
Abstract
The Screening for Abdominal Aortic Aneurysms Very Efficiently (SAAAVE) Act authorizes Medicare to pay for an ultrasound screening for select patients. We hypothesized that the potential increase in screening would affect the ability of a high-volume medical center to respond to this need. Selection criteria included age >65 years and evidence of or risk factors for cardiovascular and/or atherosclerotic disease. We queried the medical center's information warehouse to define a patient population which, in a retrospective fashion, would have met the aforementioned criteria. We sought to quantify the potential increase in the number of abdominal aortic aneurysm (AAA) ultrasound screenings. There were 29,875 patients who met the inclusion criteria. Upon admission, 476 patients (1.5%) were diagnosed with AAA, and 35 were diagnosed with ruptured AAAs. There were 742 AAA diagnosed at time of discharge, equivalent to a 55.9% increase in prevalence of aneurysms compared with admission diagnoses. Of these, 48 were diagnosed upon discharge after rupture, which was greater than a 37% increase compared with the number diagnosed upon admission. During the study period, the medical center imaging laboratories performed an average of 1700 to 2100 ultrasound scans per full-time equivalent sonographer. Our results suggest that the additional patient volume would be approximately 10,000 patients per year. The SAAAVE Act of 2005 will have a profound impact on health care institutions nationwide.
Introduction
Abdominal aortic aneurysm (AAA) is the 10th-leading cause of death in the United States among men older than 55 years of age, with a mortality rate comparable with those of breast and prostate cancer.1,2 However, AAA is a highly treatable and curable vascular condition for 95% of men and women when it is detected before rupture occurs.1,2 Unfortunately, many patients with AAA typically remain asymptomatic until rupture, after which mortality rates are 80–90%.3–6
One-year mortality rates for untreated AAAs range from 9.4–55%.7,8 Risk factors for AAA include family history, age 65 years or older, cigarette smoking, heart disease, hypertension, diabetes mellitus, and evidence of atherosclerotic disease.1,3,9–13 With appropriate surveillance, early identification of an aneurysm is quite beneficial for those patients whose aneurysms enlarge and reach treatment thresholds.
Multiple studies have demonstrated the poor reliability of physical examination and abdominal palpation for detecting AAAs.14,15 However, ultrasound screening has become increasingly prevalent as a highly sensitive diagnostic tool for screening for AAA.16,17 Ultrasonographic examinations are easy to conduct, reproducible, reliable, and can be completed in a timely manner.15,18
Elective repair of AAA, whether open or endovascular, is safe, with reports citing mortality rates of 2%.19,20 Elective repair is also cost effective19,20; emergent surgical repair of ruptured aneurysms more than doubles the hospital cost as compared with elective repair. 9 From an economic standpoint, a nationwide AAA-screening program has the potential to save millions of dollars currently spent on emergency surgery and postoperative intensive care for patients with ruptured AAAs. The cost per quality-adjusted life-year saved using either a standard ultrasound examination or a quick screening ultrasound examination may be as high as $11,285 and $6,850, respectively. 11 It has been estimated that a cost of $993 to $1173 per life-year saved as a result of AAA screening is one-third the cost per life-year gained from breast and colorectal screening programs21,22 and one-eighth that of cervical cancer screening.23,24
Numerous reports in recent years have supported the rationale for using ultrasound to screen for AAAs. The Screening for Abdominal Aortic Aneurysms Very Efficiently (SAAAVE) Act of 2005 was passed by both Houses of Congress in 2005 and signed into law by President Bush on February 8, 2006.25–27 The law provides that Medicare pay for a one-time ultrasound AAA screening for all individuals greater than 65 years of age, who meet the following criteria: family history of AAA, risk factors for cardiovascular disease (such as smoking or hypertension), evidence of atherosclerotic vascular disease, or other risk factors for AAA. The screening will be provided as part of the Welcome to Medicare physical examination that will be instituted on January 1, 2007.25,26
The authors hypothesized that the potential increase in patients to be screened for AAA would have a substantial impact on the ability of a high-volume medical center to respond to the need. We conducted this retrospective analysis of the clinical effects (RACE) to SAAAVE study to quantify the potential increase in numbers of AAA ultrasound screenings, in order to assist the medical center in meeting this need when the SAAVE act takes effect. (Note: this study was initiated and completed before the SAAAVE Act of 2005 became law. Thus, the underlying assumption guiding the project was that the legislation would eventually be signed into law).
