
Abstract
Background:
We estimated the prevalence of elevated liver-associated enzymes (LAEs) in a nationally representative sample of women aged 40–65 years in the United States, overall and by menopausal status or by metabolic dysfunction-associated steatotic liver disease (MASLD).
Methods:
This descriptive study used cross-sectional data from the National Health and Nutrition Examination Survey collected from 1999/2000 to 2017/March 2020. The primary study endpoint was the weighted prevalence of elevated LAEs, measured by alanine aminotransferase (ALT) or aspartate aminotransferase (AST) >3× the upper limit of normal (ULN). Prespecified secondary endpoints included the prevalence of elevated LAEs by different definitions and by menopause and MASLD status.
Results:
The study included 11,443 women aged 40–65 years (mean age 51.7 years) from surveys representing the general population: 53.3% postmenopausal, 33.8% premenopausal, and 12.9% with unknown menopausal status. The prevalence of MASLD was estimated at 29.5% (95% confidence interval [CI]: 27.7–31.4); this was higher in postmenopausal women (34.4%, 95% CI: 32.0–36.9) than premenopausal women (22.7%, 95% CI: 20.2–25.4). The estimated prevalence of ALT or AST >3× ULN was 0.87% (95% CI: 0.68–1.11); this was similar for premenopausal (0.84%, 95% CI: 0.48–1.36) and postmenopausal (0.91%, 95% CI: 0.67–1.21) women, but higher for women with MASLD (1.50%, 95% CI: 0.87–2.40) than those without MASLD (0.25%, 95% CI: 0.09–0.56).
Conclusions:
This study provides prevalence estimates of elevated LAEs in middle-aged women in the US general population. MASLD was common, and ALT or AST >3× ULN was more prevalent in women with than without MASLD.
Keywords
Introduction
An increasing body of evidence has suggested a heightened risk of liver function abnormalities in the general population. Common risk factors include metabolic dysfunction-associated steatotic liver disease (MASLD), including metabolic dysfunction-associated steatohepatitis (MASH, also called nonalcoholic steatohepatitis [NASH]), alcohol consumption, the use of various classes of medications, illegal drug use, hepatitis infection, autoimmune hepatitis, inherited or acquired muscle disease, and strenuous exercise. 1 Liver function may be affected by exposure to a hepatotoxic drug or infectious agent and may also be associated with impaired biliary, metabolic, or hemodynamic function or autoimmune disease. 2
MASLD, formerly termed nonalcoholic fatty liver disease (NAFLD), is a chronic condition characterized by the accumulation of fat in the liver in the absence of other causes of steatosis, including excess consumption of alcohol or drugs. 3
Two aminotransferase parameters, alanine aminotransferase (ALT) and aspartate aminotransferase (AST), are sensitive indicators of liver cell injury. In the research field of drug-induced liver injury (DILI), a level of ALT or AST much higher than the upper limit of normal (ULN), such as >3× ULN, is more clinically meaningful than simply being above the ULN and would usually require further evaluation by considering the combination of additional hepatic laboratory tests, such as alkaline phosphatase (ALP) and total bilirubin (TB), as well as clinical manifestations.2,4
The prevalence of elevated liver-associated enzymes (LAEs) and MASLD among middle-aged women in the general population has rarely been studied. The primary objective of this study was to estimate the prevalence of elevated LAEs, defined as ALT or AST >3× ULN, among women aged 40–65 years in the US general population, overall and by menopausal status. The secondary objectives were: (1) to estimate the prevalence of ALT or AST >3× ULN by ∼4 year survey waves and by MASLD status; (2) to estimate the prevalence of MASLD overall and by menopausal status; and (3) to estimate the prevalence of elevated hepatic laboratory test results using different thresholds above normal values: ALT >3× ULN; AST >3× ULN; ALT or AST >1× ULN, >2× ULN, or > 5× ULN; TB >2× ULN; and ALP >1.5× or >2× ULN. The findings from this study provide context for interpreting results from treatment-related studies and postmarketing safety data in similar populations.
Methods
Study design
This descriptive study used cross-sectional data from the National Health and Nutrition Examination Survey (NHANES) collected from 1999/2000 to 2017/March 2020. NHANES, conducted by the National Center for Health Statistics (NCHS) of the US Centers for Disease Control and Prevention (CDC), is a national survey that measures the health and nutrition of adults and children in the United States. 5 Each year, ∼5,000 adults and children are randomly selected to participate in NHANES (with a survey cycle every 2 years) without regard to their health/disease status. NHANES comprises interviews, questionnaires, physical examinations conducted at mobile examination centers (MECs), and laboratory results.
The original NHANES protocols were approved by the NCHS Research Ethics Review Board at the CDC, and informed consent was documented from all participants. All research using anonymized data was conducted in accordance with both the Declarations of Helsinki and Istanbul.
