
Abstract
Research Question:
What is the current lifetime prevalence of infertility in the U.S., and how do U.S. adults view access to in vitro fertilization (IVF) and state-mandated insurance coverage?
Design:
Cross-sectional data were analyzed from a nationally weighted online survey of 1,000 U.S. adults in November 2024. Survey-weighted descriptive statistics estimated lifetime infertility prevalence and support for the right to access IVF and for state-mandated IVF insurance coverage. Survey-adjusted chi-square tests assessed differences in support across sociodemographic groups.
Results:
The sample included adults aged 18–87 years (median age 51 years). Lifetime infertility prevalence was 8.9% (95% CI: 7.2–11.0). Most respondents supported IVF access for infertility patients (74.2%; 95% CI: 70.9–77.2), and approximately two-thirds supported state-mandated IVF insurance coverage (64.6%; 95% CI: 61.2–67.7). Support for IVF access varied significantly by age (p = 0.04), education (p < 0.01), income (p < 0.01), race/ethnicity (p = 0.01), political leaning (p < 0.01), and infertility experience (p < 0.01). Lower support was observed among adults ages 18–29 and 30–49, those with lower income or educational attainment, Black respondents, Independents/Independent-leaning respondents, and individuals without personal or secondhand infertility experience. Support for state-mandated IVF insurance coverage varied by education (p < 0.01), income (p < 0.01), political leaning (p < 0.01), and infertility experience (p < 0.01), with the lowest support among respondents with lower income or education, Republican/Republican-leaning respondents, and those without infertility experience.
Conclusions:
Approximately 1 in 11 U.S. adults has experienced infertility. Although support varied across demographic and political groups, most Americans support IVF access and insurance mandates.
Keywords
Introduction
In vitro fertilization (IVF) is financially burdensome for many Americans due to the lack of federal requirements for insurance coverage and wide variation in state laws. 1 Only 25 states require insurance coverage for infertility services, and just 15 mandate IVF coverage specifically. 1 The absence of comprehensive insurance places the financial burden entirely on patients, unlike many other medical treatments where insurance offsets much of the expense. As a result, access to IVF has become a focus of high-profile federal policymaking efforts,2,3 including President Trump’s February 2025 Executive Order to study how costs can be lowered. 2
Despite recent policy discussions, Americans’ personal experiences with infertility remain underexplored. The National Survey of Family Growth (1982–2010) estimated that 9% of men and 11% of women of reproductive age experienced fertility challenges. 4 Additionally, 12–15% of couples are unable to conceive after 1 year of unprotected intercourse. 4 However, these estimates and others5,6 may not fully capture those who experience infertility or otherwise may need access to IVF for family building (e.g., single individuals, same-sex couples). Traditional clinical definitions of infertility are often centered on heterosexual intercourse and may not fully reflect the experiences of all individuals who seek fertility treatment or assisted reproduction. 4
A 2024 Pew Research Center poll found that 70% of U.S. adults support IVF access. 7 A separate 2024 Gallup poll found that 82% consider IVF morally acceptable, with higher approval among Democrats. 8 A 2017 national survey found that approximately half of Americans supported private insurance coverage of IVF. 9 Additional peer-reviewed studies have explored attitudes toward infertility insurance coverage among specific populations. A 2023 national survey found that although most respondents generally supported infertility insurance coverage, support varied substantially for marginalized populations, including LGBTQ+ individuals, immigrants, and people with disabilities. 10 Additionally, a national survey of Society for Assisted Reproductive Technology members found broad support for expanding insurance coverage for assisted reproductive technologies across several patient populations and clinical scenarios, such as fertility preservation for cancer patients and transgender patients. 11 However, less is known about nationally weighted public support for state-mandated IVF insurance coverage and how these attitudes vary across sociodemographic groups in the current U.S. policy environment.
Given that traditional clinical definitions of infertility are often centered on heterosexual intercourse and may not fully capture all individuals who seek fertility treatment or assisted reproduction, this study aimed to provide a broader estimate of lifetime infertility prevalence and assess public support for IVF access and state-mandated insurance coverage. Sociodemographic comparisons across outcomes were examined to contextualize findings and inform future advocacy and research. We hypothesized that public opinion would vary by political affiliation.
Materials and Methods
Study population
Data were drawn from the Verasight American Public Health Association (APHA) Omnibus Survey, a national online survey weighted to approximate the demographic and political composition of the U.S. adult population, fielded among adults aged ≥ 18 years from November 19 to November 22, 2024. 12 Verasight designed and administered the full survey instrument and conducted all recruitment, sampling, and data collection procedures. The survey included 2,000 respondents randomly assigned to two modules (n = 1,000 per module), each containing a subset of survey questions (≈29 items). The present study’s items appeared in Module A. Because Verasight predetermined the module size (n = 1,000), the analytic sample size was not set a priori and no de novo power calculation was performed.
All respondents were recruited from the Verasight Community, composed of individuals recruited via random address-based sampling and random person-to-person text messaging, supplemented by online outreach. 12 Community members were verified through multi-step authentication (including SMS verification with a major U.S. carrier and within-survey bot-prevention such as reCAPTCHA v3). 12 Verasight implements pre- and post-fieldwork data-quality procedures, including attention, speeding, and straight-lining checks; confirmation of U.S. IP addresses; and removal of duplicate or low-quality responses. 12 Respondents receive compensation (e.g., digital payments or gift cards) for invited surveys. 12
Verasight provided post-stratification weights aligning the module to October 2024 Current Population Survey benchmarks for age, race/ethnicity, sex, income, education, region, and metropolitan status, and to population benchmarks for partisanship and 2020 presidential vote. 12 All estimates and tests applied these weights. The margin of sampling error, accounting for design effect and using the classical random-sampling formula, was ± 3.4% for Module A. 12 This level of precision is consistent with accepted standards for national prevalence estimation in probability-based surveys.
