor rather than active outdoor leisure activities. Forty-four to 50% of previously active people with SCI engage in very little leisure time physical activity (Eitivipart et al., 2022; Martin Ginis et al., 2010; Rocchi et al., 2017). This represents a significant loss of previously enjoyed leisure time and outdoor physical activity, as well as a potential health risk.
A sedentary lifestyle presents a significant health risk for all people (Center for Disease Control and Prevention, 2022). There is an additional risk for those with SCI since mortality statistics indicate that respiratory complications and infectious diseases are the most common causes of death (National Spinal Cord Injury Statistical Center, 2020). Physical activity improves cardiovascular health, supports immune function, and may mitigate the secondary conditions associated with SCI such as deep vein thrombosis and osteoporosis (World Health Organization, 2013).
Outdoor Recreation Definition
Outdoor recreation is leisure-time physical activity that takes place outdoors or in nature. Leisure time physical activity (LTPA) includes all of the behaviors associated with physical activity that people choose to take part in voluntarily (Steinbach & Graf, 2008). Outdoor recreation was chosen for this study because it has been shown to result in more engagement, well-being, and decreased tension than indoor physical activity alone (Thompson Coon et al., 2011).
Benefits of Outdoor Recreation After SCI
Some people return to previously meaningful outdoor recreation activities or take up new ones, and there are many programs providing a wide variety of adapted recreation opportunities such as archery, canoeing, fishing, sailing, sea kayaking, scuba diving, skating, skiing, swimming, surfing, and hiking. Several qualitative studies have previously demonstrated how outdoor and LTPA can promote a sense of community, build self-determination, and improve well-being for people with SCI.
People who participate in outdoor recreation report a sense of community and social support. Some attribute their ongoing participation to interacting with others which gave meaning to the physical activity (Luchauer & Shurtleff, 2015). Outdoor group activities that require people to rely on one another to succeed, such as scuba diving, restore a sense of contribution for people with SCI who experienced social isolation after injury (Carin-Levy & Jones, 2007).
Outdoor recreation is meaningful because people value how their sense of identity and self-concept grow as a result of mastering challenging tasks (Boyce & Fleming-Castaldy, 2012; Williams et al., 2014). It provides the opportunity to build self-determination by accomplishing goals in the context of enjoyable activities. People who return to previously valued outdoor recreation post-SCI also experience a sense of competence and improved self-esteem (Boyce & Fleming-Castaldy, 2012; Ekelman et al., 2017).
Physical activity, being in nature, and outdoor recreation are all associated with improved mood and well-being. Physical activity for people with physical disabilities including SCI has been found to improve mood and quality of life (Battalio et al., 2020). Finally, outdoor recreation is reported by wheelchair users to improve quality of life and well-being (Menzies et al., 2021).
Barriers to Outdoor Recreation After SCI
A number of barriers to outdoor recreation after SCI have been described, including environmental and personal barriers which limit participation. Environmental barriers include high costs for adapted equipment and specialized training, limited access to programs providing adapted activities, and limited accessibility to outdoor recreation spaces. The lifetime costs associated with having a SCI range from one to five million dollars depending on medical care and equipment needs, not counting specialized adapted equipment needed for many forms of outdoor recreation (National Spinal Cord Injury Statistical Center, 2020). Previous studies have found that financial resources were a significant limitation to engagement in LTPA and outdoor recreation (Hwang et al., 2016; Menzies et al., 2021). In addition to difficulty affording equipment and training individually, the high costs associated with paying for travel and fees to participate in adapted outdoor recreation programs have also been identified as barriers to participation (Williams et al., 2014). The study by Hwang et al. (2016) found that some people with SCI were unaware of these programs. Many qualitative studies have found that a significant barrier to outdoor recreation is the lack of accessibility even in spaces meeting ADA Standards for Accessible Design (n.d.; Corazon et al., 2019; Menzies et al., 2021; Williams et al., 2014).
The personal barriers to outdoor recreation include the areas of personal skills, pain, time use, and feelings of exclusion. Matching a person’s bodily characteristics with the activity they want to do can be complex and require skilled support and accommodations (Hwang et al., 2016). Time was found to be a barrier in terms of scheduling the time needed either due to additional time for using adapted equipment or not having enough time in addition to the demands of activities of daily living (Hwang et al., 2016; Williams et al., 2014). Finally, feelings of exclusion, outsideness, and lacking societal support were reported as barriers to outdoor recreation (Williams et al., 2014). In both the studies by Hwang et al. (2016) and the meta-analysis by Williams et al. (2014), results demonstrated that people with SCI who experienced more barriers to LTPA had lower levels of participation in LTPA.