Data sources
This study included NHANES data from biennial surveys from 1999/2000 to 2017/March 2020 that are publicly available through the CDC. Details regarding the sampling design and measurement methods have been described elsewhere (http://www.cdc.gov/nchs/nhanes).
Because menopausal status was not directly available in the NHANES datasets, participant self-reported data were used to categorize women as postmenopausal, premenopausal, or unknown. Blood samples and physical measurements, such as waist circumference, were ascertained at the MEC. Half of NHANES participants were randomly assigned to morning MEC appointments and were asked to fast for ≥8 hours and ≤24 hours.
Participants
NHANES participants are selected using a multistage probability cluster sampling design that oversamples African Americans and Mexican American populations. Sample weights were used to account for the survey design, nonresponse, and poststratification to ensure that the estimates were representative of the noninstitutionalized US population.
This study included women aged 40–65 years at the time of each survey who were interviewed at the MEC, did not have a history of liver cirrhosis, and had at least one hepatic laboratory test result: ALT, AST, ALP, or TB. Overall prevalence estimates were based on the population of all women without cirrhosis, whereas MASLD estimates were based on the population who had fasted for ≥8 hours and ≤24 hours and did not have a known cause of liver disease (e.g., hepatitis or excess alcohol consumption).
Variables
Hepatic laboratory tests included ALT (U/L), AST (U/L), ALP (U/L), and TB (mg/dL). The cutoff points used to define elevations were based on NHANES documentation on the ULN (ALT and AST) and normal range of values (ALP and TB) for each survey cycle (Table 1).
Upper Limits of Normal for Alanine Aminotransferase and Aspartate Aminotransferase and Normal Range for Alkaline Phosphatase and Total Bilirubin by National Health and Nutrition Examination Survey Cycle in Females a
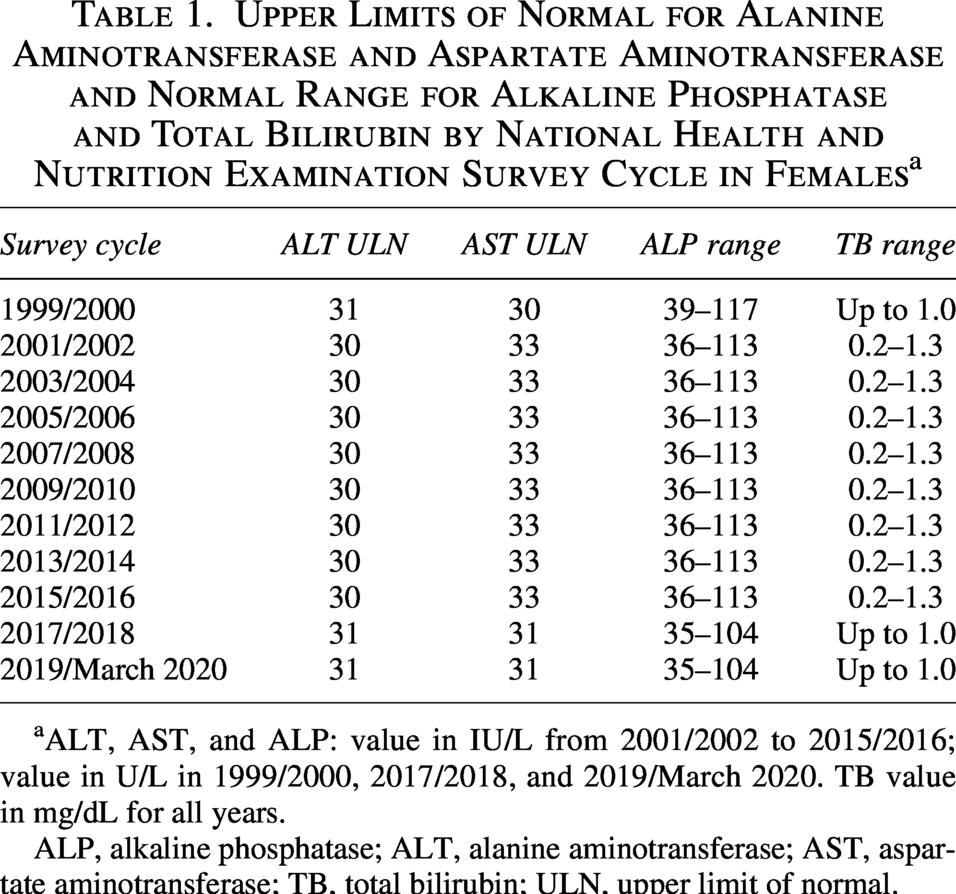
ALT, AST, and ALP: value in IU/L from 2001/2002 to 2015/2016; value in U/L in 1999/2000, 2017/2018, and 2019/March 2020. TB value in mg/dL for all years.