The Verasight APHA Omnibus survey was prospectively designed and fielded by Verasight as part of their standard survey operations. Analysis of these publicly available data did not require Institutional Review Board approval. This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors. This article was prepared in accordance with the STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) guidelines for observational studies.
Of note, the study intentionally included adults across the full age range. The goal was not to estimate infertility risk exclusively among individuals who have completed their reproductive years, but rather to assess the proportion of U.S. adults who had ever experienced infertility at the time of the survey. Individuals who have not attempted pregnancy do not meet the clinical definition of infertility, so their inclusion does not introduce bias into the lifetime prevalence estimate. Instead, it accurately reflects the true population-level proportion of adults who have ever experienced infertility.
Primary outcome measures
Respondents were asked whether they, their partner, someone they knew, or no one they knew had ever experienced infertility, defined as the inability to conceive after 12 months of unprotected intercourse (6 months for those 35+) or requiring medical interventions (e.g., IVF). Lifetime infertility prevalence was defined as selecting self/partner.
Support for infertility patients’ right to pursue IVF was assessed via a multiple-choice question with four response options: (1) yes, with no restrictions; (2) yes, but with some restrictions (e.g., unused embryos cannot be discarded); (3) no; and (4) unsure. Responses were dichotomized as “support” (1 or 2) versus “do not support” (3 or 4) to improve interpretability, reduce the influence of small or ambiguous categories (e.g., “unsure”), and allow for cleaner demographic comparisons.
Support for state-mandated insurance coverage of assisted conception (example.g., IUI and IVF) was assessed with a 5-point Likert item ranging from strongly support to strongly oppose. Responses were dichotomized as “support” (strongly or somewhat support) versus “do not support” (neutral, somewhat oppose, or strongly oppose). Survey items are shown in Figure 1. The Omnibus survey did not include a parallel item on coverage limited to non-IVF assisted conception (for example, IUI only); therefore, a direct comparison between non-IVF coverage and IVF coverage was not possible.
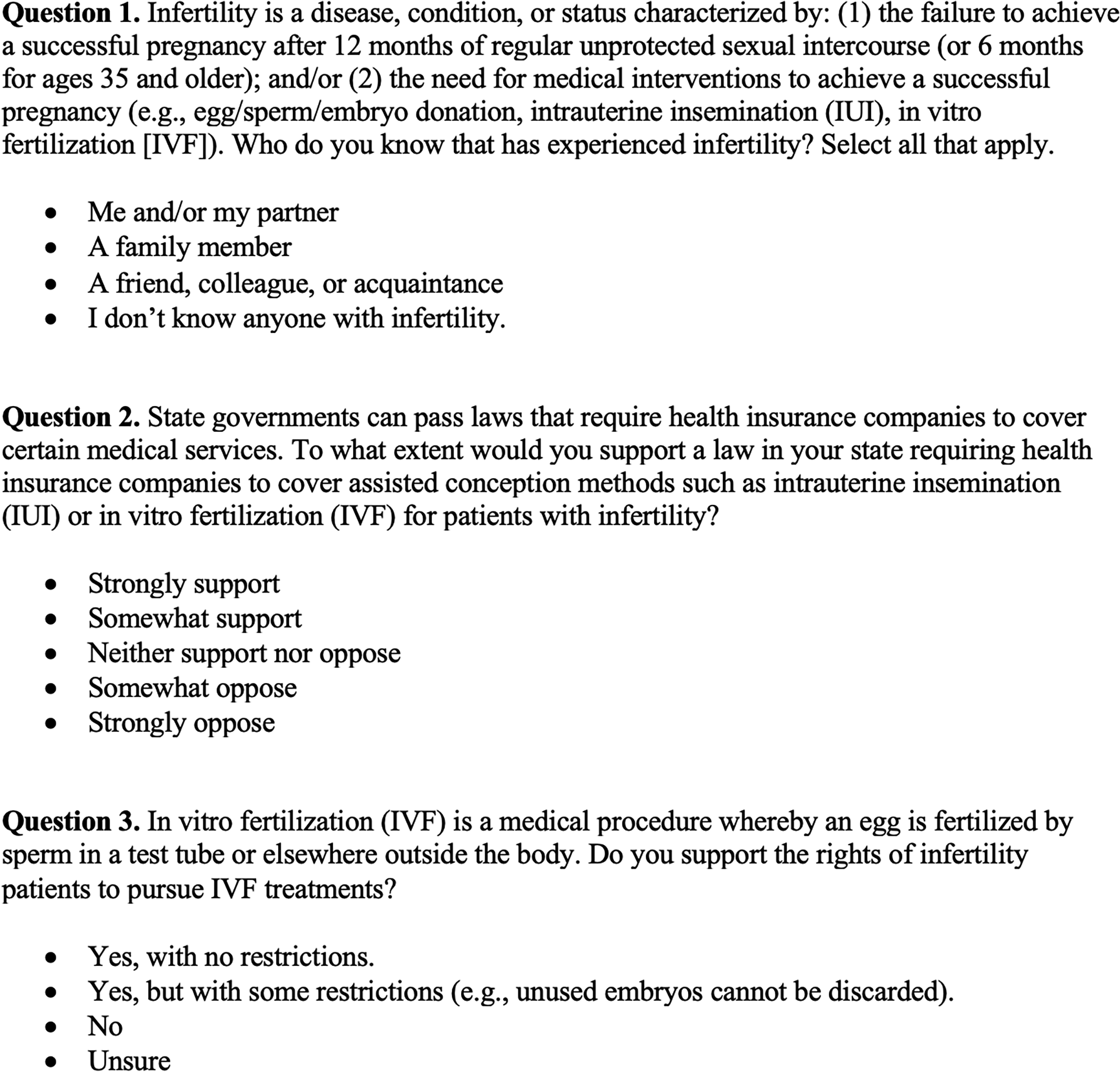
The three infertility questions from the 2024 Verasight Omnibus Survey used in the present analysis on lifetime infertility prevalence and public opinion on accessing fertility treatments for infertility patients among a nationally weighted sample of 1,000 United States adults.
