
Abstract
Background:
Choosing antibiotics for prenatal urinary tract infections (UTIs) is challenging because fetal safety data are inconclusive and must be weighed against resistance. Recent information on prescribing patterns and antimicrobial susceptibility is sparse; we aimed to address this gap.
Study Design:
We used electronic health record data from two US health systems (Kaiser Permanente Washington [KPWA] and Vanderbilt University Medical Center [VUMC]) to ascertain pregnancies from January 1, 2006, to August 31, 2023, to individuals aged 15–49. We included outpatient-treated prenatal UTIs with an oral UTI antibiotic plus a diagnosis or positive urine culture. We described patterns of antibiotic utilization and susceptibility overall (2006–2023) and by year (2010–2022).
Results:
We identified 10,734 eligible UTIs. The most common antibiotics were nitrofurantoin (KPWA: 42%; VUMC: 65%) and first generation cephalosporins (KPWA: 23%; VUMC: 15%). Nitrofurantoin decreased substantially from 2010 to 2022 (KPWA: from 50% to 27%; VUMC: 65–49%), while first generation cephalosporins increased (KPWA: 12 to 45%; VUMC: 14 to 21%). Escherichia coli was susceptible to nitrofurantoin in 98–99% of UTIs. Susceptibility to other antibiotics was higher at KPWA than VUMC (first generation cephalosporins: KPWA: 97%, VUMC: 89%; amoxicillin–clavulanate: KPWA: 93%, VUMC: 85%). 93–95% were treated with an appropriate antibiotic based on susceptibility results.
Conclusions:
In two health systems in different regions, nitrofurantoin decreased substantially while first generation cephalosporins increased, despite better nitrofurantoin susceptibility. Other concerns, like malformation risk, may have influenced prescribing. Further research and guideline development are needed to weigh risks versus benefits of different antibiotics for prenatal UTIs.
Keywords
Background
Guidelines in the United States recommend universal prenatal screening for urinary tract infections (UTIs) and antibiotic treatment 1 to lower risk of serious maternal and neonatal harms, including pyelonephritis, sepsis, preterm labor, and low birth weight.2,3 In pregnancy, it is recommended to treat asymptomatic bacteriuria identified through screening, as well as acute cystitis. Due to emphasis on early detection and treatment, UTIs are among the leading indications for antibiotic use during pregnancy. 4 However, guidance about which antibiotics to use has been complicated in recent decades by questions about effectiveness and safety. Since 2011, the American College of Obstetricians and Gynecologists (ACOG) has cautioned against using nitrofurantoin in the first trimester, if an acceptable alternative antibiotic is available, due to inconclusive evidence of increased risk of birth defects.1,5 In addition, temporal changes in bacterial susceptibility to antibiotic agents add complexity to these concerns, with the threat of increasing resistance to some commonly used medications. 6
Quantifying antibiotic utilization for UTIs in pregnancy is the necessary first step to investigating the impact on the health of pregnant individuals. Using electronic health record (EHR) data from two health systems in different US regions, we characterized utilization of antibiotic agents for the outpatient treatment of UTI during pregnancy for the whole study period (2005–2023) and individually for years with at least 50 UTIs per health system (2010–2022). Additionally, we quantified bacterial organisms identified from urine samples and assessed antimicrobial sensitivity, for the whole study period and stratified by year.
Methods
Settings
The study was set within Kaiser Permanente Washington (KPWA) and Vanderbilt University Medical Center (VUMC), two health systems based in different regions of the United States. KPWA is an integrated health care delivery system that provides insurance and health care in Washington State, with over 7,000 pregnancies to KPWA members annually. For prenatal care, approximately half of individuals insured by KPWA see internal KPWA providers, and half see external providers. VUMC provides health care for middle Tennessee, with over 4,000 births annually in the greater Nashville area. At VUMC, all obstetric care is delivered by VUMC clinicians. The study was approved by the KPWA and the VUMC Institutional Review Boards (with waivers of consent).
Data sources
KPWA and VUMC have rich EHR data including demographics, health care encounters, diagnoses and procedures, laboratory data, and medication/pharmacy data. KPWA also has enrollment data with the date of enrollment and disenrollment. At KPWA, prescription medication information was identified via medication dispensings and orders and at VUMC via medication orders. KPWA databases capture laboratory data only for patients who receive care internally. At VUMC, all laboratory testing is conducted internally and available in VUMC databases.
Study sample
Our final sample included treated UTIs in pregnant individuals aged 15–49 who were enrolled in the health system (KPWA) or had a visit (VUMC) by 20 weeks’ gestation with a pregnancy outcome date from January 1, 2006, to August 31, 2023 (some prenatal UTIs occurred in 2005). Details of inclusion and exclusion criteria are presented in Supplementary Figures S1A and S1B. At VUMC, we included livebirths only due to data availability; at KPWA, the cohort additionally included stillbirths, spontaneous abortions, and terminations. A “treated UTI” was defined as a combination of medication use with either a UTI diagnosis or laboratory test. Specifically, we required an outpatient medication order or dispensing for an oral antibiotic commonly used to treat UTIs (Supplementary Table S1) between pregnancy onset and the day before pregnancy outcome, along with either: (1) a documented UTI diagnosis in the 0–5 days prior to the order or dispensing date, or (2) a positive urine culture 0–8 days prior to the order or dispensing date. We defined “index” date as the date of an antibiotic dispensing or order. At KPWA, if there was both an order and a dispensing in the appropriate window, we used the earlier date. We allowed diagnoses of acute cystitis or asymptomatic bacteriuria to qualify (Supplementary Table S2). We defined a positive urine culture as ≥10,000 colony-forming units (CFU)/mL of selected bacterial organisms (those commonly accepted as causing UTI), instead of the clinical guideline-recommended definition of ≥100,000. 1 The choice of cutpoint was informed by input from co-investigators with expertise in infectious disease and maternal–fetal medicine who noted that providers may be more inclined to treat potential UTIs in pregnancy at a lower threshold, given concerns about risk of adverse pregnancy outcomes with untreated infections. We excluded UTIs with different antibiotic agents prescribed or dispensed on the same day and UTIs in individuals with systemic autoimmune conditions, cancer, HIV/AIDS, spinal cord injuries; recent hospitalization, pyelonephritis, or kidney stones; or a previous UTI diagnosis or positive urine culture (in the 90–9 days before index date). We excluded UTIs in these individuals because they have higher risk of complications or antibiotic resistance, and therefore treatment guidelines differ from the treatment of uncomplicated cystitis. We restricted to the first UTI meeting inclusion criteria per pregnancy. Individuals could contribute more than one pregnancy to the cohort and thus more than one UTI. For analyses related to microbial susceptibility, the sample was further restricted to those with positive urine culture results and available susceptibility results.
At both sites, we extracted information about characteristics of the study population, including age, sex, race, and ethnicity (details in Table 1 footnotes), body mass index (BMI), pregestational diabetes, and Medicaid coverage. At KPWA, we additionally ascertained pregnancy outcome (e.g., livebirth, stillbirth), prescriber type and specialty, and care setting.
