
Abstract
Introduction
Methods
Results
Conclusion
Introduction
The ultimate goal of aortic endovascular repair (EVAR) is to successfully exclude the aneurysm preventing expansion and rupture. Endoleak is defined as residual aneurysm blood flow outside the endograft and can be identified in as many as 50% of patients after EVAR.1–5 Although the significance of endoleaks is an ongoing controversy, the expansion of the aneurysm sac size is a concern that usually requires intervention. Although many aneurysms with endoleak continue to shrink after EVAR, some endoleaks lead to aneurysm expansion.
Color duplex ultrasound (CDU) is effective in the identification of endoleak and the assessment of abdominal aortic aneurysm (AAA) morphology after EVAR when compared with computed tomography (CT).6–9 CDU is cost-effective, noninvasive, and can be repeated without exposure to contrast agents. A thorough protocol in the hands of an experienced technologist will achieve optimal results. 6 However, even in experienced laboratories, the use of CDU after EVAR is challenging and extremely dependent upon the abilities of the technologist.
With obstacles such as body habitus and bowel gas, low-flow endoleaks can be difficult to detect. Although a previous study has suggested that low-velocity endoleaks (specifically Type II endoleaks) will likely seal spontaneously, 10 we have discovered a subset of patients with low-flow endoleaks that result in significant AAA expansion. These patients have a characteristic B-mode appearance to their AAA sac by CDU with a low-flow Type II endoleak that is difficult to detect by either CDU or CT scan.
Methods
A retrospective review of all patients with EVAR devices, including Ancure® (Guidant Co. Indianapolis, IN), AneuRx® (Medtronic, Minneapolis, MN), Zenith® (Cook, Bloomington, IN), and Quantum® (Cordis, Warren, NJ), were followed with CDU for evaluation of endoleak during a 5-year period. Routine follow-up of patients was performed at least annually and since 2001, more than 700 scans have been performed in our laboratory. All CDU exams were performed by registered vascular technologists using Philips 5000, 3000, and IU22 systems with 2.25- to 5-MHz curved-array or phased-array transducers. Patients fasted for 6 to 8 hr before the examination. A thorough assessment of the AAA sac with spectral and color Doppler was used to identify endoleak according to published protocol. 6 Endoleak within the AAA sac was confirmed with spectral Doppler, and the waveform was categorized as bi-directional, biphasic, or monophasic as described by Carter et al. 11 The source of the leak was identified and categorized into endoleak classification Type I-Type IV. 12 B-mode evaluation of the residual AAA sac was characterized for echogenicity and sac symmetry and measured for orthogonal transverse diameter.
All patients were evaluated using CT scan and/or angiography for confirmation of endoleaks. CT scan protocol consisted of a 3-mm slice thickness and a pitch of 2 mm. Three separate imaging examinations were performed: precontrast run for the identification of opacities; a contrast run beginning 20 sec after the start of an infusion of contrast; and an immediate post-contrast run for delayed imaging in search of late branch vessel endoleaks. CT scan was diagnostic for endoleak if contrast was visualized exterior to the endograft but within the aneurysm sac.
Results
There were 12 patients with subtle Type II endoleaks and a characteristic heterogeneous B-mode texture by CDU identified from 1 month to 16 months after intervention. The endoleaks had very low velocities within the aneurysm sac, ranging from 10 to 50 cm/sec with a bidirectional spectral Doppler waveform. Most of velocities identified in this group were less than 20 cm/sec. An asymmetrical residual aneurysm sac with a “spongy” multiechogenic texture was a finding in all 12 patients at the time of CDU endoleak detection (Figure 1A–B). These endoleaks were difficult to detect by CDU because of the low velocities. (Figure 2A–B). The suspicious B-mode appearance of the AAA sac was an important clue to the technologist to thoroughly search for the endoleaks with sensitive color and Doppler settings and with multiple approaches and planes. All CDU aneurysm sac measurements had increased in size or remained unchanged compared with the prior CDU at the time of endoleak detection. At the time of intervention, the average AAA sac size increase compared with the previous CDU was 4.4 mm.

A, B-mode image of “spongy” echogenicity texture. B, Color duplex ultrasound of multiechogenic “spongy” texture.