Statistical analysis
Weighted proportions were estimated for all primary outcomes, along with weighted cross-tabulations to examine differences by age, gender, education, income, race and ethnicity, political leaning, region, and urbanicity. Race/ethnicity and income variables reflected the harmonized categorizations provided in the Verasight analytic dataset, including a dichotomized household income variable (<$50,000 vs. ≥$50,000). Chi-square tests, adjusted for complex survey design, assessed differences in outcomes across sociodemographic groups. Analyses were conducted in StataBE version 18. 13
Results
The median age of participants was 51 years (range: 18–87). Approximately half of respondents had at least a four-year college degree (Table 1). Three-quarters reported annual incomes exceeding $50,000 and resided in metropolitan areas. Sex and region were approximately evenly distributed across response categories.
Sociodemographic and Geographic Characteristics for a Sample of 1,000 United States Adults Randomly Selected from the Verasight Community for the Verasight Omnibus Survey
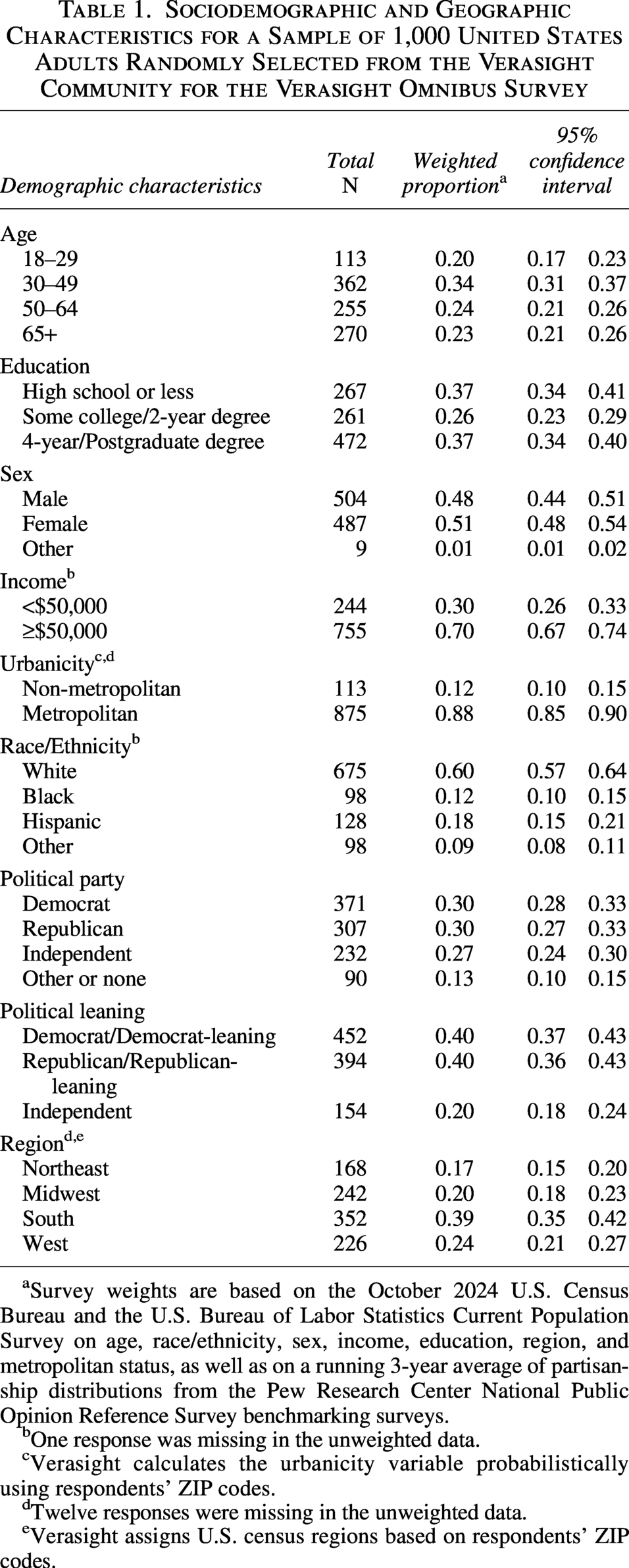
Survey weights are based on the October 2024 U.S. Census Bureau and the U.S. Bureau of Labor Statistics Current Population Survey on age, race/ethnicity, sex, income, education, region, and metropolitan status, as well as on a running 3-year average of partisanship distributions from the Pew Research Center National Public Opinion Reference Survey benchmarking surveys.
One response was missing in the unweighted data.
Verasight calculates the urbanicity variable probabilistically using respondents’ ZIP codes.