Characteristics of Pregnant Individuals with Treated Urinary Tract Infections, 2005–2023
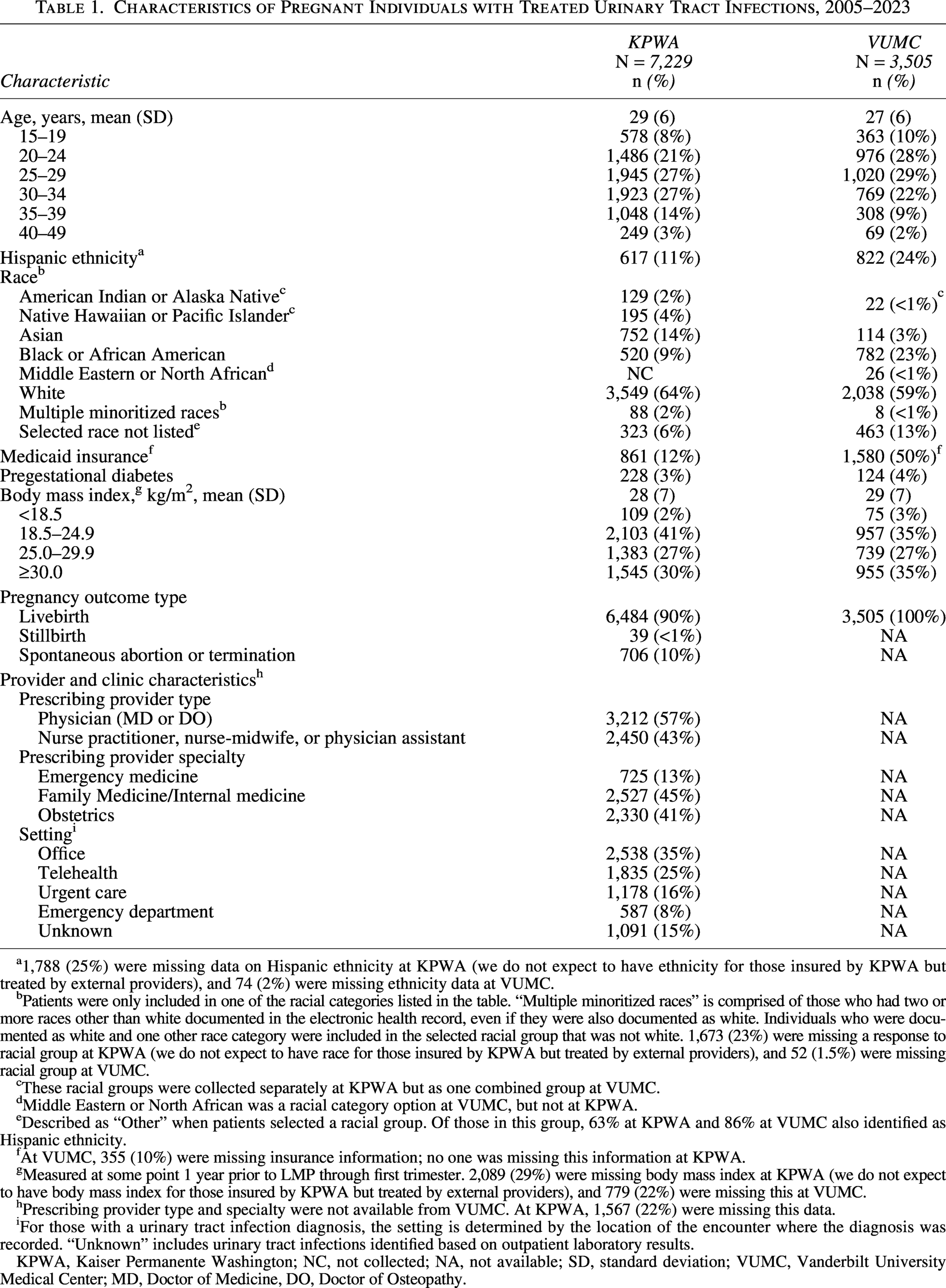
1,788 (25%) were missing data on Hispanic ethnicity at KPWA (we do not expect to have ethnicity for those insured by KPWA but treated by external providers), and 74 (2%) were missing ethnicity data at VUMC.
Patients were only included in one of the racial categories listed in the table. “Multiple minoritized races” is comprised of those who had two or more races other than white documented in the electronic health record, even if they were also documented as white. Individuals who were documented as white and one other race category were included in the selected racial group that was not white. 1,673 (23%) were missing a response to racial group at KPWA (we do not expect to have race for those insured by KPWA but treated by external providers), and 52 (1.5%) were missing racial group at VUMC.
These racial groups were collected separately at KPWA but as one combined group at VUMC.
Middle Eastern or North African was a racial category option at VUMC, but not at KPWA.
Described as “Other” when patients selected a racial group. Of those in this group, 63% at KPWA and 86% at VUMC also identified as Hispanic ethnicity.
At VUMC, 355 (10%) were missing insurance information; no one was missing this information at KPWA.
Measured at some point 1 year prior to LMP through first trimester. 2,089 (29%) were missing body mass index at KPWA (we do not expect to have body mass index for those insured by KPWA but treated by external providers), and 779 (22%) were missing this at VUMC.
Prescribing provider type and specialty were not available from VUMC. At KPWA, 1,567 (22%) were missing this data.
For those with a urinary tract infection diagnosis, the setting is determined by the location of the encounter where the diagnosis was recorded. “Unknown” includes urinary tract infections identified based on outpatient laboratory results.
KPWA, Kaiser Permanente Washington; NC, not collected; NA, not available; SD, standard deviation; VUMC, Vanderbilt University Medical Center; MD, Doctor of Medicine, DO, Doctor of Osteopathy.
Antibiotic agents
We assessed treatment with oral antibiotic agents often used for UTIs, including trimethoprim–sulfamethoxazole (TMP–SMX), nitrofurantoin, β-lactams (first generation cephalosporins, second generation cephalosporins, third generation cephalosporins, amoxicillin or ampicillin, and amoxicillin–clavulanate), and fluoroquinolones (specific agents in Supplementary Table S1).
Antimicrobial susceptibility
We reported the proportion of UTI samples susceptible to different antibiotics for several common bacteria. For analyses by year, we restricted to the most common bacterium, E. coli.
We defined a “good match” as a UTI caused by a bacterium that was susceptible to the index antibiotic agent.