Person, Environment, Occupation Model
The theoretical framework that informs this study is the Person, Environment, Occupation (PEO) Model (Law et al., 1996). Being an occupation-based model that focuses on the transactional relationships between a person, environments, and occupations the PEO Model situates occupational performance at the dynamic intersection of these domains. Using the PEO, participation in outdoor recreation results from the complex interactions between a person’s own choices and abilities; the characteristics and demands of the activities themselves; and the specific environments in which the people engage in the activities.
Purpose
Although it is known that some people with SCI return to outdoor recreation post-injury that there are many forms of adapted outdoor recreation available, and that physical and outdoor activity is related to improved overall health, it is also known that LTPA levels are very low and there are significant barriers for people living with SCI. Further description of how and why people with SCI engage in outdoor recreation may inform OTs working with this population. The purpose of the study was to describe how people with SCI engage in outdoor recreation activities, and what meaning it has for them. The central research question for the study was:
Research Question 1 (RQ1): What is the meaning and experience of people with SCI who regularly participate in outdoor recreation?
Method
We designed this study with qualitative methodology using a descriptive phenomenological approach. Phenomenological studies describe the shared experiences and meanings of a particular phenomenon (Creswell & Poth, 2018). The inclusion criteria included English-speaking adults with any level of spinal cord injury who regularly participate in outdoor recreation activities. This was defined by participating at least three times in the past year. The amount of required participation was low because the data were collected in the fall of 2020, about 8 months into the start of the COVID-19 pandemic closures. Each participant completed a 1-hr semi-structured interview. The study design and report follow the Standards for Reporting Qualitative Research (O’Brien et al., 2014).
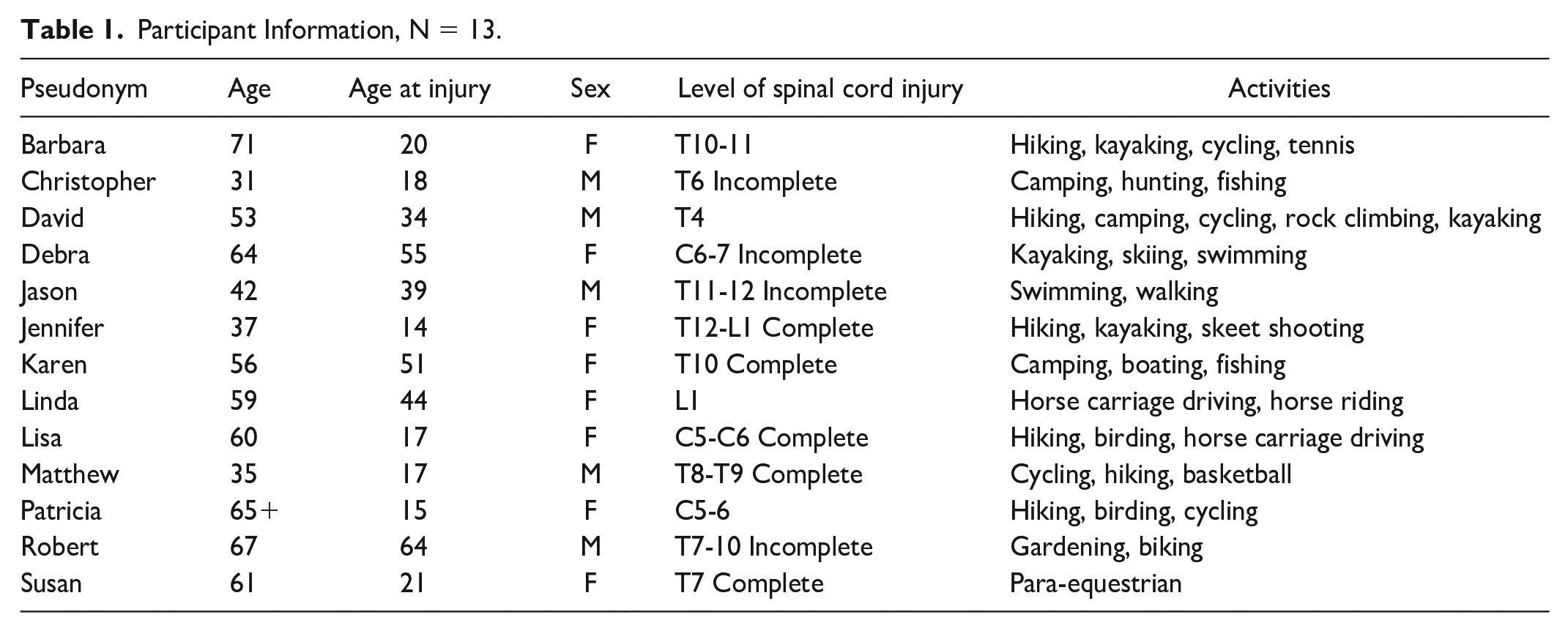