Twelve responses were missing in the unweighted data.
Verasight assigns U.S. census regions based on respondents’ ZIP codes.
Lifetime infertility prevalence was 8.9% (95% CI: 7.2–11.0) (Table 2) and was highest among ages 30–49 (11.2%; 95% CI: 8.2–15.0), followed by 50–64 (10.9%; 95% CI: 7.5–15.4), 18–29 (6.7%; 95% CI: 3.2–13.6), and 65+ (5.5%; 95% CI: 3.3–8.9). Prevalence varied significantly by income (< $50,000: 5.3%, ≥ $50,000: 10.4%, p = 0.02), urbanicity (non-metropolitan: 16.8%, metropolitan: 7.9%, p < 0.01), and political leaning (Democrats: 6.1%, Republicans: 9.6%, Independents: 13.0%, p = 0.02) (Table 3).
Selected Questions and Weighted a Tabulations from the Verasight Omnibus Survey about Lifetime Infertility Prevalence and Public Opinion on Accessing Fertility Treatments for Infertility Patients among a National Sample of 1,000 United States Adults
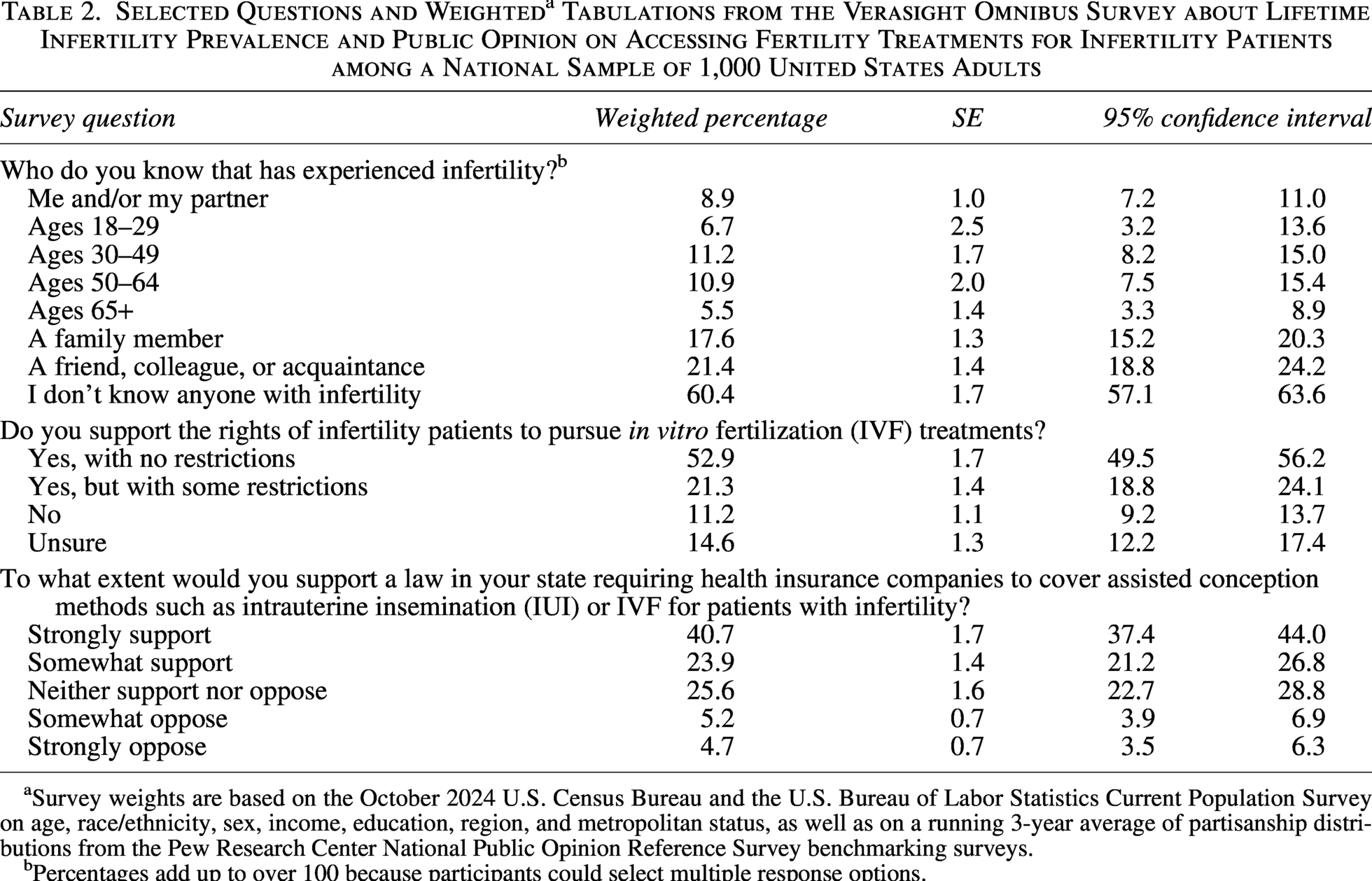
Survey weights are based on the October 2024 U.S. Census Bureau and the U.S. Bureau of Labor Statistics Current Population Survey on age, race/ethnicity, sex, income, education, region, and metropolitan status, as well as on a running 3-year average of partisanship distributions from the Pew Research Center National Public Opinion Reference Survey benchmarking surveys.
Percentages add up to over 100 because participants could select multiple response options.