ALP, alkaline phosphatase; ALT, alanine aminotransferase; AST, aspartate aminotransferase; TB, total bilirubin; ULN, upper limit of normal.
MASLD was defined as a US fatty liver index (FLI) ≥30 and no evidence of other known causes of liver disease. 6 Variables used to calculate the US-FLI included age in years, race/ethnicity (categorized as non-Hispanic Black, Mexican American, other), waist circumference (cm), gamma-glutamyltransferase (GGT; IU/L), fasting insulin (pmol/L), and fasting glucose (mg/dL). Participants who were fasting for 8.0–23.9 hours (∼50% of participants randomly assigned to the morning MEC examination) and who had complete information on those variables were included in the MASLD analyses. Participants with missing data on any of those variables or who had one or more of the following known causes of liver disease were excluded from the MASLD analysis: excessive alcohol consumption (>7 alcoholic drinks/week on the self-reported Alcohol Use Questionnaire) 7 ; hepatitis B, defined as a positive result on the hepatitis B surface antigen test; hepatitis C, defined as a positive result on the hepatitis C virus RNA test; and other known causes of liver disease (available in NHANES beginning in 2017), defined as liver fibrosis, liver cirrhosis, viral hepatitis, autoimmune hepatitis, or other liver disease on the Medical Conditions Questionnaire (participant self-report in the 2017/March 2020 survey cycle).
Women were categorized as postmenopausal, premenopausal, or unknown menopausal status based on self-reported data from the Reproductive Health Questionnaire (RHQ). Women who reported having undergone a hysterectomy or bilateral oophorectomy, or who had not had a menstrual period in the past 12 months for reasons other than pregnancy or breast feeding, were categorized as postmenopausal. Women aged ≥60 years whose menopausal status could not be determined using the RHQ were also categorized as postmenopausal. Women who reported having had a menstrual period in the past 12 months, or who had not had a menstrual period in the past 12 months due to pregnancy or breast feeding, were categorized as premenopausal. Women aged between 40 and 59 years whose menopausal status could not be determined using the RHQ were categorized as having unknown menopausal status.
With the exception of menopausal status, where age was used as a proxy for postmenopausal status among the subset of women aged 60–65 years who did not have sufficient data on the RHQ to determine their menopausal status, no proxy or other methods (e.g., imputation) were applied for missing values in other variables, including those used in the US-FLI algorithm.
Endpoints
The primary study endpoint was the presence of ALT or AST >3× ULN. This endpoint was chosen to provide relevant background information to support hepatic safety assessment in pharmaceutical development, where ALT or AST >3× ULN is a key component in defining DILI.2,4 Prespecified secondary endpoints were the presence of MASLD or elevated hepatic laboratory test results using different thresholds above the normal values: ALT >3× ULN; AST >3× ULN; ALT or AST >1× ULN, >2× ULN, or >5× ULN; TB >2× ULN; ALP >1.5× or >2× ULN.
Statistical analysis
The main summary measures were the weighted prevalence as a point estimate and its 95% confidence interval (CI). Analytic procedures that account for the complex survey design and sample weights were used to generate estimates that are representative of the noninstitutionalized US population of women aged 40–65 years. 8 Variance was estimated using the Taylor Series Linearization method, and the 95% CI for proportions was calculated using the Korn and Graubard method. 9 For MASLD estimates, we used NHANES fasting subsample weights (e.g., WTSAF2YR), rescaled per NCHS guidance to combine the 1999–2018 cycles and the 2017–March 2020 release.
Results
Survey population
For all survey cycles combined, 12,687 women aged 40–65 years participated in NHANES. Of those women, 11,443 (90.2%) were examined at a MEC and had ≥1 valid hepatic laboratory test and therefore were eligible for this study. The reasons for the 1244 exclusions were as follows: no MEC interview (n = 479), history of liver cirrhosis (n = 6), or no valid hepatic laboratory test (n = 759). Weighted demographic and clinical characteristics of the study population of US women aged 40–65 years are summarized in Table 2. The weighted mean age was 51.7 years, 69.4% were non-Hispanic White, 12.1% were Hispanic, and 40.0% were obese. In total, 53.3% were categorized as postmenopausal, 33.8% as premenopausal, and 12.9% had unknown menopausal status.