Statistical analysis
First, we conducted descriptive analyses of population characteristics. For the antibiotic utilization and “good match” measures, we reported counts and proportions, along with 95% Wilson confidence intervals (CIs), which perform well with small sample size or low proportions.7,8 Analyses were run separately by health system. Analyses were conducted for the whole time period and across individual calendar years with at least 50 UTIs at each site (2010–2022). We also assessed utilization separately by first trimester versus second or third trimester. For the susceptibility measures, we created antibiograms showing the proportion of susceptible samples, considering susceptibility high if ≥ 90%, moderate if 60–89%, and low if <60%. 9 Accepted thresholds between moderate and high susceptibility are 80–90%, with some guidelines recommending different thresholds for different medications9,10; we used 90% for all medications to be conservative, given the setting of pregnancy. Analyses were conducted in SAS 9.4 (Cary, NC, USA), R 4.4.0 (Vienna, Austria), and Tableau 23.1 (Seattle, WA, USA).
Results
Study flow
After applying inclusion and exclusion criteria, we identified 10,734 eligible UTIs, with 7,229 UTIs at KPWA (among 6,804 individuals) and 3,505 UTIs at VUMC (among 3,339 individuals) (Supplementary Figs. S1A and S1B). Among these UTIs, 4,093 (KPWA: 2,133; VUMC: 1,960) had positive urine culture results and susceptibility results and were included in the bacterial susceptibility analyses.
Sample characteristics
Mean age at prenatal UTI was 29 years at KPWA and 27 years at VUMC (Table 1). All individuals in the sample had sex recorded as female. Of UTIs in pregnant individuals with documented ethnicity, 11% at KPWA and 24% at VUMC were in Hispanic individuals; of those with documented race, the largest groups at KPWA were white (64%) and Asian (14%), and at VUMC, white (59%) and Black or African American (23%). A larger proportion of UTIs were in individuals insured by Medicaid at VUMC (50%) than at KPWA (12%). For pregnancies with BMI data, 30% of eligible UTIs at KPWA and 35% at VUMC were in individuals with a BMI ≥30 kg/m2. At KPWA, 90% were livebirths, 10% were spontaneous abortions or terminations, and <1% were stillbirths; VUMC data included livebirths only. The median gestational age of the first visit in pregnancy was 6 weeks for KPWA and 8 weeks for VUMC. UTIs occurred predominantly in the first trimester (KPWA: 59%, median gestational age: 11 weeks; VUMC: 50%, median gestational age: 14 weeks). At KPWA, slightly more providers who prescribed the antibiotic were in family medicine, internal medicine, or pediatrics (45%) than in obstetrics (41%); VUMC data did not include provider specialty.
Antibiotic utilization
The most commonly used antibiotics for UTI over the whole study period (2005–2023) were nitrofurantoin (KPWA: 42%, VUMC: 65%) and first generation cephalosporins (KPWA: 23%, VUMC: 15%; Supplementary Table S3A). From 2010 to 2022, the proportion of UTIs treated with nitrofurantoin decreased considerably at both sites, dropping from 50% to 27% at KPWA and from 65% to 49% at VUMC. First-generation cephalosporin use increased greatly at both sites, with a more pronounced increase at KPWA (from 12% to 45%) than at VUMC (from 14% to 21%) (Fig. 1; Supplementary Table S3A). At KPWA, use of first generation cephalosporins surpassed nitrofurantoin in 2018 and was greater for the rest of the study years, while nitrofurantoin was the most used antibiotic at VUMC in all study years. There was a slight increase in amoxicillin–clavulanate at both sites (KPWA: from 2% to 7%; VUMC: from 6% to 14%). Use of amoxicillin or ampicillin decreased at KPWA (from 26% to 8%), while use did not appear to change meaningfully at VUMC. Similar patterns of decreasing nitrofurantoin use and increasing cephalosporin use were observed across provider type and specialty (Supplementary Fig. S2 and S3).
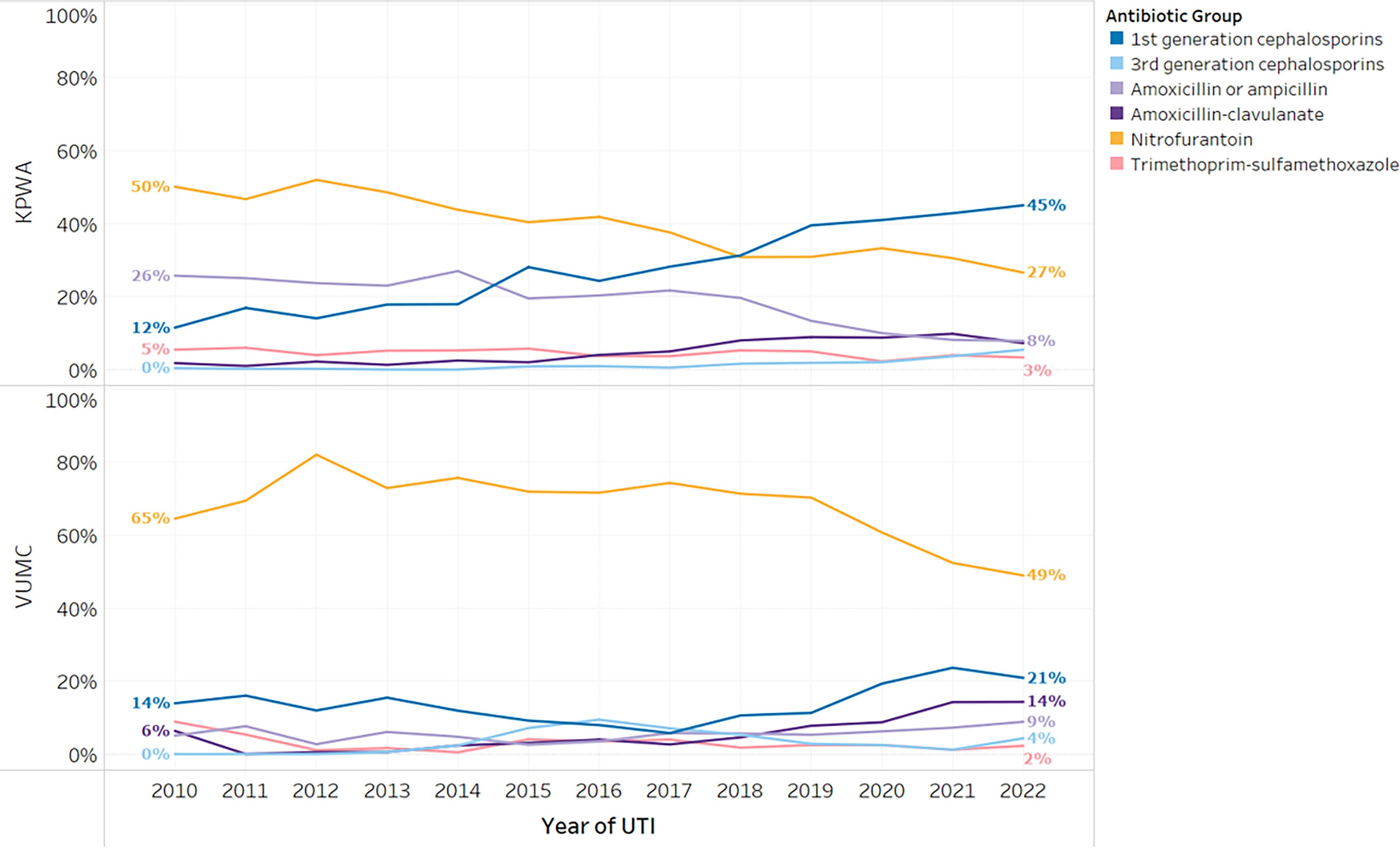
Antibiotic agent utilization for urinary tract infections in pregnancy, 2010–2022. Analyses across individual calendar years were only conducted for years with at least 50 UTIs at each site (2010–2022). Some antibiotic groups were not included here due to small proportions (second generation cephalosporins and fluoroquinolones), but are presented in Supplementary Table S3A. KPWA, Kaiser Permanente Washington; VUMC, Vanderbilt University Medical Center.
