
Abstract
Introduction
Subintimal angioplasty (SIA) is the endovascular recanalization of vessels in the subintimal plane and most often is used to treat long-segment occlusions involving the femoropopliteal segment. This study demonstrates the value of pre- and postprocedural color duplex ultrasound (CDU) imaging.
Methods
Forty-three subintimal angioplasty procedures were performed to treat lower-extremity arterial occlusions. CDU was used as the definitive imaging modality in all cases. There were 26 women and 17 men, with a mean age of 76 years. Sixteen patients had anklebrachial index < 0.45. Most patients had significant medical comorbidities, placing them at high risk for arterial bypass procedures.
Results
In all patients, the extent of the occlusion was accurately diagnosed with CDU before intervention. SIA was technically successful in 42 of 43 patients (98%). The postprocedure CDU follow-up (1–2 months) demonstrated 10 patients had reoccluded (24%). Our primary patency rate was 42% at 30 months.
Conclusion
SIA can be an effective method of treatment in aged, high-risk patients with lower-extremity ischemia and threatened limb loss. CDU accurately locates the site of and measures the length of arterial occlusions in such patients, allowing the interventionalist to plan the site of arterial puncture and to prognosticate the likely success. CDU obviates the need for diagnostic angiography and remains the modality of choice for surveillance after SIA intervention.
Introduction
The advent of duplex ultrasonography has not only been a major breakthrough in the noninvasive diagnosis of arterial disease, but it has revolutionized the preoperative assessment and postoperative surveillance of patients undergoing arterial intervention either by surgical or radiological means. The accuracy of duplex ultrasound for the identification of significant lesions and the ability to differentiate stenosis from occlusion has been well documented. The addition of color flow and parallel technological improvement in ultrasound imaging units together with cumulative worldwide sonographer experience has allowed reasonably rapid duplex evaluation of long arterial segments such that many surgeons and endovascular specialists are now able to dispense with diagnostic angiography before planning intervention on aortoiliac and peripheral arteries.
The technique of endovascular recanalization of occluded arterial segments by the use of subintimal angioplasty is a relatively recent innovation that initially was performed by Bolia et al. 1 in Leicester, United Kingdom, in 1987. In that color duplex ultrasound (CDU) imaging ideally is suited to the diagnosis of arterial occlusions, particularly in the femoropopliteal segment, its potential for use as the definitive diagnostic tool before subintimal angioplasty is obvious. The purpose of this study is to demonstrate the importance and reliability of pre- and postprocedural CDU, and we detail here our initial results with the subintimal recanalization technique using CDU as the definitive diagnostic tool before intervention.
Materials and Methods
Between January 2001 and October 2004, 43 patients were submitted for the subintimal recanalization of 43 occluded femoropopliteal arterial segments. Using standard laboratory testing protocols, we performed continuous-wave Doppler waveform analyses, anklebrachial indices (ABIs), and color duplex ultrasound imaging on all 43 patients before intervention. Examinations were performed in a standard manner on Philips HDI 5000 Sonos CT or HDI 3500 color flow imaging units using a 7-4 MHz linear array transducer (Advanced Technology Laboratories, Bothel, WA).
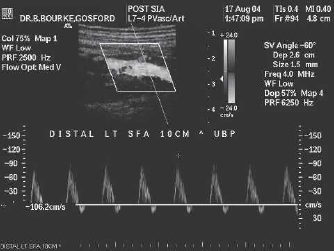
Complete occlusion was diagnosed where an imaged segment had no flow identified by color and spectral Doppler, collateral outflow was demonstrated at the point of occlusion, and there was collateral inflow at the point of vessel reconstitution (Figure 1). The spectral waveform distal to the occlusion identified was of low velocity and monophasic in nature (Figure 2). The location and length of the occlusion was measured using the upper border of the patella as the definitive landmark, and this was recorded in centimetres.2,3
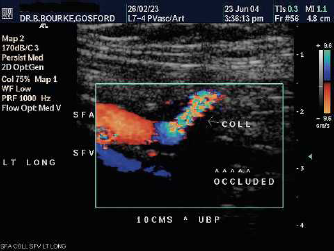
Color duplex imaging of occluded distal superficial femoral artery segment with outflow collateral at point of occlusion.