Weighted a Data Tabulations Displaying Infertility Prevalence by Various Sociodemographic Characteristics among a Nationally Weighted Sample of 1,000 United States Adults
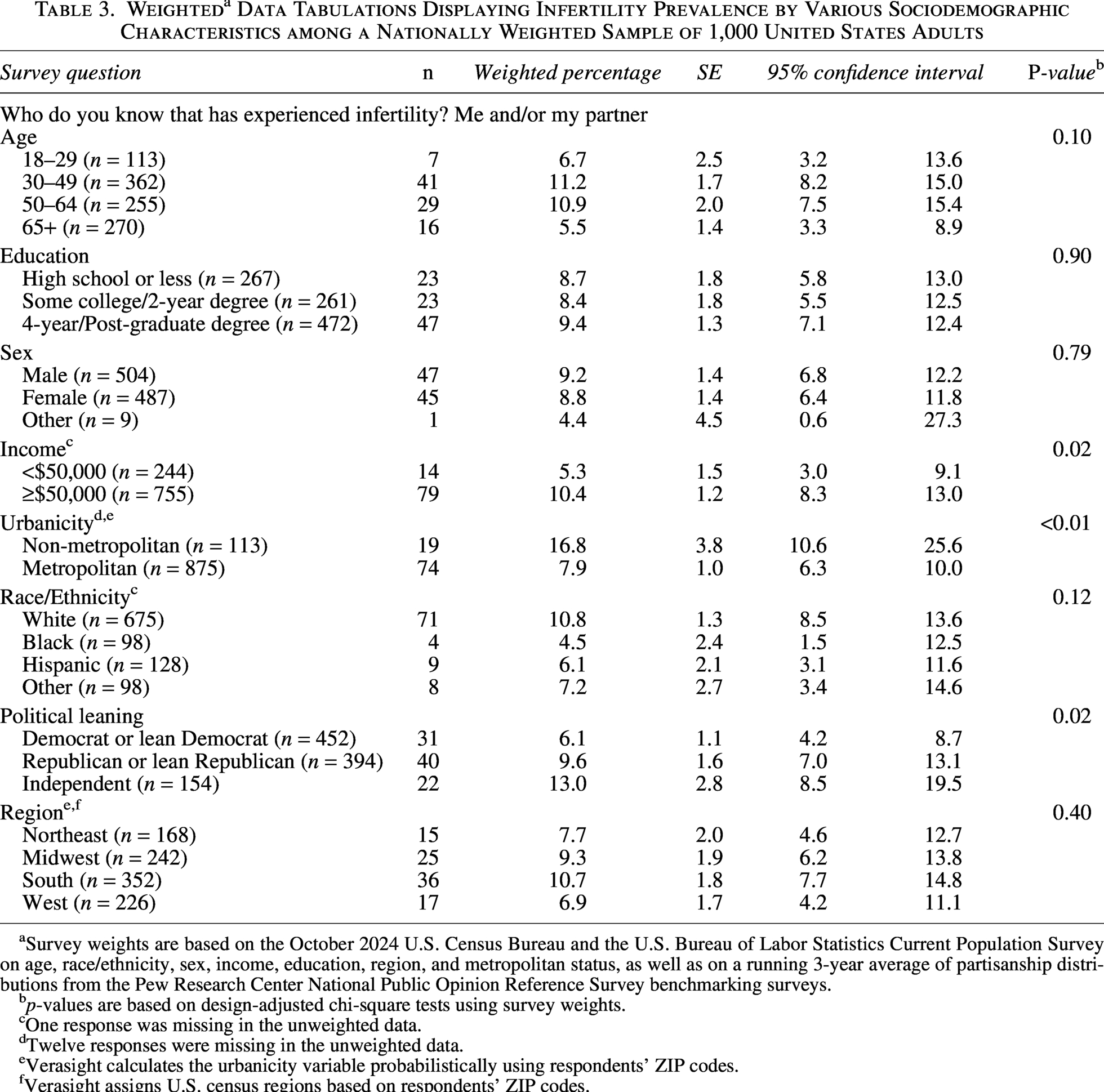
Survey weights are based on the October 2024 U.S. Census Bureau and the U.S. Bureau of Labor Statistics Current Population Survey on age, race/ethnicity, sex, income, education, region, and metropolitan status, as well as on a running 3-year average of partisanship distributions from the Pew Research Center National Public Opinion Reference Survey benchmarking surveys.
p-values are based on design-adjusted chi-square tests using survey weights.
One response was missing in the unweighted data.
Twelve responses were missing in the unweighted data.
Verasight calculates the urbanicity variable probabilistically using respondents’ ZIP codes.
Verasight assigns U.S. census regions based on respondents’ ZIP codes.
Nearly 75% of respondents supported the right to pursue IVF with no (52.9%; 95% CI: 49.5–56.2) or some restrictions (21.3%; 95% CI: 18.8–24.1) (Table 1). Sixty-five percent (95% CI: 61.2–67.7) supported state-mandated insurance coverage of IVF. Over half of Democrats and Republicans supported each outcome (Tables 4 and 5).