Methods
We queried the medical center's Information Warehouse to define a patient population which, in a retrospective fashion, would have met the aforementioned criteria. Data were queried using Microsoft Access 2000 and then analyzed using Microsoft Excel (Microsoft Corp, Redmond, WA). The university medical center consists of three separate hospitals: the main hospital (UH), a cancer hospital (CH), and another hospital elsewhere in the city (UHE). Data were collected for a 3-year period beginning July 1, 2002, and ending June 30, 2005.
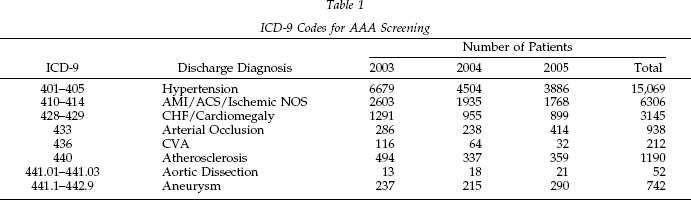
The availability of data regarding past patient information (e.g., history of smoking, positive family history for AAA, etc.) was a limiting factor; thus, the time frame of 3 years was chosen to minimize fluctuation changes in comparison with a single-year study. We selected patients who were 65 years of age or older (Medicare eligible) upon hospital admission. Patients were only selected for inclusion during their first hospital admission during the study time period to eliminate any artificial increase in the statistical outcome of the study, as the reimbursement from Medicare states only one screening is covered per patient. To determine which patients would qualify for the Medicare reimbursable ultrasound screening, we reviewed several methods for identifying this subpopulation of patients at the medical center. Included in these discussions were Diagnosis-Related Group codes, International Classification of Diseases, Ninth edition (ICD-9) codes, and a patient database established by the section of cardiology at the medical center. After consulting several vascular surgeons, cardiologists, and the resource planning analyst at the medical center, we determined that the most cohesive, efficient, and specific coding system would be the ICD-9 codes by which patients were admitted and discharged. The ICD-9 codes would also be used by Medicare, thereby minimizing error. An experienced vascular surgeon and an interventional cardiologist reviewed the complete list of ICD-9 codes to determine the appropriate codes to assess for the stipulations set forth in the SAAAVE ACT of 2005. Risk factors for cardiovascular disease and evidence of atherosclerotic disease were determined to include the ICD-9 codes shown in Table 1. Examples of ICD-9 codes that were removed before the query was completed included those for left bundle-branch block and paroxysmal tachyarrhythmias, as all physicians involved agreed that these were not independent risk factors for cardiovascular disease.
ICD-9 Codes for AAA Screening
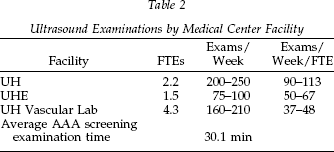
Data collected from the ultrasound laboratory managers of each of three laboratories at the medical center, one vascular and two ultrasound-specific, are shown in Table 2. Numbers were approximated using past data from each department's computer database. The estimated average time to perform a sonographic AAA screening examination was calculated after 10 examinations by an experienced sonographer.
Ultrasound Examinations by Medical Center Facility
Results
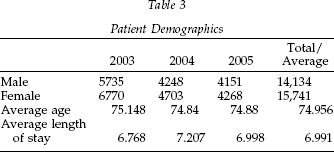
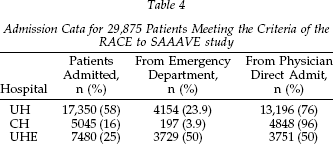
Patient demographics and length of stay data are shown in Table 3. There were 346,044 first-time patients admitted to the medical center during the study period; of these, 8.63% or 29,875 met the criteria to be included in the RACE to SAAAVE study (Table 4). Upon admission, 476 patients (1.5%) were diagnosed with aortic aneurysms. Thirty-five (7.35%), or approximately 11 per study year, were diagnosed with ruptured AAAs upon admission. There were 742 AAAs diagnosed at time of discharge, equivalent to a 55.9% increase in prevalence of aneurysms compared with admission diagnoses. Of the 742 aneurysms, 48 were diagnosed upon discharge after rupture, greater than a 37% increase compared with the number diagnosed upon admission at the medical center. During the 3-year study, 93 patients received an ultrasound procedure on the day of admission. Of these, 91 were completed using either a curvilinear or linear probe. Two patients received a transvaginal and rectal ultrasound. These procedures require an endoluminal probe, which is not appropriate for abdominal imaging or an AAA screening.