Weighted Characteristics of Women in the United States Aged 40–65 Years in National Health and Nutrition Examination Survey
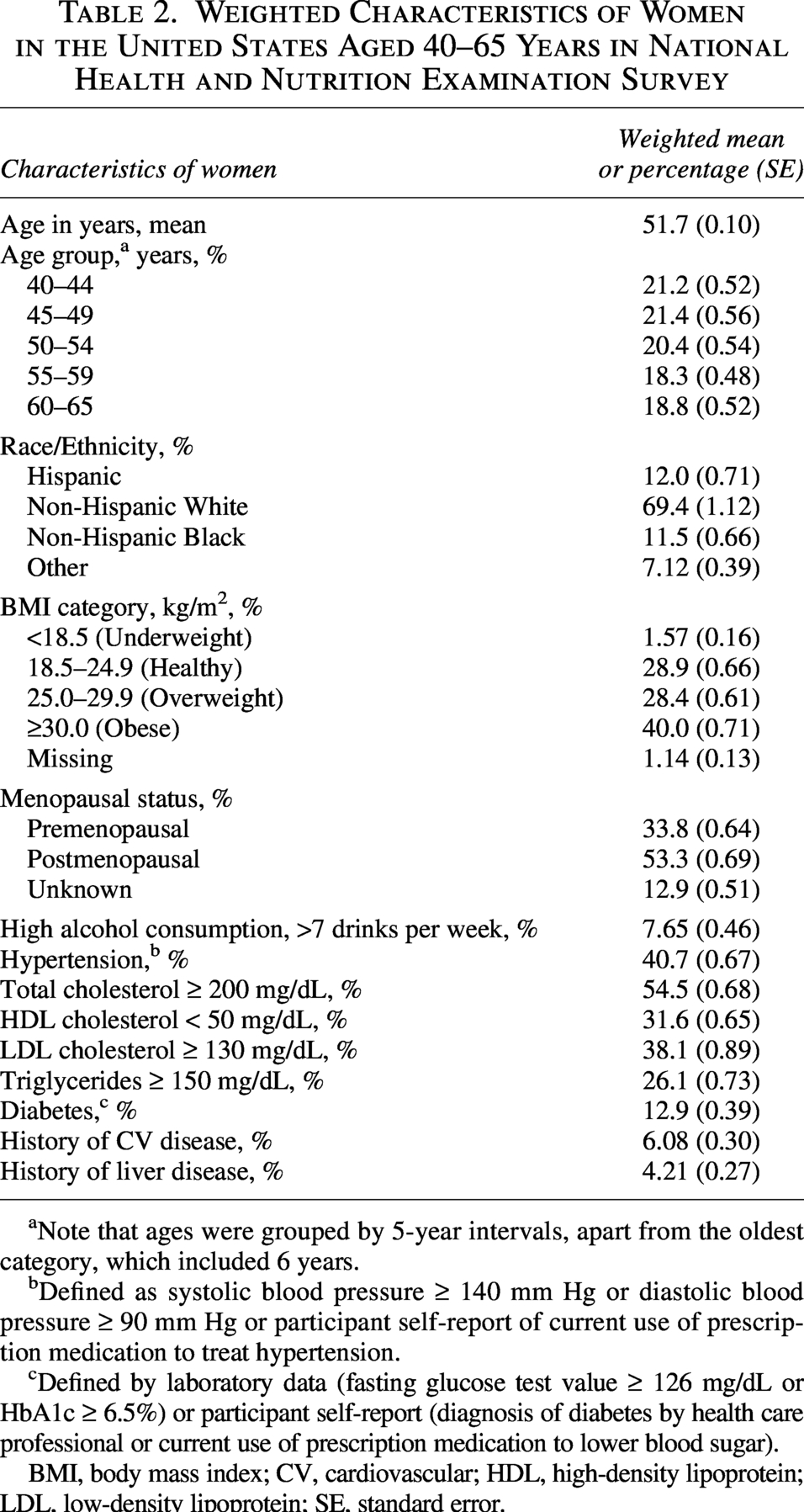
Note that ages were grouped by 5-year intervals, apart from the oldest category, which included 6 years.
Defined as systolic blood pressure ≥ 140 mm Hg or diastolic blood pressure ≥ 90 mm Hg or participant self-report of current use of prescription medication to treat hypertension.
Defined by laboratory data (fasting glucose test value ≥ 126 mg/dL or HbA1c ≥ 6.5%) or participant self-report (diagnosis of diabetes by health care professional or current use of prescription medication to lower blood sugar).
BMI, body mass index; CV, cardiovascular; HDL, high-density lipoprotein; LDL, low-density lipoprotein; SE, standard error.
Prevalence of MASLD
There were 4,675 women aged 40–65 years without a known cause of liver disease with sufficient data to calculate the US-FLI (fasting glucose and insulin test results, as well as waist circumference, GGT, age, and race/ethnicity data) and thus determine their MASLD status. The prevalence of MASLD was estimated to be 29.5% (95% CI: 27.7–31.4) (Table 3). The MASLD prevalence estimate was higher in postmenopausal women than in premenopausal women (34.4% [95% CI: 32.0–36.9] and 22.7% [95% CI: 20.2–25.4], respectively). In a post hoc analysis, the weighted prevalence of MASLD was 25.3%, 22.9%, 29.6%, 33.6%, and 33.6% across the survey periods 1999–2002, 2003–2006, 2007–2010, 2011–2014, and 2015–March 2020, respectively.