The proportion of nitrofurantoin use was slightly lower in the first trimester versus the second and third trimesters, but decreased over time in all trimesters, while cephalosporin use increased (Fig. 2, Supplementary Table S3B).
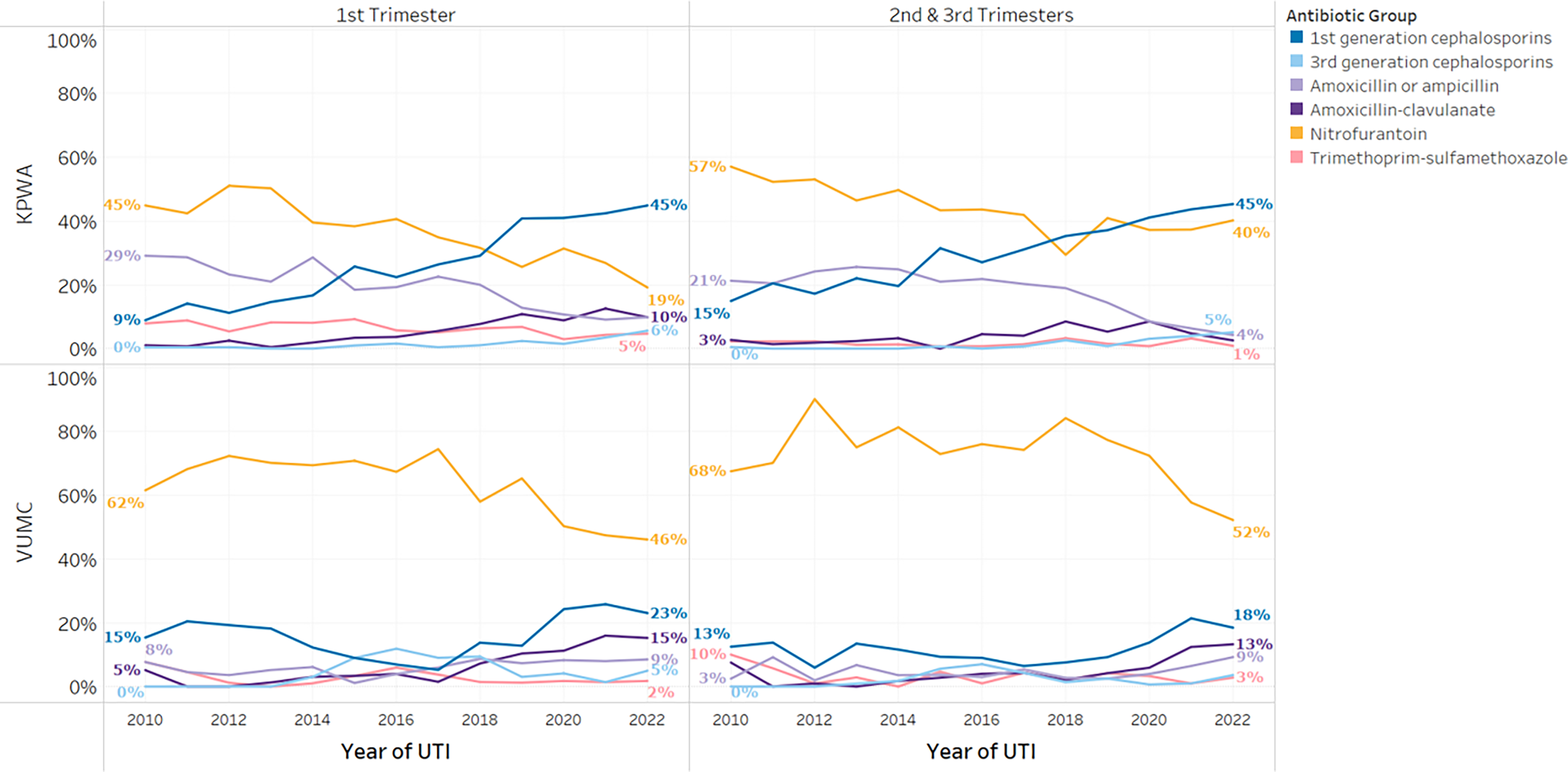
Antibiotic agent utilization for UTIs in pregnancy in KPWA and VUMC by trimesters, 2010–2022. Some antibiotic groups were not included here due to small proportions (second generation cephalosporins and fluoroquinolones), but they are presented in Supplementary Table S3B. KPWA, Kaiser Permanente Washington; VUMC, Vanderbilt University Medical Center.
Most common microorganisms and prevalence of antibiotic resistance
E. coli was the predominant microorganism detected by urine culture (KPWA: 76%, VUMC: 73%), followed by Enterococcus (KPWA: 7%, VUMC: 9%), Klebsiella (KPWA: 6%, VUMC: 9%), S. Saprophyticus (KPWA: 5%, VUMC: 3%), and Proteus (KPWA: 3%, VUMC: 4%) (Supplementary Table S4). Among (treated) UTIs with a culture in our data that detected a typical UTI-causing organism, the majority had a bacterial count of ≥ 100,000 CFU/mL, and a minority had less than 100,000 CFU/mL (below the clinical guideline-recommended threshold for treatment 1 ). Specifically, at KPWA, 69% had a culture growing ≥ 100,000 CFU/mL, 26% had 10,000 to < 100,000 CFU/mL, and 5% had 1,000 to < 10,000 CFU/mL; at VUMC, 62% had ≥ 100,000 CFU/mL, 38% had 10,000 to < 100,000 CFU/mL, and 1% had 1,000 to < 10,000 CFU/mL. The proportion of UTIs treated at 10,000 to < 100,000 CFU/mL varied by antibiotic and organism (Supplementary Table S5 and S6).
Most bacteria had moderate-to-high susceptibility to all antibiotics (Supplementary Table S7). At KPWA, E. coli was highly susceptible to most antibiotics, including nitrofurantoin (98%), first-generation cephalosporins (97%), and amoxicillin–clavulanate (93%), but only moderately susceptible to TMP–SMX (86%) and amoxicillin or ampicillin (69%). At VUMC, E. coli was highly susceptible to nitrofurantoin (99%), but only moderately susceptible to first generation cephalosporins (89%), amoxicillin–clavulanate (85%), and TMP–SMX (78%), and had low susceptibility to amoxicillin or ampicillin (56%).