Patient Demographics
Admission Cata for 29,875 Patients Meeting the Criteria of the RACE to SAAAVE study
Discussion
The results of this study support the hypothesis that the implications of the new Medicare coverage on The Ohio State University Medical Center (OSUMC) are substantial. Although our objective was to identify implications of the new law, preparing for the additional volume of ultrasound scans will require a review of available resources and a way to satisfy the screening program. The results and implications illustrated within this work reach national significance by quantifying the clinical and financial impact of the SAAAVE Act of 2005 to every medical center caring for Medicare covered patients.
Theoretically, if Medicare had covered the AAA screenings during the study period, the medical center would have been confronted with the opportunity to screen nearly 30,000 additional patients. It is anticipated with the aging of the population—specifically the baby boomers born between 1947 and 1964—after that the number of individuals meeting the criteria to receive this screening will continue to increase. If the average incidence of AAA in the general population is 1–4%,1,11,12 then it can be inferred that this incidence is greater in the “at-risk” population. Research has shown this risk to be as high as 11% in men older than 65. 1 Extrapolating the data from this study, the medical center could have potentially detected 3,286 (29,875 × 11%) AAAs before they ruptured during the past 3 years. Cost savings would also be realized, considering that hospital costs more than double when an AAA is diagnosed after rupture as compared with preventive serial screening examinations and prophylactic repair is pursued.
Currently, the medical center's three hospitals have access and use two ultrasound-specific laboratories and one vascular laboratory. During the past 3 years, these laboratories have performed an average of 1700 to 2100 ultrasound scans per full-time sonographer. The findings of this study suggest that the additional patient volume would be approximately 10,000 patients per year, which equates to about 190–200 additional ultrasound scans per week. At our institution, the average number of scans performed per day per ultrasound technician/FTE averaged over the three labs is 7.3–7.7. The average time to perform a screening ultrasound examination by an experienced sonographer for AAA at the medical center is just over 30 minutes. It must be considered that the screening AAA ultrasound examination does not take as much time as most other examinations that were included in the data collected from the ultrasound labs and therefore it is difficult to quantify the additional load these exams may have on the OSUMC labs. Nevertheless, the new caseload could be more than overwhelming to the current system. Additionally, if the volume of screening AAA examinations increases, it is foreseeable that the time required would decrease over time, as sonographers gain experience (similar to most learning curves). Any prediction at this time to quantify increasing the sonography staff to accommodate this influx of patients is not the aim of this paper; rather, the study has identified that this issue exists and further evaluation will need to be conducted to address this specific issue.
The findings of this study raise a number of questions that must be addressed in a timely fashion for the medical center to be prepared for implementation of the SAAAVE Act on January 1, 2007. We believe the results of this study will also encourage the medical center to proactively embrace the significance of the SAAAVE Act, identify the need for and develop protocol(s) that would benefit the clinical care of patients screened and treated for AAA, and determine whether AAA screening is both fiscally prudent and operationally feasible. How would a medical center feasibly identify the qualified patients who would benefit from the Medicare coverage of an AAA screening? Once identified, how does the medical center staff approach the issue of screening these individuals for AAA? One possible solution to the second question is to use a portable ultrasound screening service. The new generations of portable scanners are compact, cheaper, versatile, and provide high-quality images without the ergonomic disadvantages of large scanners, 28 all of which could potentially allow a larger number of scans of in-patients who qualify for AAA screening.
It is worth noting that an inherent limitation of this study lies in the method of accurately identifying the patient population in question. The medical center's Information Warehouse was unable to modify our search for two particular fields we believed to be prudent: a history of smoking and a positive family history of AAA. Thus, it can only be inferred that the population queried in this study may be smaller than the true number of individuals who would have otherwise qualified for an AAA screening. Although an experienced vascular surgeon and cardiologist meticulously scrutinized the list of ICD-9 codes for which we queried, the resulting list does not represent the exact list that Medicare will use for determining pertinent risk factors.
The relevance of this study extends beyond the scope and practice of this medical center, as the impact of the SAAAVE Act of 2005 will affect health care institutions nationwide. We conducted this study in a manner that would be reproducible by other hospital systems by adjusting for relative size and patient populations. It is the hope of the authors that other health care institutions can determine the impact of the passage of the SAAAVE Act of 2005 will have on the workload and resources within their respective centers.
Footnotes
Acknowledgment
We acknowledge the editorial assistance of Janet L. Tremaine, ELS, Tremaine Medical Communications, Dublin, Ohio.