Prevalence of Metabolic Dysfuction-Associated Steatotic Liver Disease Overall And by Menopausal Status Among Women in the United States Aged 40–65 Years in National Health and Nutrition Examination Survey
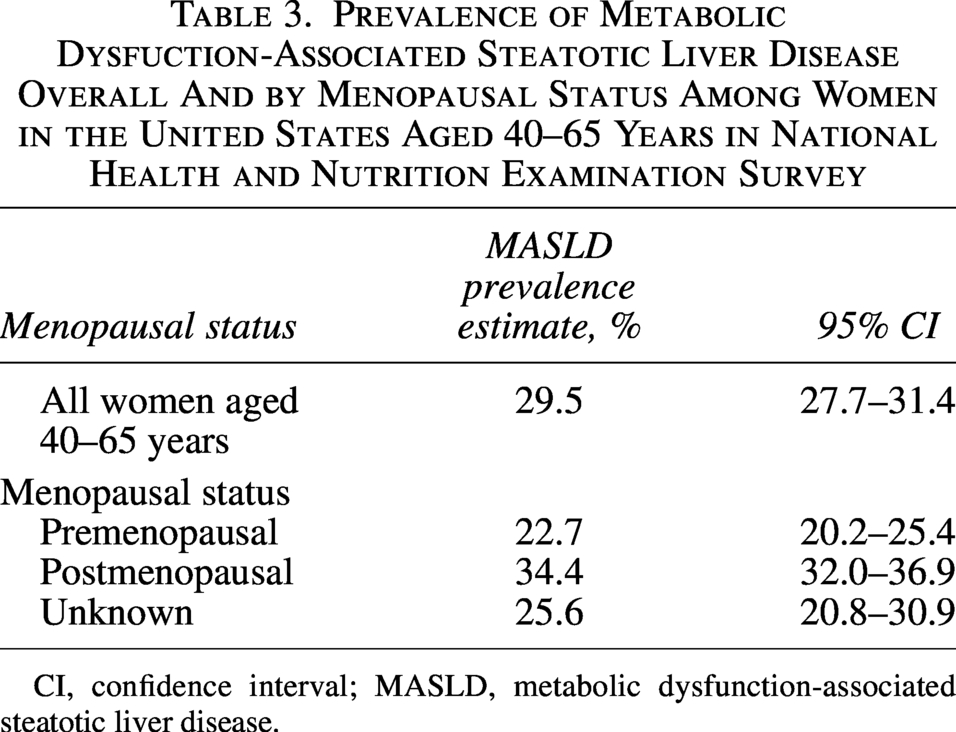
CI, confidence interval; MASLD, metabolic dysfunction-associated steatotic liver disease.
Prevalence of ALT or AST >3× ULN overall and by subgroups
Of 11,443 eligible women, 11,424 had both ALT and AST results available for the primary endpoint. The weighted prevalence of ALT or AST >3× ULN was 0.87% (95% CI: 0.68–1.11) (Fig. 1). The estimated prevalence was similar by menopausal status (0.91% in postmenopausal women; 0.84% in premenopausal women). The prevalence of ALT or AST >3× ULN was also similar across the ∼4-year survey cycle periods chosen a priori for this study (Table 4). The estimated prevalence of ALT or AST >3× ULN was 1.50% (95% CI: 0.87–2.40) in women with MASLD and was 0.25% (95% CI: 0.09–0.56) in women without MASLD (Fig. 1).
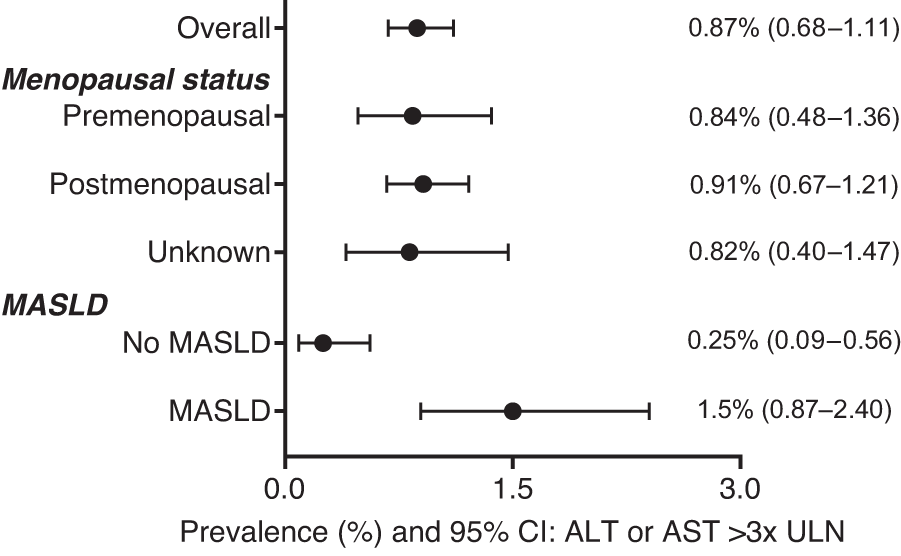
Prevalence (%) of ALT or AST >3× ULN among women aged 40–65 years overall, by menopausal status and by MASLD. Prevalence estimate and 95% CI are weighted and account for the complex survey design used by NHANES. ALT, alanine aminotransferase; AST, aspartate aminotransferase; CI, confidence interval; MASLD, metabolic dysfunction-associated steatotic liver disease; ULN, upper limit of normal.