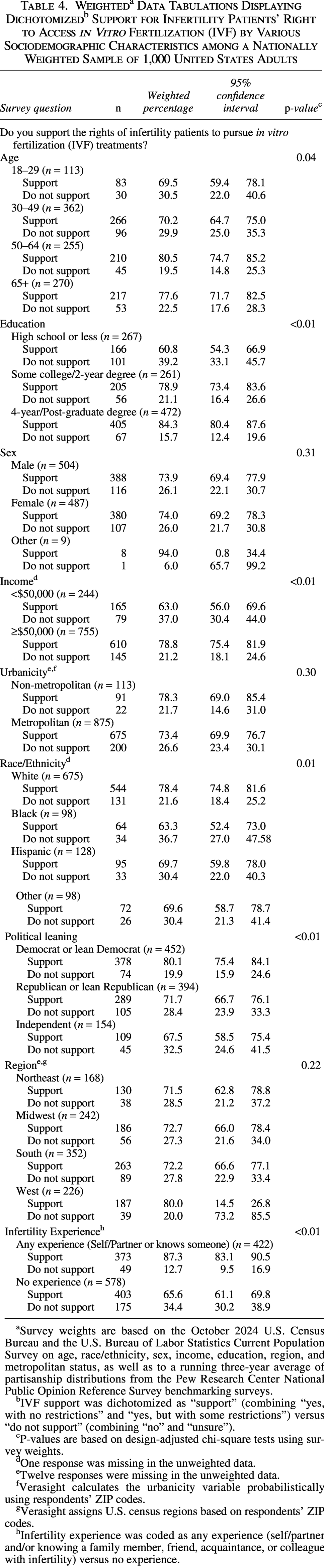
Survey weights are based on the October 2024 U.S. Census Bureau and the U.S. Bureau of Labor Statistics Current Population Survey on age, race/ethnicity, sex, income, education, region, and metropolitan status, as well as to a running three-year average of partisanship distributions from the Pew Research Center National Public Opinion Reference Survey benchmarking surveys.
IVF support was dichotomized as “support” (combining “yes, with no restrictions” and “yes, but with some restrictions”) versus “do not support” (combining “no” and “unsure”).
P-values are based on design-adjusted chi-square tests using survey weights.
One response was missing in the unweighted data.
Twelve responses were missing in the unweighted data.
Verasight calculates the urbanicity variable probabilistically using respondents’ ZIP codes.
Verasight assigns U.S. census regions based on respondents’ ZIP codes.
Infertility experience was coded as any experience (self/partner and/or knowing a family member, friend, acquaintance, or colleague with infertility) versus no experience.
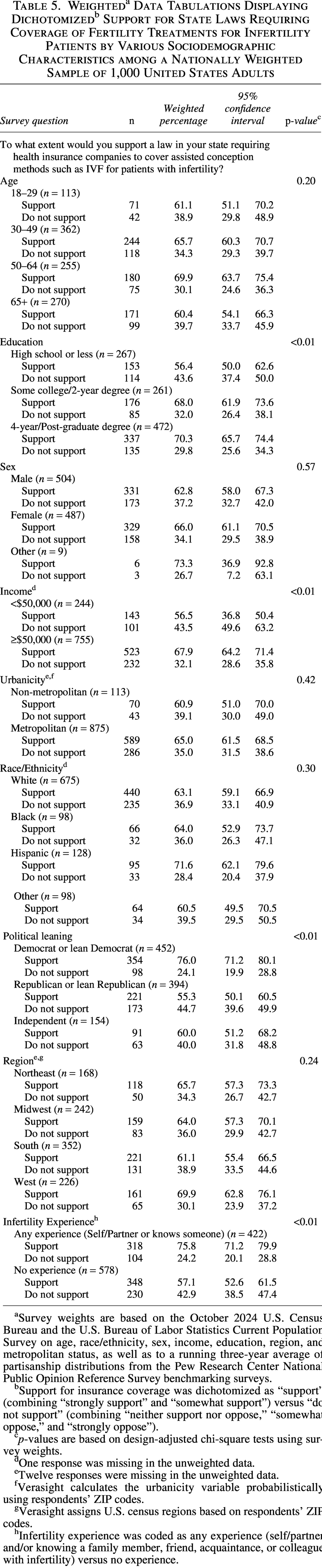
Survey weights are based on the October 2024 U.S. Census Bureau and the U.S. Bureau of Labor Statistics Current Population Survey on age, race/ethnicity, sex, income, education, region, and metropolitan status, as well as to a running three-year average of partisanship distributions from the Pew Research Center National Public Opinion Reference Survey benchmarking surveys.
Support for insurance coverage was dichotomized as “support” (combining “strongly support” and “somewhat support”) versus “do not support” (combining “neither support nor oppose,” “somewhat oppose,” and “strongly oppose”).
p-values are based on design-adjusted chi-square tests using survey weights.
One response was missing in the unweighted data.
Twelve responses were missing in the unweighted data.
Verasight calculates the urbanicity variable probabilistically using respondents’ ZIP codes.
Verasight assigns U.S. census regions based on respondents’ ZIP codes.
Infertility experience was coded as any experience (self/partner and/or knowing a family member, friend, acquaintance, or colleague with infertility) versus no experience.
Support for IVF access varied significantly by age (p = 0.04), education (p < 0.01), income (p < 0.01), race/ethnicity (p = 0.01), political affiliation (p < 0.01), and infertility experience (p < 0.01) (Table 4). Lowest levels of support were observed among respondents ages 18–29 (69.5%; 95% CI: 59.4–78.1) and 30–49 (70.2%; 95% CI: 64.7–75.0), those with lowest levels of educational attainment (60.8%; 95% CI: 54.3–66.9) or income (63.0%; 95% CI: 56.0–69.6), Black respondents (63.3%; 95% CI: 52.4–73.0), Independent/Independent-leaning respondents (67.5%; 95% CI: 58.5–75.4), and those who had never experienced nor knew someone who experienced infertility (65.6%; 95% CI: 61.1–69.8).