Thirteen participants were recruited via convenience sampling from four online SCI support and activity groups. See Table 1 for participant information. All of the participants are White and Christopher is Hispanic. All participants were living in the United States at the time of the interviews. Participants ranged in age from 31 to 71 years old (median age = 59), had sustained their injuries between ages 14 and 64 (median age = 21), and had been living with SCI for 3 to 51 years (median years = 18.5).
Participant Information, N = 13.
This study was approved by the Institutional Review Board at California State University Dominguez Hills, #21-016. All participants provided informed consent. The interviews were recorded and transcribed via Zoom. Data were de-identified and stored securely in Dropbox. Participants received a small monetary incentive for participation, which was funded by an internal grant.
We analyzed the data using thematic analysis as described by Braun and Clark (2006). First, each investigator read through the transcripts noting initial ideas, followed by generating initial codes. Investigators used triangulation by defining shared terms and coming to consensus on the coding scheme. This was followed by grouping codes which led to the identification of themes to answer RQ1. Defining and naming the themes followed an iterative process until final themes reflected the research question and available data.
None of the investigators has sustained a SCI or have another physical disability. To mitigate for researcher biases, the team created a reflexivity plan prior to conducting this study which included bracketing pre-existing assumptions and becoming familiar with narratives of disabled advocates via their online materials and public social media posts. In addition, interviews were semi-structured with open-ended questions. Participants were reminded that they could pause or end the interview at any time.
Results
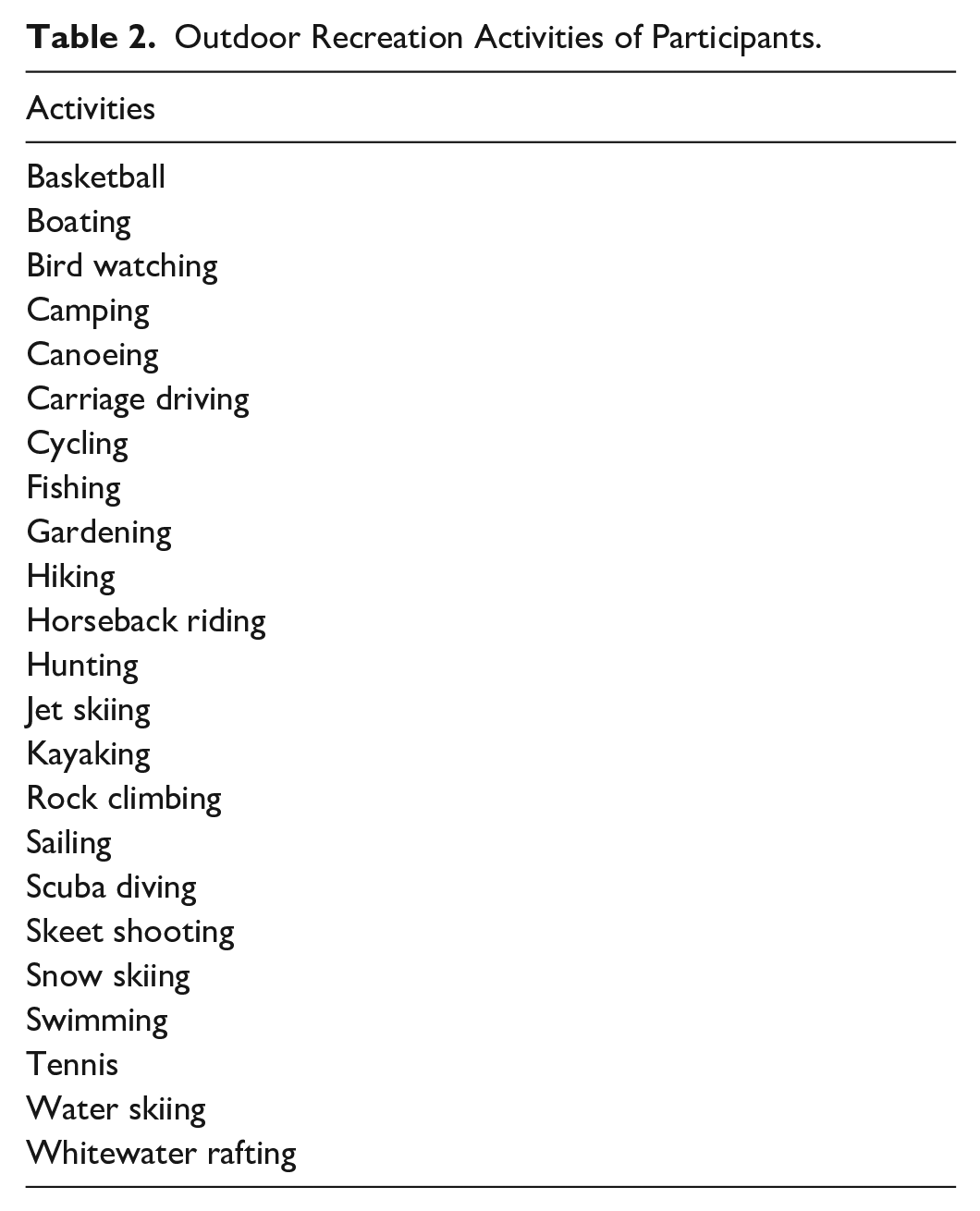
The themes that emerged are that outdoor recreation post-SCI contributes to personal well-being and a sense of self. It is a way to share life with loved ones and other disabled people. Participants identified over 20 activities that they engage in, commonly with adaptations (see Table 2). Outdoor recreation for people post-SCI was either supported or constrained by physical, built, and information environments.
Outdoor Recreation Activities of Participants.
Personal Health and Meaning