Over time, E. coli susceptibility patterns remained relatively stable at both institutions with one exception: at VUMC, susceptibility to first generation cephalosporins decreased from 98% in 2010 to 78% in 2022 (Figs. 3 and 4).
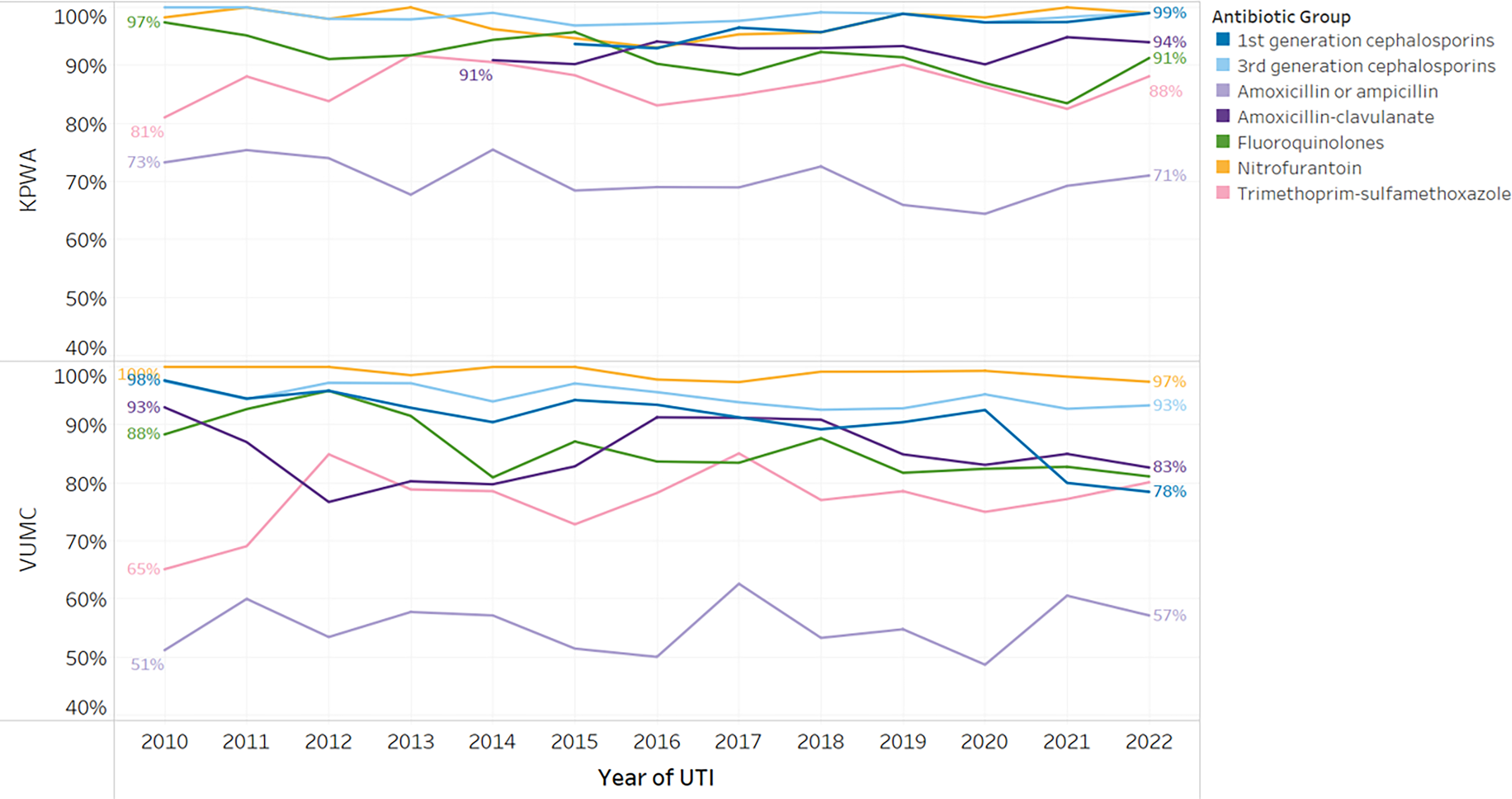
Antibiotic susceptibilities to urinary tract infections in pregnancy by year, 2010–2022, among infections with E. coli. Second generation cephalosporins) were not included here due to small numbers, but are presented in Figure 4. KPWA, Kaiser Permanente Washington; VUMC, Vanderbilt University Medical Center.
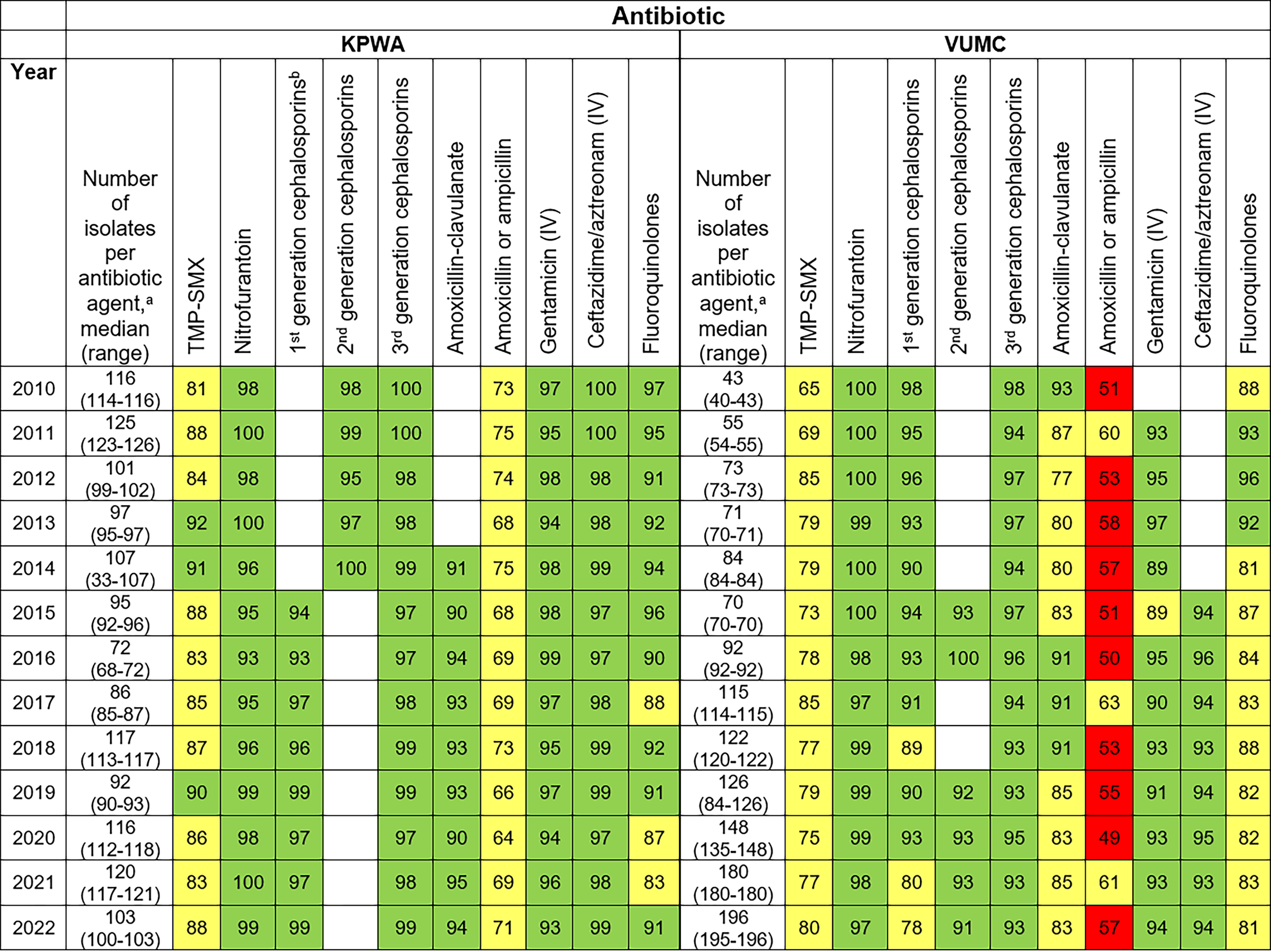
Antibiogram: percentage of E. coli urinary tract infection samples susceptible to antibiotic agents by year, 2010–2022. We used green to denote high susceptibility (≥90%), yellow for moderate susceptibility (60–89%), and red for low susceptibility (<60%). aThe number of isolates tested varied for different antibiotics; we present the median and range tested for each antibiotic, separately for each bacterium. Cells with <30 isolates are left blank, and range (minimum–maximum) and medians are only calculated out of non-blank cells. bIn KPWA, we included results for first generation cephalosporins only in 2015 and later, because prior to 2015, cephalothin was used to test susceptibility for first generation cephalosporin. When evidence was published that this was not a good surrogate for first generation cephalosporin susceptibility, the surrogate was changed to cefazolin in 2015. 