Support for state-mandated insurance coverage varied significantly by education (p < 0.01), income (p < 0.01), political leaning (p < 0.01), and infertility experience (p < 0.01) (Table 5). Lowest levels of support were observed among those with lowest levels of educational attainment (56.4%; 95% CI: 50.0–62.6) or income (43.5%; 95% CI: 36.8–50.4), Republican/Republican-leaning respondents (55.3%; 95% CI: 50.1–60.5), and those who had never experienced nor knew someone who experienced infertility (57.1%; 95% CI: 52.6–61.5).
Supplementary Tables S1 and S2 present weighted tabulations of support for IVF access and state-mandated insurance coverage across sociodemographic characteristics for original response categories.
Discussion
Principal findings
This national cross-sectional study, which was weighted to approximate the demographic and political composition of the U.S. adult population, provides updated estimates of lifetime infertility prevalence and public support for IVF-related policies in the United States. Nearly 9% of U.S. adults reported experiencing infertility, with prevalence exceeding 11% among those aged 30–64. Support for the right to pursue IVF was high overall (74%), and approximately two-thirds of respondents supported state-mandated insurance coverage for IVF.
Key sociodemographic differences emerged. Infertility prevalence was highest among middle-aged and higher-income individuals, and among those living in nonmetropolitan areas. Support for IVF access and insurance mandates was higher among respondents with greater age, income, and education. Lower levels of support were observed among Black respondents, Independent/Independent-leaning individuals, and those with lower income or educational attainment.
Results in the context of what is known
This study’s lifetime infertility prevalence estimate (8.9%) is lower than the World Health Organization’s (WHO) widely cited global infertility figures. 6 WHO’s pooled global estimates, based on 133 studies and 91 data points, indicate a lifetime prevalence of 17.5% and 12-month (period) prevalence of 12.6%. 6 WHO also notes wide variation across contributing studies due to differences in definitions of infertility, inclusion and exclusion criteria, and measurement approaches, and recommends comparing estimates only when study characteristics are similar. 6 This study’s estimate is based on a single self-report item fielded to all U.S. adults (18+) with a brief definition; this broader denominator and measurement approach likely yield a lower point estimate than pooled studies that often focus on reproductive-age populations.
Consistent with prior evidence,7–11 the majority of Americans supported IVF access and state insurance coverage. Despite partisan differences in support for insurance coverage, both Democrats and Republicans broadly supported the right to pursue IVF. This public approval presents an opportunity for bipartisan policy action, especially amid the elimination of federal reproductive health agencies. 14
Support for IVF access and insurance coverage was higher among individuals with greater income or educational attainment, aligning with past studies suggesting that awareness of and access to assisted reproductive technologies are greater among these groups. 15 In contrast, Black respondents were less likely to support IVF-related policies, which may reflect longstanding mistrust of the health care system, lower rates of IVF utilization, or differing cultural or religious views on fertility treatment. 16 These findings highlight the need for targeted education, culturally sensitive care, and equity-centered policy approaches to ensure that public support translates into inclusive access.
Clinical implications
The estimated lifetime infertility prevalence of nearly 9%, and approximately 11% among adults aged 30–64, underscores the substantial number of U.S. patients likely to require fertility evaluation and treatment. These findings suggest that tens of millions of American adults may seek care for infertility during their lifetimes, reinforcing the need for providers across specialties to be equipped to discuss fertility health, provide referrals, and support access to assisted reproductive technologies.
Increased public support for IVF access and insurance coverage also has direct clinical implications. As policy changes are debated and potentially enacted, more patients may be able to afford and pursue IVF. This could increase the number of people seeing reproductive endocrinologists and raise the need for counseling about treatment options across all levels of care. Obstetrician–gynecologists and primary care providers may also need to stay informed about changing insurance requirements and referral pathways to help patients navigate access to IVF.
At the same time, clinicians should be aware that not all patients have equal access to fertility care or feel equally informed or supported. Disparities in knowledge, access, and trust, especially among lower-income groups, lower-age groups, Black patients, and politically conservative individuals, should be addressed through culturally sensitive education and equitable care strategies.
Research implications
This study highlights the need for continued national monitoring of infertility prevalence and public attitudes toward IVF access and insurance coverage, particularly as reproductive health policy debates continue to evolve. Future research should explore the underlying reasons for variation in IVF support across sociodemographic groups, particularly among Black respondents, lower-income populations, lower age groups, and political Independents, who showed lower levels of support. Qualitative and mixed-methods studies could provide deeper insight into cultural beliefs, perceived barriers, and knowledge gaps related to IVF.
While prior studies have shown that state-mandated insurance coverage is associated with increased IVF utilization and higher live birth rates,17,18 disparities persist. A 2023 study using data from the Society for Assisted Reproductive Technology Clinical Outcome Reporting System from 2014 to 2019 found that racial and ethnic disparities in IVF utilization and outcomes persist regardless of state insurance mandates, indicating that insurance coverage alone is not sufficient to eliminate inequities in infertility care. 19 Additional research is needed to evaluate more recent policy changes, assess long-term effects, and identify structural and sociocultural factors that limit equitable access. Health communication research may also help identify effective strategies to increase awareness and reduce stigma around infertility and IVF.
Personal experience with infertility was associated with greater support for both IVF access and state-mandated insurance coverage. Individuals with personal or secondhand experience with infertility may have heightened awareness of the financial, emotional, and logistical burdens associated with fertility care, which may shape their policy preferences. This finding highlights the importance of involving patients and patient advocacy organizations in efforts to improve infertility care and expand insurance coverage. Patients’ lived experiences offer critical insight into the barriers that impede access, and their engagement in policy discussions, alongside clinicians, researchers, and professional societies, can strengthen advocacy efforts and help ensure that policies reflect the realities of those most affected.