The personal meaning of outdoor recreation resonated strongly with participants. For many, the physical aspects of health, fitness, and learning to trust and live in their own changed bodies gave meaning to their outdoor recreation activities. Participants used phrases such as “good exercise,” “invigorating,” and feeling “healthier” to describe the benefits. Linda discussed that horseback riding gave her the opportunity to stretch her legs in a position that her wheelchair did not allow. Besides the direct physical benefits, Patricia shared, “Being out there in the world is really where you’re going to get those skills for how to be in the world in a different body.”
It took varying amounts of time for participants to engage in outdoor recreation activities after their injuries, and most needed to address their fear of falling in the process. Matthew started playing competitive basketball and bicycle racing soon after his injury at age 17. Barbara described that she was injured in an accident coming back from a ski trip and did not try skiing again for 15 years, despite regular family vacations at a lodge that had an adaptive skiing program.
Return to Previously Meaningful Occupations
A consistent and salient theme among participants was their identity as being active and athletic prior to their injuries and re-connecting with this part of themselves through outdoor recreation. As Patricia explained, “I don’t think people change at their core or what they were interested in before—it is just a matter of finding out how to manifest that in a different way.” Jennifer, who enjoys hiking, said: Nature has always been really important in my life. I grew up camping and hiking. My dad was a park ranger. And so I—me and my sisters—we grew up having a respect for nature and appreciation for nature.
For some it wasn’t the activity that was as important as the experience of pleasure and enjoyment. Having been athletic prior to her injury, Patricia tried a variety of sports until finding that, “it was cycling that really gave me that same kind of sense of enjoyment and thrill as when I wasn’t disabled.”
Freedom, Confidence, and Well-Being
Outdoor recreation allowed people to test their limits and abilities and provided a sense of accomplishment. David expressed how he encountered difficult situations in nature that built his confidence: “It’s cold. It’s wet. It’s abrasive. My arms hurt. I’m scared—and then the next day you’re like, ‘Huh. I’m glad I did that. That was pretty cool.’” Jennifer, who takes the risk of hiking alone, described the importance of participating in challenging outdoor recreation activities, saying, “I gotta stretch my boundaries, I gotta test those limits a little bit. Otherwise, I’m not going to be myself, I’m not going to be human.”