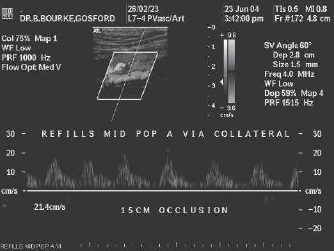
Doppler spectral waveform distal to occlusion at point of reconstitution (same case as Figure 1).
Subintimal angioplasty was performed under local anesthesia in all cases with the aid of a 6-French sheath placed percutaneously either prograde into the ipsilateral common femoral artery (CFA) or antegrade in the contralateral CFA. In the latter case, a longer sheath placed up and over the aortic bifurcation replaced the first sheath if greater stability was needed during subintimal passage of the guide wire. An angled nonstiff 0.035″ Terumo Glidewire (Terumo Medical Corporation, Somerset, NJ) and a supporting straight 5-French flushing catheter (Merit Medical Systems Inc., South Jordan, UT) were used to create a subintimal dissection plane at the level of the occlusion. The wire was made to form a redundant loop at its distal end which, in effect, acted as a cutting edge to separate the subintimal layers as the loop was advanced distally. In the initial part of the recanalization, the loop was kept long to allow maximal separating efficiency. If the loop met resistance and forced the supporting catheter to move in a cephalad direction, the supporting catheter was replaced with a balloon angioplasty catheter so that the balloon could be expanded just proximal to the point of resistance to prevent proximal dislodgement and to allow further advancement of the loop (Figure 3).
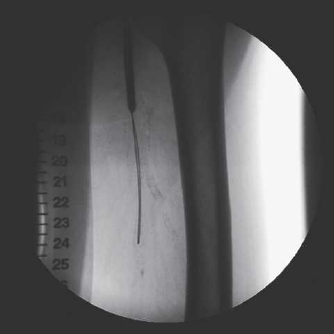
Angioplasty catheter containing guide wire with balloon inflated proximal to occlusion to stabilize wire and formation of loop in proximal left superficial femoral artery.
As the proposed re-entry point was approached, the loop was shortened to allow a maximal spring effect so that the wire would tend to spring back in through the intimal layer to the patent lumen (Figure 4). If re-entry could not be achieved, the wire was replaced with a stiff Terumo Glidewire (Terumo Medical Corporation, Somerset, NJ), which would usually successfully allow re-entry into the true lumen if the softer wire had failed. Re-entry was heralded by sudden loss of resistance and unlooping of the wire. The supporting catheter (or balloon catheter if that had been used) was advanced to just beyond the re-entry point into the true lumen. The wire was then removed. If a brief suction noise was heard as the wire was removed, it usually meant that the true lumen had not been reached. Successful re-entry usually was heralded by free back-dripping of fresh blood through the catheter lumen. Re-entry was confirmed by performing an angiogram through the catheter, at which time runoff vessels also were checked. The subintimal plane was then expanded from distal to proximal by multiple dilatations of a balloon catheter (usually 5 mm balloon diameter). Wire control was maintained until completion angiography through the proximal sheath confirmed patency of the canalized subintimal segment, absence of distal emboli, and preservation of preprocedural runoff vessels.

Same case as Figure 3. The guide wire loop is being advanced distally in the subintimal plane.
Hemostasis was achieved either with an angioseal (St Jude Medical Inc, Minnetonka, MN) or digital groin pressure. The procedures were performed after intra-arterial unfractionated heparin (approximately 70 IU/Kg) had been administered, which was left non-reversed. Patients were instructed to continue preprocedural antiplatelet agents.
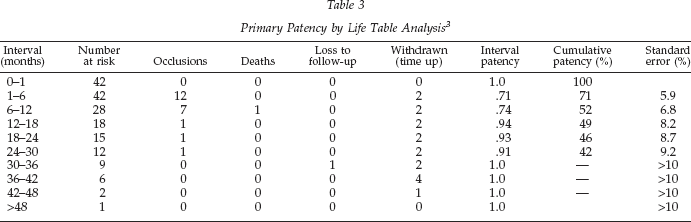
Procedural success was defined as successful subintimal canalization of the occluded segment in continuity with the patent inflow and outflow vessel. Continuing patency was defined as the persistence of this patent channel whether subsequent narrowing occurred or not. Patency rates were calculated according to standards recommended by Rutherford et al. 4 Because of relatively small numbers only primary patency rates have been calculated.