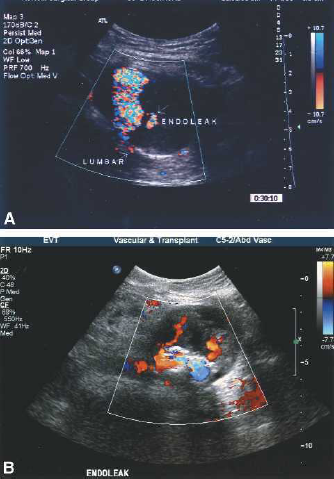
A, Subtle slow-flow endoleak within aneurysm sac. B, Pananeurysmal endoleak within “spongy” echogenicity area of residual aneurysm sac.
CT scan failed to detect endoleak in 6 of 12 patients positive for endoleak by CDU despite residual sac enlargement. In one of these patients, select angiography also failed to identify endoleak at the time of intervention. This patient ultimately had the endograft explanted almost 3 years after placement with conversion to open repair because of significant aneurysm expansion. Select angiography described lumbars coursing toward the residual aneurysm but without identification of contrast within the residual sac. An ultrasound contrast study according to protocol and using Optison® (GE Healthcare Technologies, Waukesha, WI) confirmed the CDU findings of endoleak despite the negative CT and angiography. Ultrasound contrast has been shown to decrease the threshold for endoleak detection. 13 The AAA sac at the time of open repair was described as “gelatinous” and inflammatory by the surgeon.
Seven of the 12 patients eventually required intervention to repair their endoleaks as the result of expansion of the residual sac. Five of the seven patients had coiling and/or fibrin glue of the AAA sac with recurrent Type II lumbar endoleak in all five patients. Three of the seven patients underwent exploratory laparotomy with lumbar ligation. In two of the three patients, near systemic pressure was directly measured in the residual aneurysmal sac before intraoperative identification using CDU and subsequent ligation of the offending lumbar artery. Two of the three open interventions had a successfully resolved endoleak, determined by CDU and CT scan, and one patient had a persistent Type II lumbar endoleak detected by CDU that is being followed conservatively. One of the five patients with unsuccessful coiling of the AAA sac died as the result of unrelated causes, and the remaining patients are being followed conservatively at this time.
Discussion
EVAR is becoming an accepted alternative to standard open aortic aneurysm repair. The challenge has been in managing endoleak around a functioning endovascular graft. Any exposure of the residual aneurysm sac to arterial flow represents a potential for aneurysm expansion and possibly rupture.
AAA sac enlargement after EVAR would suggest persistent pressurization of the residual sac.14,15 Some endoleaks expose the residual aneurysm sac to systemic pressures and result in sac expansion, whereas other endoleaks are benign and the sac continues to shrink appropriately. 1 A phenomenon that has been poorly understood is endotension, 16 which is defined as aneurysm expansion in the absence of detectable endoleak. Some studies have suggested that endotension actually represents missed endoleak.17,18 The fact that the low flow endoleaks in our small series were difficult to detect by CDU and were missed by CT scan (and by angiography in one patient) would support the belief that endotension may be missed endoleak.
Although the use of EVAR is increasing rapidly, the routine use of CDU remains controversial as a reliable modality for detecting endoleak. 19 Some centers may not want to invest in such a time-consuming and technically challenging examination. High-end ultrasound equipment is required for an optimal CDU examination, as well as sonographers who are experienced in visceral vascular imaging. There is a long learning curve associated with becoming proficient in accurately performing these exams and a thorough knowledge of the various EVAR devices is essential. In the hands of a skilled sonographer, CDU endoleak detection is comparable with CT scan.4–6 However, we have found that in this subset of patients with very low flow endoleaks, asymmetrical aneurysm sac with enlargement and a spongy heterogeneous sac texture, the endoleaks are much more difficult to detect. The important B-mode residual aneurysmal sac characteristics are helpful in alerting the sonographers to be diligent in assessing for endoleak. The similarity of these CDU B-mode findings between all 12 patients is remarkable. What also is concerning is the significant aneurysmal sac enlargement in all 12 patients in which the endoleaks were not defined by CT scan or angiography. Seven of the 12 patients required significant secondary intervention to attempt to repair the persistent endoleaks.
Conclusion
CDU after EVAR can effectively detect the presence of endoleak and assess the B-mode characteristics of the AAA sac. Important clues such as sac asymmetry and a “spongy” heterogeneous B-mode appearance are consistent with subtle, low flow endoleak that may predict AAA expansion. When undetected, this type of endoleak may be diagnosed as endotension. Careful follow-up with CDU combined with CT scan for AAA enlargement should be performed in all patients after EVAR, especially when they have these CDU characteristics. In the presence of aneurysm expansion with these B-mode characteristics identified, undefined endoleak must be considered. Perhaps ultrasound contrast would be helpful in further defining this very subtle but clearly dangerous type of endoleak.