Sometimes the sense of freedom and autonomy had to do with not needing specialized equipment to participate, such as Debra feeling liberated by not needing any adaptive equipment to kayak and Jennifer feeling “normal” when floating in the ocean without her wheelchair. For others, having specialized equipment was what made the activities possible. Christopher described how his track power wheelchair allowed him to reach the edge of a river and fly fish. With or without adapted equipment, participants expressed the importance of finding the joy they previously had in outdoor recreation. Susan expressed the challenge of having to participate differently post-SCI, but reflected: I said—you know—get past the ego part and just try to resurrect that joy that was in your heart when you remember doing it. And you know—it doesn’t die within you. So, it’s resurrecting that joy that some of those things bring back to you.
The sense of well-being included both being outside and engaging in recreation.
Participants expressed the benefits of recreating outdoors in terms such as “rejuvenating,” “calming,” “healing,” and described it as a means to “get away from everyday life.” Linda explained that: So many people who are disabled are really restricted to a small vicinity. Or restricted by transportation issues or money issues or—you know—many things. . . And I know for me and my other friends who are disabled, who are out in nature a lot, it just kind of helps.
David described this sense of being part of something bigger than himself when he said, “[Getting outdoors] gives you a place to feel like you’re in a larger space and connected to a larger thing and your life consists of more than the medical apparatus around you.”
Being active outdoors provided a strong sense of well-being, freedom, confidence, and identity.
Social Relationships and Meaning
Several participants expressed that outdoor activities were not a part of their initial rehabilitation process post-injury, but it was their friends, family, or adapted recreation programs that enabled their engagement in outdoor activities. Most participants chose to participate in outdoor recreation when there was someone there to assist. They valued their participation because it allowed for them to share life with family and friends and get to know other disabled people.
Someone to Assist
Many participants reported that help from their family and friends enabled them to participate in outdoor recreation. Debra stated that her husband helps her engage in hiking and kayaking saying, “He calls himself the ‘camp director’ because without him, I wouldn’t be doing most of these activities.” Christopher reported that he camps with his family for both togetherness and to have assistance. He said, “I still do need some assistance to be able to transfer back into my track chair or onto my ATV.”
Some participants shared experiences they had when they did not have immediate access to assistance. Susan fell out of her wheelchair and would not have been able to get back in if someone had not stopped to help her. Although Jennifer hikes alone and doesn’t always plan ahead for assistance, she trusts that someone will assist in the moment if needed.
Sharing Life
In addition to having someone to assist, participants reported that they value sharing life with their friends, family, and loved ones by doing activities together. A significant part of the meaning of outdoor recreation included sharing life experiences, as in Christopher’s words: Being able to go out to an area and that place being accessible enough for me to be able to go up to a river, for example, so I can still fish from that river holds a lot of value to me—Just being able to teach my son and my daughter and my wife how to fish in a river or stream.
Similarly, Barbara talked about bicycling with her son’s family and kayaking with her niece. In these ways, being able to participate in outdoor recreation was described as a meaningful way to share life with others.
Community With Other Disabled People
Many participants indicated that outdoor recreation helped them get to know other disabled people and be part of the disabled community. Several took a leadership role to encourage others to get involved in outdoor recreation. Barbara recalled that wheelchair sports were a way to get to know other disabled people, saying, “tennis and basketball and rugby and whatever else helps you to socialize with other wheelchair users.” Matthew shared that he tries to connect people who have newly acquired SCI to a local outdoor recreation group he started, saying, “I want to be able to share with others because it may be something that really touches home with somebody, and [they] say, ‘Hey, you know, I could really do that too.’” He also shared that many with newly acquired SCI are not initially ready for his resources but join later. Similarly, David explained that he advises others with SCI to get outside, even if it is exploring their neighborhood, saying, “because I find that when you walk with a friend or something, you end up talking about your entire life.” The interpersonal environments of having someone to assist, sharing life, and being with other disabled people were described by participants as central parts of their participation in outdoor recreation.