11 KPWA, Kaiser Permanente Washington; VUMC, Vanderbilt University Medical Center.
Bacterial susceptibility to antibiotic agent used
The vast majority of UTIs with a positive culture result were treated with an antibiotic that was a “good match” (KPWA: 93%, VUMC: 95%, Table 2). Over time, the percentage of UTIs susceptible to the antibiotic used was relatively consistent, with some evidence of a slightly higher percentage of KPWA UTIs treated with an antibiotic that was a “good match” after 2016 than in earlier years (Fig. 5).
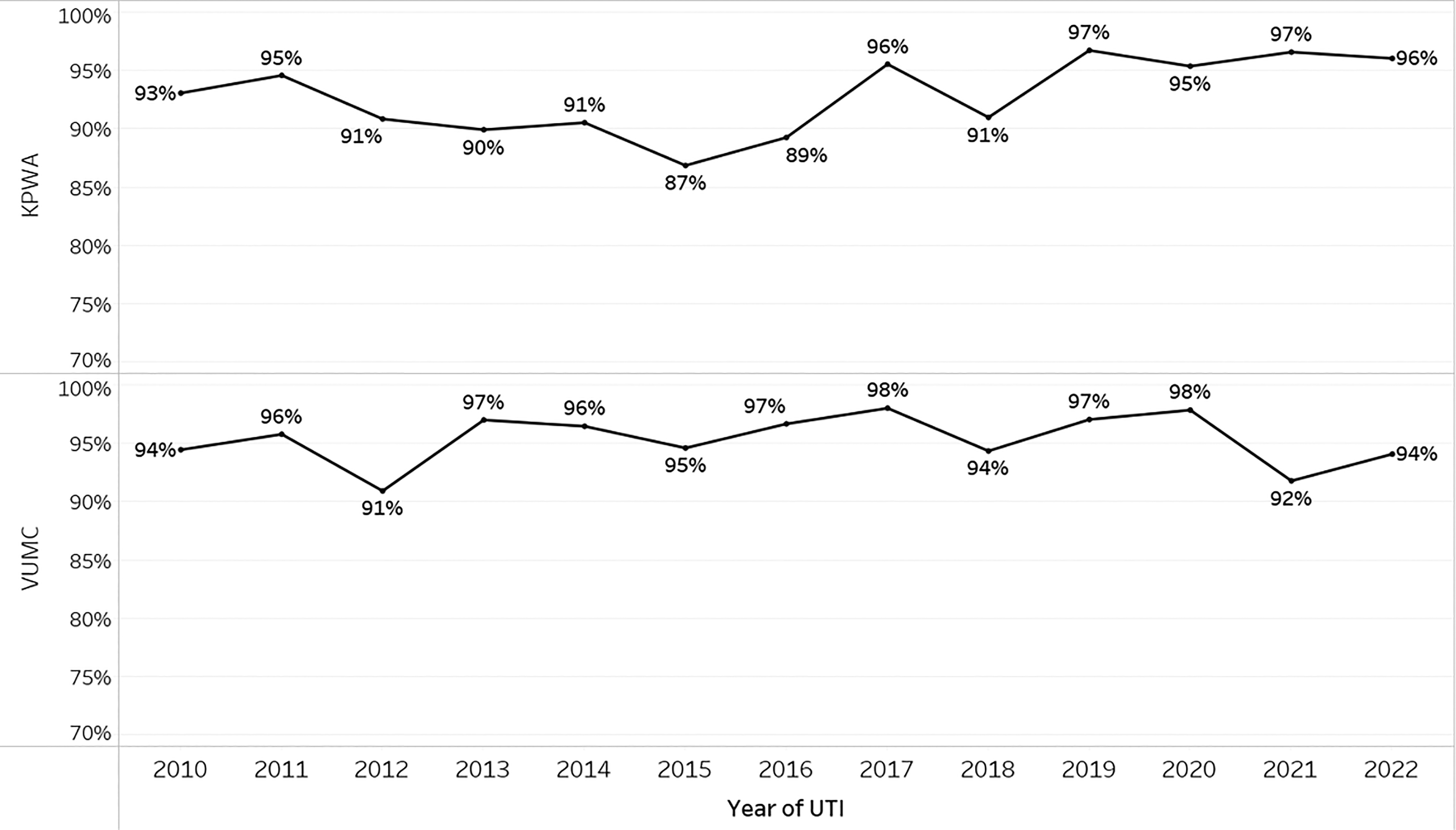
Proportion of urinary tract infections in pregnancy treated with an appropriate antibiotic susceptibility match by year, 2010–2022. In KPWA, we included results for first generation cephalosporins only in 2015 and later, because prior to 2015, cephalothin was used to test susceptibility for first generation cephalosporin. When evidence was published that this was not a good surrogate for first generation cephalosporin susceptibility, the surrogate was changed to cefazolin in 2015. 11 KPWA, Kaiser Permanente Washington; UTI, urinary tract infection; VUMC, Vanderbilt University Medical Center.