Strengths and Limitations
Strengths
This study has several strengths. It used a national sample with survey weighting to reflect the demographic and political composition of the U.S. adult population. The timing of data collection, which occurred shortly after several high-profile policy developments related to IVF, adds to the relevance of these findings for ongoing legislative debates. These developments included a federal executive order focused on lowering the cost of IVF, 3 as well as a White House announcement highlighting agreements with manufacturers to reduce the cost of commonly used fertility drugs. 20 Additionally, the study employed a broader infertility definition that incorporated both traditional clinical criteria and the need for medical intervention (e.g., IVF), which may have allowed respondents to consider a wider range of fertility-related experiences.
Limitations
However, several limitations should be noted. First, although recruitment was address-based with multi-step verification and results were weighted to national benchmarks, online participation may still skew toward more computer-active respondents; residual selection and nonresponse bias are therefore possible. If individuals who are more digitally engaged are also more aware of or more supportive of IVF and insurance coverage, our estimates could overstate national support even after weighting. Second, because the module size was fixed at n = 1,000, precision and statistical power for subgroup comparisons (i.e., design-adjusted chi-square tests) were limited, especially for smaller groups (e.g., race/ethnicity), so some differences may not reach statistical significance (potential Type II error). Third, the unweighted sample skewed toward higher educational attainment relative to U.S. population benchmarks; post-stratification weighting reduced this imbalance, but residual differences may remain. Fourth, infertility prevalence may be underestimated, as nearly half the sample was under age 45 and may not have completed their reproductive years yet, though age-stratified estimates were provided. Prevalence may also be underestimated because the sample included older adults who were more likely to have completed childbearing at younger ages 21 and therefore may have been less likely to experience age-related infertility. Fifth, multivariable regression models were not estimated due to concerns about survey item comprehension and response interpretation. Some respondents may not have fully understood distinctions between IVF access and insurance coverage or the meaning of state mandates. Such misunderstandings could introduce measurement error that affects both adjusted and unadjusted analyses. Although descriptive subgroup comparisons remain informative, these potential sources of misinterpretation should be considered when interpreting the findings. Sixth, the Omnibus survey did not include a parallel item on public support for insurance coverage for assisted conception other than IVF (e.g., IUI), precluding a direct comparison between non-IVF coverage and IVF coverage. Seventh, although recruitment incorporated address-based sampling and weighting to national benchmarks, the online omnibus design may not fully replicate the characteristics of a traditional probability-based survey sample. Additionally, detailed survey response and completion rate metrics were not publicly available from Verasight, limiting the ability to fully assess potential nonresponse bias. Finally, the survey did not capture reasons for IVF support or opposition. Future research should disentangle public support for general infertility coverage (e.g., diagnostics, medications, surgery, IUI) versus IVF-specific coverage (given potential differences driven by high IVF costs and ethical considerations) and use larger samples and qualitative methods to explore underlying reasons.
Conclusions
This nationally weighted study finds broad public support for both IVF access and state-mandated insurance coverage, suggesting a favorable policy climate for expanding fertility care. However, gaps in support across age, racial, educational, income, and political lines underscore the need for targeted education and culturally responsive communication. To advance reproductive health equity, efforts must focus not only on reducing financial barriers but also on building public trust and awareness, particularly among historically underserved communities. As IVF access becomes a central issue in national policy debates, ensuring that public health responses are inclusive, data-driven, and equity-oriented is more critical than ever.
Authors’ Contributions
L.C. conceptualized the study, conducted the formal data analysis with assistance from M.K.P., curated the data, managed the project, and wrote the original draft of the article. A.G. provided supervision and oversight of the research. M.K.P., J.K., and A.G. reviewed and edited the article. All authors read and approved the final article.
Ethical Considerations
This study analyzed publicly available, de-identified data and did not involve interaction with human participants or access to identifiable private information. As such, the study did not constitute human subjects research and did not require approval from an Institutional Review Board or ethics committee.
Consent for Publication
Not applicable. This study did not include identifiable individual-level data, images, or videos.
Supplemental Material
sj-docx-1-jwh-10.1177_15409996261467343 — Supplemental material for Infertility Prevalence and Public Support for In Vitro Fertilization Policies in the United States
Supplemental material, sj-docx-1-jwh-10.1177_15409996261467343 for Infertility Prevalence and Public Support for In Vitro Fertilization Policies in the United States by Leah E. Chapman, Mary Kathryn Poole, Jennifer F. Kawwass, and Audrey J. Gaskins
Supplemental Material
sj-docx-2-jwh-10.1177_15409996261467343 — Supplemental material for Infertility Prevalence and Public Support for In Vitro Fertilization Policies in the United States
Supplemental material, sj-docx-2-jwh-10.1177_15409996261467343 for Infertility Prevalence and Public Support for In Vitro Fertilization Policies in the United States by Leah E. Chapman, Mary Kathryn Poole, Jennifer F. Kawwass, and Audrey J. Gaskins
Footnotes
Consent to Participate
Not applicable. This study analyzed publicly available, deidentified data and did not involve interaction with human participants.
Data Availability
Author Disclosure Statement
The authors declare no potential conflicts of interest with respect to the research, authorship, and publication of this article.
Funding Information
The authors received no financial support for the research, authorship, and publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.