Prevalence of Elevated Liver-Associated Enzymes Defined as Alanine Aminotransferase or Aspartate Aminotransferase >3× Upper Limit of Normal per 4-Year National Health and Nutrition Examination Survey Cycle Period
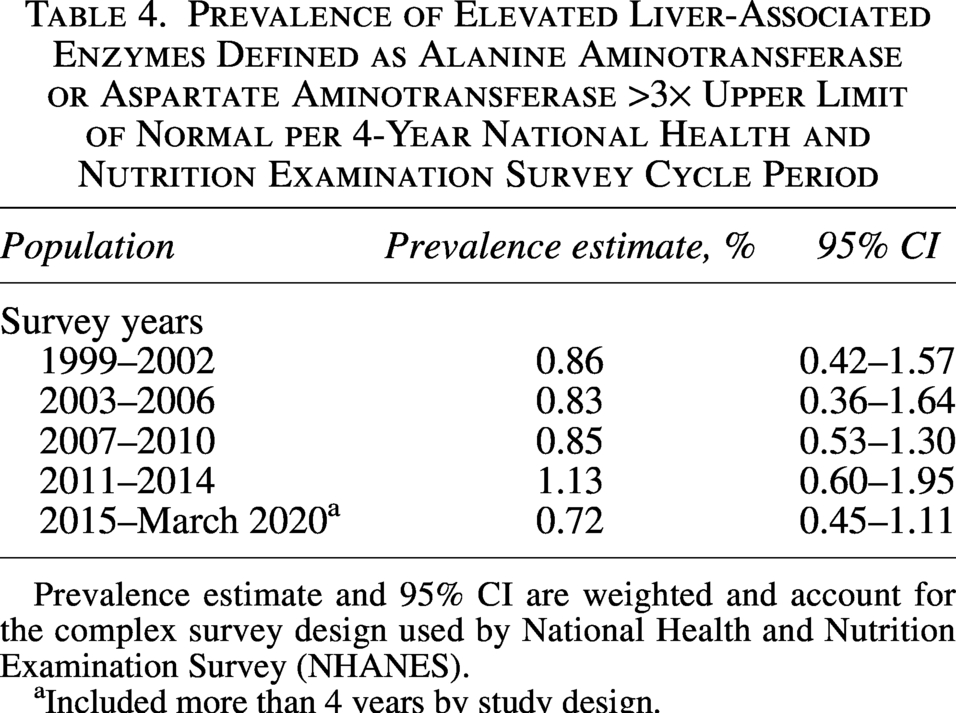
Prevalence estimate and 95% CI are weighted and account for the complex survey design used by National Health and Nutrition Examination Survey (NHANES).
Included more than 4 years by study design.
Prevalence of other hepatic laboratory test abnormalities
The estimated prevalence (95% CI) of hepatic laboratory measures with a test result abnormality are presented in Table 5. The estimated prevalence (95% CI) of elevated ALT or AST was: 15.11% (14.26–15.98) for >1× ULN, 2.29% (1.97–2.65) for >2× ULN, and 0.18% (0.10–0.31) for >5× ULN. The estimated prevalence of ALT >3× ULN was 0.64% (0.48–0.84), and for AST >3× ULN was 0.53% (0.37–0.74). For TB, prevalence >2× ULN was 0.02% (0.002–0.09). For ALP, prevalence >1.5× ULN was 0.46% (0.34–0.60) and >2× ULN was 0.15% (0.09–0.24).