Antibiotic Susceptibility Match with Agent Dispensed or Prescribed
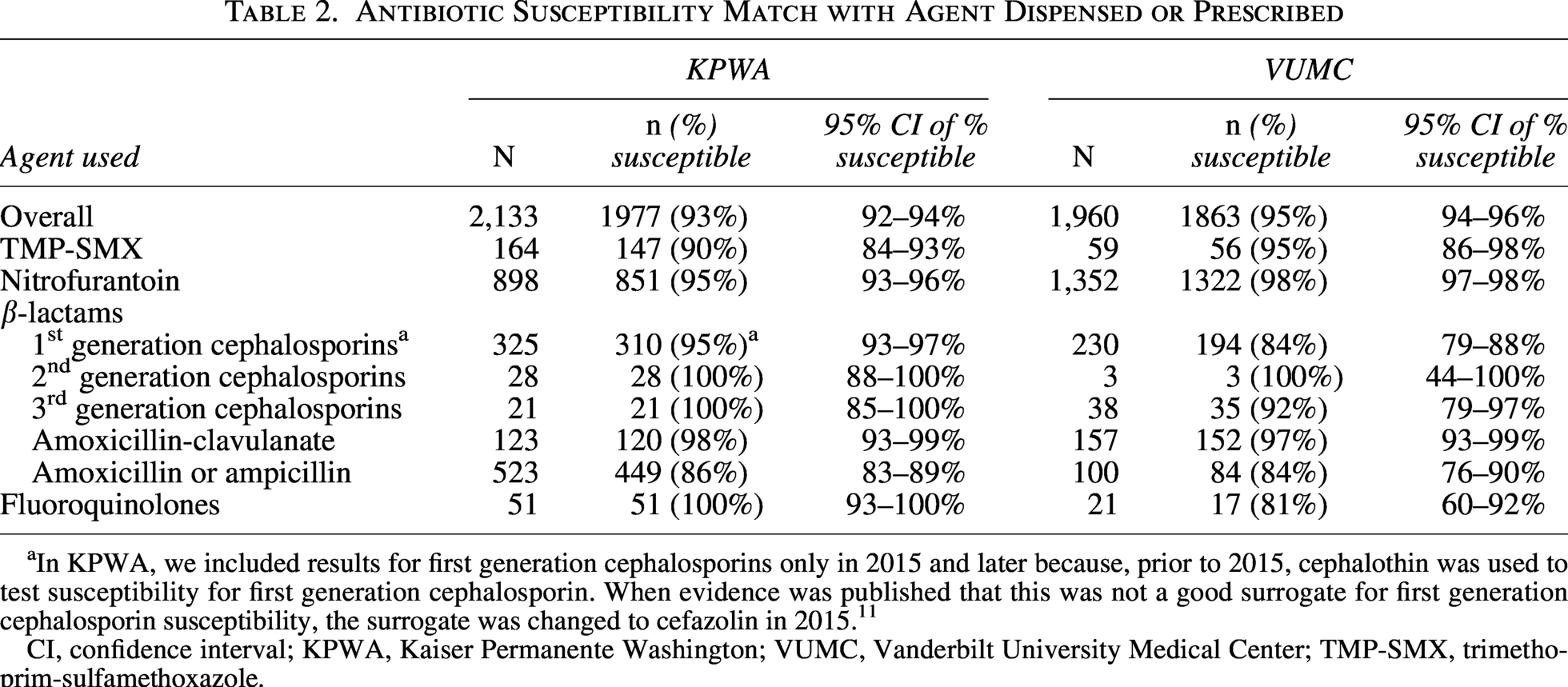
In KPWA, we included results for first generation cephalosporins only in 2015 and later because, prior to 2015, cephalothin was used to test susceptibility for first generation cephalosporin. When evidence was published that this was not a good surrogate for first generation cephalosporin susceptibility, the surrogate was changed to cefazolin in 2015. 11
CI, confidence interval; KPWA, Kaiser Permanente Washington; VUMC, Vanderbilt University Medical Center; TMP-SMX, trimethoprim-sulfamethoxazole.
Discussion
In this study of two health systems in different US regions, the most common antibiotics used for UTI in pregnancy were nitrofurantoin followed by first generation cephalosporins. Use of nitrofurantoin decreased substantially from 2010 to 2022, while use of first generation cephalosporins increased. Susceptibility of E. coli (accounting for 75% of UTIs) to nitrofurantoin was high at both sites. Susceptibility to first generation cephalosporins and amoxicillin–clavulanate was high at KPWA but only moderate at VUMC. Susceptibility results for E. coli were relatively stable over time. Importantly, both health systems used antibiotics that were a “good match” in terms of susceptibility for almost all prescriptions (93–95%).
The most recent published US study of antibiotic utilization for prenatal UTI used data on pregnancies from over a decade ago (2014) and did not assess patterns over time. 12 This study was consistent with our study in finding that nitrofurantoin and first generation cephalosporins were the most commonly used. Not restricting to a pregnant population, a large study of male and female individuals from Kaiser Permanente Southern California (KPSC) from 2016 to 2021 found that first generation cephalosporins were most commonly used to treat UTIs, followed by nitrofurantoin, broadly consistent with our findings. 13 A study of uncomplicated UTIs in nonpregnant women in a nationwide database found that nitrofurantoin use increased from 24% (2015) to 38% (2019), 14 while nitrofurantoin use decreased over that period in our study.
We only identified one recent US study on bacterial susceptibility of UTIs in pregnancy. 15 This small study (n = 259 with positive E. coli urine culture) was conducted from 2013 to 2019 in a single health system in North Carolina. The authors observed very high susceptibility to nitrofurantoin, similar to our findings. Susceptibility to amoxicillin or ampicillin was moderate in their study, as at KPWA, although it was low at VUMC. First-generation cephalosporin susceptibility was high in KPWA, but only moderate in the North Carolina study and VUMC.
Not restricting to pregnant people, we identified previous studies of bacterial susceptibility of UTIs in female populations in the US, including the aforementioned KPSC study 13 and another large study that used laboratory data across the US from 2011 to 2019. 16 These studies' findings were generally consistent with our findings: susceptibility to nitrofurantoin was high, susceptibility to cephalosporins, largely first generation, was moderate-to-high, and susceptibility to TMP-SMX was moderate. Susceptibility remained relatively constant over time in these studies and ours, except for first generation cephalosporin susceptibility decreasing recently at VUMC.
In our study, the observed decrease in nitrofurantoin use over time may have been due to increasing concern over congenital malformations. In 2011, ACOG offered guidance raising concern about the potential that nitrofurantoin (and TMP–SMX) may increase risk of congenital malformations, suggesting that these antibiotics should be avoided in the first trimester if alternatives were available. 5 Current ACOG guidance maintains this recommendation. 1 Interestingly, the temporal decrease in nitrofurantoin use was also present in the second and third trimesters, when exposure would not cause malformations. Providers may prescribe based on the broad message that nitrofurantoin may not be safe in pregnancy, without focusing on the relevant time window. Our analysis by provider type and specialty suggested this trend of decreasing use of nitrofurantoin over time was not driven by a particular provider type or specialty but instead occurred more broadly.