Physical, Built, and Information Environments
Participants consistently spoke about how the physical, built, and information environments either enabled or constrained their participation. Although they experience numerous benefits from specialized programs or adaptive equipment, barriers include high costs of programs and equipment, distance to access programs, and difficulty finding needed accessibility information ahead of time.
Adapted Programs
Specialized programs provide equipment and training for activities such as skiing and horseback riding. Barbara shared about a camp program where she learned what to do when a kayak flipped over, and she can now kayak elsewhere as well. Other participants reported traveling for programs, as well as being part of local adapted recreation programs such as hand cycling, basketball, or carriage driving.
Several participants started or joined the leadership of adapted recreation programs. Matthew started his own organization providing group adapted outdoor recreation activities. Lisa and Patricia co-founded an inclusive dance company. Patricia advocates for disability rights on advisory boards and as the founder of a non-profit specializing in accessible recreation.
At the time of the interviews, many programs had not resumed their event programming due to the COVID-19 pandemic. Although many participants continued their outdoor recreation with members of their own household, they were limited due to public area closures.
Participants were quick to note that the cost and distance of these programs can be prohibitive for disabled people who may be unable to continue their careers and live on tight budgets. Patricia explained: I think one of the hardest parts for people is that they don’t have access to these [programs]. How does someone that doesn’t have transportation or live in an area that doesn’t have public transit get there? It has always bothered me that we would go and say, “Oh yeah, you can go cycling.” And then it’s like, but where do I get to do that? “Oh, you have to travel 70 miles and come.” That’s the hard part.
The Right Equipment
Participants frequently described the joy of having appropriate adapted equipment to access outdoor environments, including hand cycles, power wheelchairs, track power wheelchairs, beach wheelchairs, sports wheelchairs, and adapted vehicles. They described the equipment with enthusiasm for the freedom these allowed. Debra uses a beach wheelchair to reach the double kayak she paddles with her husband. Some participants sought out programs that provide equipment rather than purchasing it, and others who had purchased equipment noted that the cost is prohibitive for many others.
Trial-and-Error
Participants used a trial-and-error approach when engaging in outdoor recreation due to the frequent lack of available information ahead of time and actual accessibility on-site.
Participants who enjoy hiking shared how difficult it is to find accessible trails and obtain the information they need prior to arrival. Linda described these frustrations, saying “It’s the fact that so many trails that could be accessible—easily accessible—aren’t. Or it’s very difficult to get information about what is and what isn’t.” Linda, Jennifer, and David shared that the information on websites often does not provide the details they need to know ahead of time. David reported it is difficult to find enjoyable ADA compliant trails because they tend to be easy and short, so he uses topographical maps instead. Linda concluded, “I tend to find places around home that I know work well and frequent those places,” to avoid the frustration of showing up and not being able to participate.
Having experienced the barrier of not being able to find accessibility information ahead of time, Jennifer created a website with detailed firsthand hiking and travel accessibility information. She explained how she needed to know the length, width, and make-up of trails, whether there were accessible bathrooms along the way, where water is located, and how to get more information. She also described that knowing where picnic tables, benches, or scenic views are can be used to plan for different amounts of strength, time, or energy and still having an enjoyable experience. She emphasized that websites and on-site signage are frequently lacking needed details and has created her own website in response.
Discussion
The purpose of this qualitative, phenomenological study was to describe how people with SCI engage in outdoor recreation activities, and what meaning it has for them. Findings indicate that our participants engage in a variety of outdoor recreation pursuits for their own personal health, that it brings a sense of freedom and well-being, and that it provides continuity and return to meaningful activities. Participants share outdoor recreation with others, often involving someone to provide assistance, but also because it is a meaningful way to share life with friends and family as well as meet other disabled people. Physical, built, and information environments present variable access to outdoor recreation. Having financial, transportation, and geographical access to specialized adapted equipment and programs for outdoor recreation enables participation, while participants encounter constraints in built, physical, and information environments requiring a trial-and-error approach.
Related to Previous Literature
Similar to previous studies, our findings demonstrate that people with SCI participate in many forms of outdoor recreation including informal, program-based, local, and destination (Menzies et al., 2021). Participants found a sense of congruence in returning to activities that they previously enjoyed or that provided a similar feeling (Menzies et al., 2021; Williams et al., 2014). Outdoor recreation provided not only physical activity but also a sense of mental, social, and emotional well-being (Ekelman et al., 2017; Luchauer & Shurtleff, 2015). Findings from this study describe the social benefits as including both sharing life with loved ones and meeting other disabled people in the context of outdoor recreation.