Prevalence of Elevated Hepatic Laboratory Test Results in Women Aged 40–65 Years in National Health and Nutrition Examination Survey
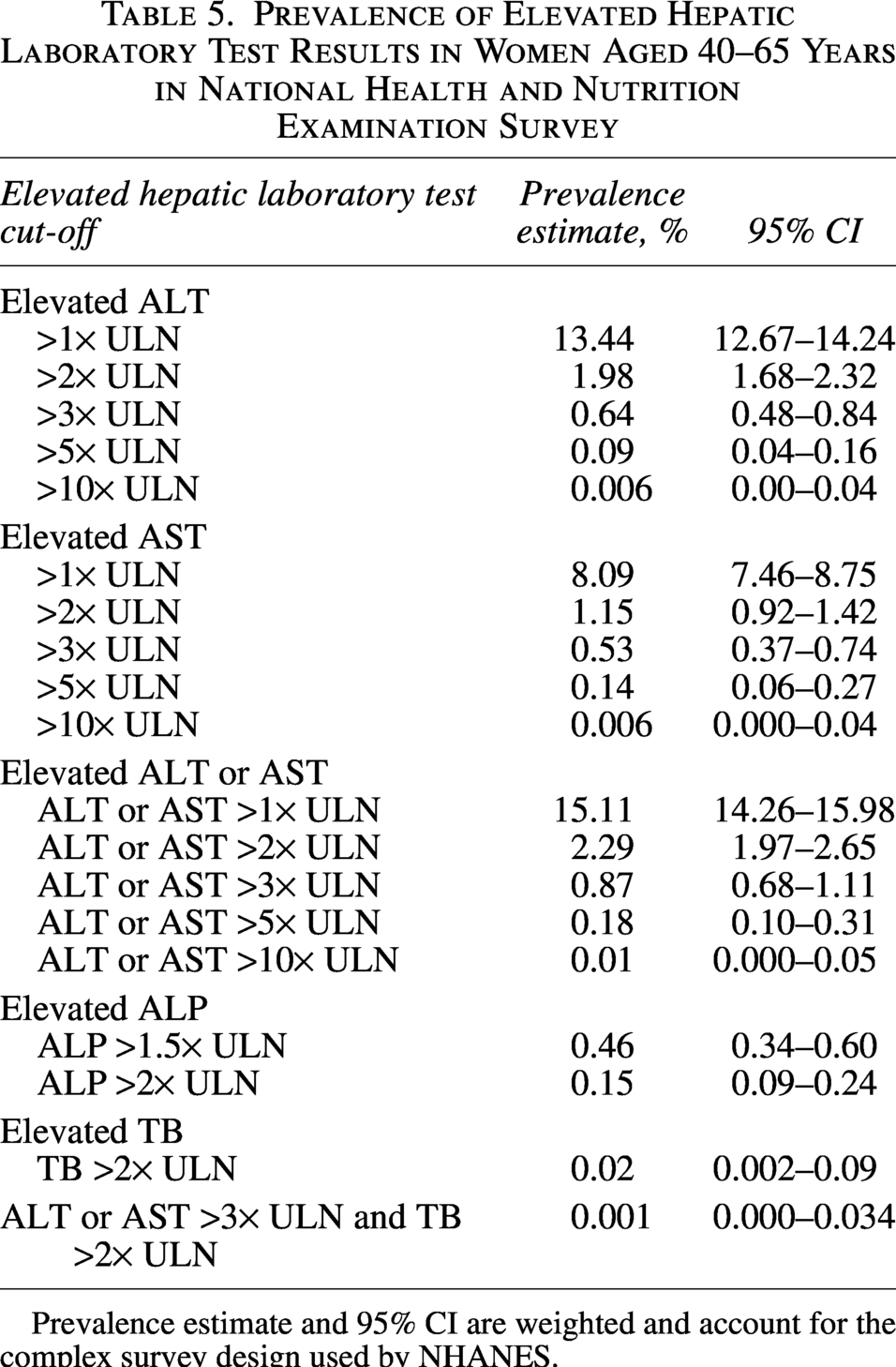
Prevalence estimate and 95% CI are weighted and account for the complex survey design used by NHANES.