Susceptibility appeared to be lower at VUMC than KPWA, including for first generation cephalosporins, amoxicillin or ampicillin, and amoxicillin–clavulanate. This aligns with previously observed lower E. coli susceptibility in the Southeastern US than in the Pacific Northwest. 16 This may have contributed to the higher proportion of UTIs treated with nitrofurantoin at VUMC than at KPWA, since there were fewer alternative antibiotics to which E. coli had acceptable susceptibility.
Another factor that may have impacted prescribing, in addition to concerns over congenital malformations and susceptibility, is differing side effect profiles of specific antibiotic agents.
By understanding patterns in prescribing practice and antimicrobial sensitivity, we can identify what additional research is required. Avoidance of nitrofurantoin in the first trimester due to potentially increased risk of congenital malformations is based on inconclusive evidence;5,17–19 more studies are needed to understand if nitrofurantoin conveys a true increased risk of malformations. Additional research should assess whether treatment with agents with lower susceptibility, potentially resulting in persistent infection, is associated with a greater risk of adverse events (e.g., pyelonephritis, preterm birth, low birth weight).
Strengths of this study include a larger sample size than previous studies of this topic, the ability to characterize longer-term temporal trends, and the use of recent data. We included two health systems in geographically distinct areas, with different prescribing practices, and notably different distributions of racial and ethnic identities and socioeconomic status. UTI outcomes were defined using multiple clinical data sources, including antibiotic dispensings/orders, diagnoses, and laboratory data in the EHR.
This study has several limitations. Results may be subject to misclassification of UTI status. We defined UTIs based on an antibiotic dispensing plus either a UTI diagnosis or a positive laboratory result; we did not require positive culture results for all UTIs. We also used a cutoff of ≥10,000 CFU/mL to define positive cultures, instead of the clinical guideline-recommended definition of ≥100,000 1 ; this choice is aligned with data from our sites showing that a substantial minority of UTIs treated in pregnancy had a bacterial count from 10,000 to ≤100,000 CFU/mL. At KPWA, we may not have captured UTIs before our cohort’s enrollment cutoff (20 weeks) or for which individuals paid out-of-pocket for antibiotics such that we did not have an insurance claim for the dispensing. For VUMC, we could not capture UTIs treated outside of that health system. We did not have laboratory susceptibility results for all UTIs. Our findings may be biased to the degree that antibiotic treatment and susceptibility results that we were not able to capture were systematically different from those in our study. We included only the first UTI per pregnancy; findings may not generalize to later UTIs. Antibiotic treatment and bacterial susceptibility patterns observed in our two health systems may not be nationally representative.
Conclusions
Data from two health systems in geographically diverse regions suggest that the vast majority of UTIs in pregnancy are being treated with a medication to which they are susceptible. However, we also observed large shifts away from nitrofurantoin despite it having the best coverage for UTIs in pregnant individuals, and toward first generation cephalosporins despite them only having moderate susceptibility at VUMC. This shift may have been due to studies raising concerns about fetal malformations associated with nitrofurantoin use in the first trimester, although, as noted in the ACOG guideline, 1 evidence about risks of nitrofurantoin remains inconclusive. Further research and guideline development should explore how to weigh the potential benefits of nitrofurantoin (increased effectiveness, fewer adverse outcomes due to persistent infection) against the potential for increased risk of fetal malformations, in the context of inconclusive evidence about malformation risk. Effective treatment of UTIs in pregnancy is critical to prevent adverse maternal and fetal outcomes that can result from persistent infection.
Authors’ Contributions
P.D.W. contributed to the conceptualization, methodology, validation, writing the original article draft, and reviewing and editing the article. S.F. contributed to the methodology, software programming, data validation, data investigation, formal analysis, data curation, reviewing and editing the article, and data visualization. L.B. contributed to the software programming, data validation, data investigation, data curation, review and editing the article, and data visualization. S.S. contributed to the conceptualization, methodology, software programming, data validation, reviewing and editing the article, and supervision of data analysis. K.B.N. contributed to the conceptualization, methodology, software programming, data validation, and reviewing and editing the article. M.J.D. contributed to the conceptualization, methodology, and reviewing & editing the article. S.S.O. contributed to the conceptualization, methodology, and reviewing and editing the article. S.M. contributed to the data validation and reviewing and editing the article. A.M.B. contributed to the conceptualization, methodology, reviewing & editing the article, providing supervision, and acquiring the funding. S.D. contributed to the conceptualization, methodology, reviewing and editing the article, and providing supervision. All authors read and approved the final article.
Ethics Approval and Consent to Participate
The study was approved by the KPWA and the VUMC Institutional Review Boards (with waivers of consent).
Consent for Publication
A waiver of consent for using patients’ data were granted by the KPWA and the VUMC Institutional Review Boards.
Supplemental Material
sj-docx-1-jwh-10.1177_15409996261463319 — Supplemental material for Patterns of Antibiotic Utilization and Bacterial Susceptibility of Prenatal Urinary Tract Infections
Supplemental material, sj-docx-1-jwh-10.1177_15409996261463319 for Patterns of Antibiotic Utilization and Bacterial Susceptibility of Prenatal Urinary Tract Infections by Paige D. Wartko, Sharon Fuller, Lisa Bastarache, Susan M. Shortreed, Katelin B. Nickel, Michael J. Durkin, Sarah S. Osmundson, Sandra McAteer, Anne M. Butler, and Sascha Dublin
Footnotes
Acknowledgments
The authors thank Xinnan Niu for his programming work with the VUMC databases. The authors thank Robin Garcia for her contributions as a project manager on their study team.
Availability of Data and Materials
The datasets generated and analyzed during the current study are not publicly available due to patient privacy and confidentiality concerns, but may be available from the corresponding author upon reasonable request. Investigators wishing to obtain the analytic dataset should contact the corresponding author. Requests will be reviewed on a case-by-case basis and may require funding to support programming to create the necessary de-identified analytic dataset(s) and establish a data transfer agreement and Institutional Review Board approval. Any data shared will honor the original data use agreements between study sites.
Author Disclosure Statement
P.D.W. and S.D. worked on a research project supported by GSK. P.D.W., S.D., and S.M.S. have worked on projects funded by Syneos Health, representing a consortium of pharmaceutical companies. S.M.S. has worked on grants awarded to Kaiser Permanente Washington Health Research Institute by Bristol Meyers Squibb and by Pfizer. A.M.B. has received investigator-initiated research funding from Merck & Co. No other authors have personal or financial disclosures relevant to this article.
Funding Information
This work was supported by the National Institute of Child Health and Human Development of the National Institutes of Health (NIH) R01HD107083 (PI, Butler).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.