The distance and cost constraints of outdoor recreation that have been previously identified are further described by our findings. Menzies et al. (2021) described the need for new adaptations, advocacy, and affordable equipment and programs in Canada. Our findings reflect the same needs in the United States. Participants identified many types of adapted equipment, notably specialized wheelchairs for outdoor recreation that make their participation possible. They associated strong emotions such as elation and relief with using equipment that could sufficiently manage the physical barriers.
Physical accessibility barriers are a consistent finding in studies assessing outdoor and LTPA for wheeled mobility users (Menzies et al., 2021; Williams et al., 2014). Our participants reported similar barriers and additionally discussed the lack of information available to them regarding the accessibility of outdoor recreation spaces. Hwang et al. (2016) found that participants lacked awareness of adapted recreational opportunities. Our participants discussed not being able to find information about accessibility even when actively searching for it, for informal local and destination trip planning. This led to needing to use a trial-and-error approach, creating their own online resources for others, and starting their own recreation programs. Some were tired of solving problems and tended to stay in known vicinities.
Related to PEO Theory
Participants in this study were active in outdoor recreation, demonstrating strong overlap between the person, environment, and occupation elements of occupational performance in the PEO Model (Law et al., 1996). See Figure 1 for a taxonomy of the themes as they relate to the PEO dimensions of occupational performance. Although the personal meanings developed over time, these were relatively stable in participants’ narratives. Similarly, the social environment of participating with others also developed over time but was discussed as a relatively stable aspect of their participation.
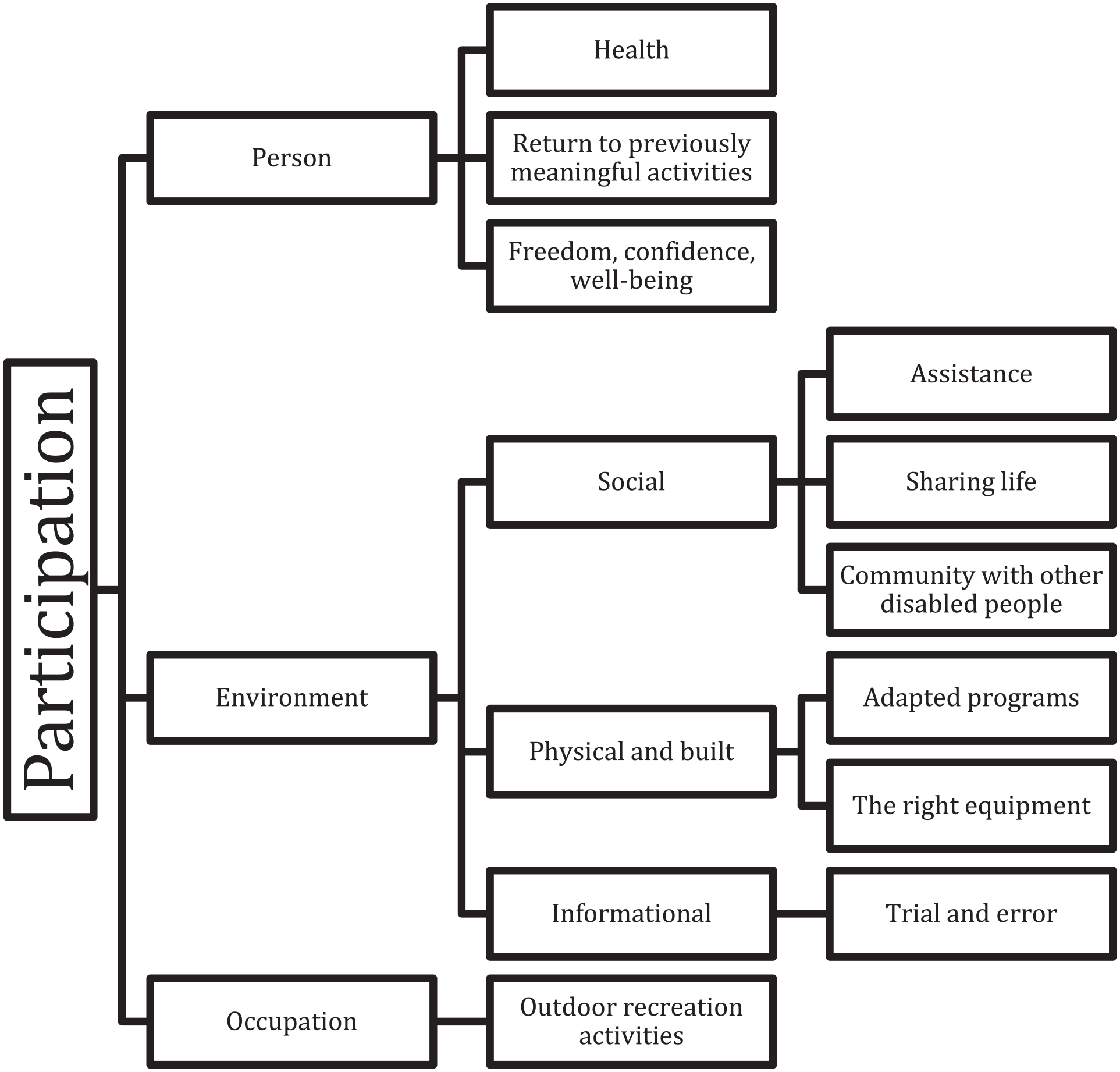
Taxonomy of Themes Using PEO Model.
The dimension that most constrained occupational performance was the variable and often unpredictable accessibility in physical, built, and information environments. Many outdoor physical environments are only accessible with the use of specialized equipment that is only available to those who can afford it or live near enough to attend a program that offers it. Built environments such as ADA compliant hiking trails are often limited in scope leaving people wanting a more inclusive or immersive experience. Participants coped with these constraints by leveraging their resources, locations, and trial-and-error persistence to enable participation in otherwise inaccessible physical, built, and information environments.
Limitations