Discussion
Several US studies using data from NHANES have previously reported the prevalence of elevated LAE in the adult population.10–13 Overall, the prevalence of ALT or AST above the normal range (i.e., >1× ULN) was 4–16%, depending on the definitions used and the study period evaluated in NHANES.10–13 While a direct comparison with previous studies is not possible, as studies had differing age ranges and other characteristics, findings from the current study (15% of participants with ALT or AST >1× ULN) were generally consistent with estimates from these previous studies based on NHANES data. The prevalence of elevated LAEs was reported in two additional studies in the United States, one in a routine medical care setting (elevated ALT or AST >1× ULN reported in 13% of participants) and another in an executive health program (elevated ALT or AST observed in 15% of participants).14,15
The parameter of ALT or AST >3× ULN is used for hepatotoxicity assessment in pharmaceutical development. As clinical characteristics of DILI are similar to liver injuries associated with other causes, the diagnosis of DILI is generally made by exclusion of other causes. Few studies have assessed the prevalence of liver enzyme abnormality defined as ALT or AST >3× ULN in the general population, and no recent population-based observational studies have specifically reported these parameters in women. The prevalence of ALT or AST >3× ULN of ∼0.9% in women aged 40–65 years in this study was consistent with estimates from a meta-analysis of clinical studies of statins. 16 In the statin meta-analysis, which included 73 trials investigating six different statins, the incidence of elevated aminotransferase in placebo arms ranged from 0.6% to 0.9%. 16 While the definition of elevated aminotransferase varied by individual statin trial, ALT or AST >3× ULN was a key component in the definition for most trials. 16 The prevalence is also consistent with results from participants in placebo arms of fezolinetant clinical trials, in which ∼1% had ALT or AST >3× ULN during follow-up.17–19
In this study, ∼30% of women aged 40–65 years had MASLD. This estimate is consistent with several other studies from NHANES using US-FLI to define MASLD,6,7,20–22 with MASLD prevalence rising over time. For example, US estimates in the general population show an increase from ∼19% in 1988–1994 to over 30% by 2012.23–25 In the NHANES survey data from the period 2007–2014, ∼32% of women aged ≥45 years in the United States had MASLD. 20 Our study provided further evidence that MASLD is as common in the United States as it is elsewhere. 26
In 2017, NHANES began to use vibration-controlled transient elastography, a noninvasive medical imaging technique, for the detection of liver steatosis and liver fibrosis. However, different cutoff points of controlled attenuation parameters for liver steatosis or MASLD have been applied, and the corresponding prevalence estimates have not been consistent across studies.27–32 Overall, the prevalence estimates from these studies appear to be higher than estimates from the current study and other studies using US-FLI to define MASLD. Further studies are needed to compare results based on different methodologies and to establish the optimal and most practical way to accurately estimate the prevalence of MASLD.
In the current analysis, which aimed to estimate the prevalence of liver function abnormality by MASLD status, the prevalence of ALT or AST >3× ULN was found to be higher (1.50%, 95% CI: 0.87–2.40) in women with MASLD than in women without MASLD (0.25%, 95% CI: 0.09–0.56). Thus, assessment of MASLD is important when investigating reasons for transaminase elevations in hepatotoxicity assessment in clinical trials of drugs and in the postmarketing setting.
In this study, weighted prevalence estimates using the nationwide survey data were calculated using analytic methods that accounted for the complex survey design, nonresponse bias, and oversampling. Thus, the reported findings can be considered generalizable to women aged 40–65 years in the noninstitutionalized US population.
Limitations
This study has several limitations. First, the definition of MASLD was based on the US-FLI, which is calculated using an equation rather than ultrasound or other technologies. 6 Therefore, there may be misclassification bias. Second, the prevalence of MASH, an important risk factor for liver enzyme elevations, cannot be estimated reliably since data on MASH are not directly available from NHANES surveys. In addition, there is no direct indicator of menopausal status in the original survey data. In the current analysis, menopausal status was categorized based on responses to interview questions, which may result in misclassification bias.
Conclusion
In conclusion, this study provided weighted prevalence estimates of elevated LAEs and MASLD among women aged 40–65 years that are generalizable to the United States noninstitutionalized population. The study findings were broadly consistent with those of previous studies in the United States based on different study populations. The prevalence of ALT or AST >3× ULN was similar among pre- and postmenopausal women. MASLD was common among middle-aged women in the general population, and the prevalence of ALT or AST >3× ULN was higher in women with MASLD than in those without MASLD.
Authors’ Contributions
Y.A.C., A.S.-I., B.P.-L., K.M., and N.J.R.: Substantial contribution to study design. Y.A.C., A.S.-I., R.S., W.H., and N.J.R.: Acquisition of study data. Y.A.C., A.S.-I., B.P.-L., R.S., W.H., and N.J.R.: Analysis of study data. Y.A.C., A.S.-I., B.P.-L., K.M., R.S., W.H., U.C.-K.-S., and N.J.R.: Interpretation of study data. All authors read and approved the final article.
Data Availability
Researchers may request access to the data used to support this article by contacting the corresponding author.
Footnotes
Acknowledgments
Assistance with the study: Medical writing support was provided by Samantha Coates and Sue Cooper from Envision Pharma, Inc. and was funded by the study sponsor. The authors also acknowledge Francesca Goudie and Thomas Devilee from Leiden University, as well as Maartje Smulders, Josephine Wolfram, and Frank Cao from Astellas.
Author Disclosure Statement
Yadong Adam Cui, Bosny Pierre-Louis, and Wei Han are employees of Astellas Pharma Global Development. Amy Storfer-Isser was formerly an employee of Astellas Pharma Global Development. Karla Martins is an employee of Astellas Pharma Europe Ltd. Robert Snijder and Ulrich Chin-Kon-Sung are employees of Astellas Pharma Europe B.V., The Netherlands. Noah Jamie Robinson is an employee of Astellas Pharma A.G., Switzerland.
Funding Information
This study was funded by the Astellas Pharma Inc.