Results
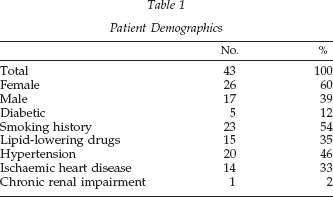
There were 26 women (60%) and 17 men (39%) with a mean age of 76 years (range, 50–95). Patient demographic characteristics are shown in Table 1. Preprocedural symptomatology and ABI information is shown in Table 2. All patients in this study had occlusive lesions in the femoropopliteal segment accurately diagnosed with CDU before intervention when correlated with the arteriogram performed at the time of the procedure. Wire re-entry to the true lumen could not be achieved in 1 case, the patient subsequently requiring arterial bypass. Immediate procedural success, therefore, was 98% (42 of 43), leaving 42 patients for subsequent follow-up evaluation. Of the 42 patients there were two patients who had previous occluded femoropopliteal bypass grafts. More than 90% had moderate-to-severe ischemia and more than 30% had limb threatening reduction in blood flow. Primary patency by life table analysis is shown in Table 3. Primary patency was 42% at 30 months, beyond which standard error exceeded 10%.
Patient Demographics
Preprocedural Symptoms and Hemodynamics
Previous occluded femoropopliteal bypass grafts.
Primary Patency by Life Table Analysis 3
At the initial follow up (1–2 months) 10 segments had reoccluded and a further 12 reoccluded during further follow up. Of these 22 eventual reocclusions, 19 also had ABI assessed postreocclusion. Of these, only 3 showed worsening of the ABI by greater than 0.10 compared with the preprocedural ABI. Of these 3 patients, only 1 required arterial bypass. A further 3 showed improvement in ABI by greater than 0.10 despite the reocclusion. The ABI in the remaining 13 essentially were unchanged. Of the 32 segments still patent on color flow duplex scanning at the first post-procedural visit, 22 had ABI increasing to the normal range (>0.8), 6 had increased to between 0.7 and 0.8, and 3 remained at less than 0.7. Five patients came to arterial bypass, one of which occluded within 6 months. Further angioplasty was performed in another five patients, three of which were successful. One patient died of unrelated causes at 11 months. No patient came to amputation.
Discussion
We have found CDU extremely reliable in the diagnosis and mapping of arterial occlusions in the femoropopliteal segment. It allows the efficient one-step planning of the intervention avoiding preprocedural diagnostic angiography. With knowledge of the degree of proximity of the occlusion to the origin of the superficial femoral artery, the proceduralist is able to plan either an ipsilateral prograde femoral entry or a contralateral antegrade femoral entry. By accurate mapping of the level of distal reconstitution, the proceduralist has excellent knowledge of how much “normal” patent artery he has to work with to gain re-entry into the true lumen. This information allows full explanation of the chance of success and possible complications of the procedure to the patient before deciding to proceed. In the case of long occlusions, even on-table angiography may not give good views of the reconstituting vessel or the tibial runoff whereas CDU usually can provide this information with good-to-excellent accuracy. Additional benefits of CDU include mapping of the long saphenous vein in case urgent bypass is required and the postoperative surveillance of both the recanalised segment and the entry point of the sheath (Figures 5 and 6).

Patent distal superficial femoral artery after SIA (same case as Figure 1).
Doppler spectral waveform of patent distal superficial femoral artery after SIA (same case as Figure 1).
Subintimal angioplasty is a relatively recent evolving technique. We have found it a useful, safe, minimally invasive procedure, which can relieve disabling symptoms in aged, frail patients with multiple comorbidities. Our immediate technical success rate of 98% compares favorably with others.5–8 In the context of the patient population treated (i.e., aged with multiple comorbidities), the primary patency rate of 42% at 30 months is acceptable given that the vast majority were not made any worse and some improved despite reocclusion and further procedures such as angioplasty and bypass were not jeopardized. We and others3,9–15 have shown previously that duplex scanning allows operative intervention for most femoropopliteal and many femorocrural bypasses without the necessity for preoperative diagnostic angiography. We and others also have demonstrated the value and cost-effectiveness of duplex scanning in the surveillance of infra-inguinal arterial saphenous vein bypasses.16–26 This study demonstrates that CDU is also an ideal tool for a one-step diagnosis of and planning for subintimal recanalization of the occluded femoropopliteal segment without the need for preliminary invasive diagnostic angiography. This has beneficial implications not only for cost but also for the convenience of these usually aged and frail patients. CDU is also an ideal, low-cost means of accurately monitoring these patients in the post-procedural phase.