Due to the convenience sampling method, participants in this sample were limited in terms of diversity in age, race, ethnicity, and level of SCI. Our sample consisted of mainly older people (median age = 59) with SCI who had sustained their injuries a long time ago (median age = 21). One participant was Hispanic. All participants had sustained a SCI between C5 and L1, with only three participants sustaining an injury between C5 and C7.
It is likely that younger people, people from various racial or ethnic backgrounds, and people with higher level injuries would differ in their experiences with outdoor recreation. The challenges and barriers to participation found in this study may be fewer than those experienced by people with higher level injuries and those from minoritized or underserved groups. Further study specific to these populations is recommended.
Conclusion
There are implications for occupational therapists and rehabilitation professionals in the areas of direct intervention, entrepreneurship, and advocacy. Sharing information early in recovery is important to raise awareness about adapted and inclusive outdoor recreation programs, equipment, as well as how to get connected with groups organizing these activities. Including outdoor recreation interests in the initial rehabilitation assessment and including clients’ outdoor recreation goals in outpatient intervention plans may facilitate outdoor recreation post-SCI.
Occupational therapists are well positioned to support entrepreneurial efforts to establish more inclusive, local outdoor recreation opportunities. This could be in a consultative role or as an entrepreneurial partnership using design and priorities informed by disabled users. Although destination-adapted recreation programs are meaningful, accessible local outdoor recreation is what allows for regular active and social participation. Contributing to the development of local spaces that are inclusive for disabled and non-disabled people to recreate together, and for specifically adapted recreation, creates environments that facilitate outdoor recreation for people with SCI.
Any substantial change in accessibility will require advocacy and policy change to regulate the costs and availability of adapted equipment and creation of inclusive outdoor environments. Advocacy takes place at the local as well as the state and national levels, and occupational therapists can get directly involved or financially support advocacy efforts.
Although these implications are mainly outside of the traditional medical model of funding for occupational therapy, they reflect the findings of the study and are consistent with AOTA Vision 2025 of collaborating for inclusion and accessibility in occupational performance (AOTA).
Footnotes
Acknowledgements
Findings from this study were previously presented at the California State University Dominguez Hills Student Research Conference on 3 March 2021.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors wish to acknowledge receipt of a Graduate Research Advancement and Development grant through California State University Dominguez Hills to fund the participant incentive gift cards.
Research Ethics and Participant Consent
California State University Dominguez Hills IRB, #21-016.