
Abstract
Introduction
Endofibrosis of the external iliac arteries (IE) occurs in some high-performance athletes, particularly female cyclists, and causes leg pain on extreme exertion. Establishing the diagnosis in these cases is challenging, because a vascular cause is often not suspected initially. The anatomic lesion of IE is difficult to detect with B-mode ultrasound because of the characteristic smooth and diffuse thickening of the arterial wall. Standard treadmill testing can be equivocal in these athletes, but more intense or “extended” treadmill exercise can demonstrate the physiological abnormalities.
Case Report
This report describes our experience with 6 limbs of 4 patients found to have IE and who also underwent surgical intervention to relieve symptoms. All patients had normal resting ankle/brachial indices, except one, who also had iliac artery thrombosis. Duplex scanning showed diffusely increased velocities throughout external iliac segments. The treadmill exam was modified, with speeds ranging from 2.5 to 5.8 mph and exercise times up to 15 minutes required to provoke a significant decrease in ankle pressure. Monophasic, high-velocity postexercise Doppler flow waveforms helped to localize the site of the responsible lesions.
Results
All 6 limbs were treated by enlarging the affected external iliac artery with a vein patch angioplasty (thrombectomy was also performed in one patient). Inspection of the arterial lumen at surgery revealed a smooth, fibrous-appearing lesion with diffuse wall thickening. The 5 limbs, which had postoperative treadmill tests, all had normal results and these patients resumed athletic training. Among 5 limbs with postoperative duplex scans, 2 showed normal vessel diameter, and 3 had a dilated lumen.
Conclusion
Although the mechanism of IE is not known, the typical history and location of the lesions suggests that repetitive stress or bending of the vessels and high flow during extreme exercise leads to thickening of the arterial wall. Awareness of this entity and a modified vascular testing protocol are essential to establishing the diagnosis.
Introduction
There is increasing recognition that high-performance athletes, predominantly female cyclists, can develop symptomatic arterial flow restriction in one or both legs as the result of endofibrosis of the external iliac arteries. These patients provide both a diagnostic and therapeutic challenge. The noninvasive vascular laboratory can play a key role in the identification and management of these patients.
The prevalence of iliac endofibrosis (IE) is not known, largely because the condition often goes unrecognized and not treated appropriately. A delay in diagnosis can result in debilitating symptoms for these elite athletes, with loss of their ability to train and compete. Some have been falsely labeled malingerers, hypochondriacs, or have been encouraged to give up their sport. The lesions of IE are difficult to appreciate with arteriography or duplex ultrasound because of their smooth, diffuse nature (Figure 1). Physiologic testing with pre- and post-exercise pressures provides conclusive diagnostic evidence and may actually be the gold standard for diagnosing this entity. In this series, we report our experience with 7 limbs in 5 patients that underwent noninvasive diagnosis and surgical repair of IE, including long-term follow up data.

Angiogram of the aorto-iliac and proximal femoral arteries, bilaterally. The right external iliac artery is small in caliber; the smooth, diffuse subtle characteristics of the lesion are demonstrated.
Pathophysiology
The pathologic mechanism of IE is not known. However, the common history of patients who exercise vigorously while bent over on a bicycle, combined with the specific location of the diffuse smooth lesions, predominantly along the posterior wall of external iliac arteries, suggests that repeated stretching or bending of the vessels or high flow/shear forces leads to scarring of the vessel wall (Figure 2). Tortuosity and kinking also have been associated with this form of diffuse intimal hyperplasia. Some authors have also proposed that external compression from well-developed hip flexors (including the psoas and iliacus muscles) may be a contributing factor.
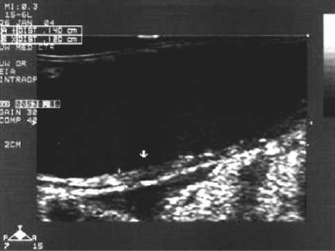
Duplex ultrasound B-mode image showing the diffuse smooth lesion along the posterior wall of the external iliac artery. This wall thickening is suggestive of scarring of the vessel caused by shear forces and high flow.
Methods
Ankle/Brachial Indices
Patients with IE typically have normal resting ankle/brachial indices (ABIs). These are documented at the beginning of the evaluation, after the patient has rested comfortably on a stretcher for at least 5–10 minutes. Systolic pressures are obtained from the bilateral brachial, posterior tibial, and anterior tibial arteries and ABIs are calculated with normal ABI ≥ 0.95.
Duplex Evaluation
Duplex evaluation is essential in the noninvasive diagnosis of IE. Because of the nonfocal and subtle nature of the fibrotic changes, angle correction and velocity estimation must be performed with great care. Careful pre-treadmill duplex scanning often reveals diffusely increased velocities throughout the external iliac artery segments. B-mode visualization of the external iliac artery with suspected IE is difficult, because in many cases this type of lesion is not significantly echogenic. If B-mode resolution is satisfactory, intimal thickening may be viewed on the posterior aspect of the vessel walls or around the circumference of the vessel. In our experience, the increased Doppler flow velocity, waveform contour, and post-stenotic turbulence are the most valuable and reliable pieces of information obtainable.
Angiography
Angiography is still the gold standard for the detection of lower-extremity arterial stenoses and gives an anatomically accurate depiction of these lesions. However, angiography cannot provide the physiologic data that Duplex ultrasound presents. Many of the iliac arteries in the case of IE are not concentric in nature. Therefore, the preferred methods for adequate angiographic evaluation of IE lesions include multiple-projection views. In our experience at this institution, angiography has accurately correlated with duplex findings.
Standard Exercise Treadmill Test
The patient exercises on the treadmill using a modified protocol as specified by the patient, which will bring them to maximal effort, adequately reproduce and document claudication symptoms, and unmask arterial insufficiency. We have demonstrated that although a standard treadmill testing protocol of 2.0 mph with 12% grade for 5 minutes will reveal a mild degree of arterial insufficiency, it will not produce a pronounced postexercise pressure decrease in patients with IE. Because patients with IE are in excellent physical condition, and IE produces a single level obstruction, these patients require an extended duration and intensity of exertion to develop claudication symptoms, and they recover very quickly once they have ceased activity. Ideally, the right and left ankle pressure should be measured simultaneously (which is possible using some pieces of equipment that are currently available). The symptomatic leg is always measured first, because by the time the second limb pressure is obtained, a significant amount of recovery may have occurred (Table 1).
Resting Ankle/Brachial Indices and Postexercise Pressures with Standard Treadmill Protocol
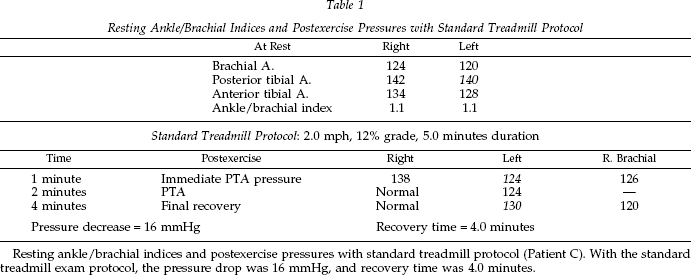
Resting ankle/brachial indices and postexercise pressures with standard treadmill protocol (Patient C). With the standard treadmill exam protocol, the pressure drop was 16 mmHg, and recovery time was 4.0 minutes.
Extended Exercise Treadmill Test
On the basis of these observations, we recommend that the treadmill exam be adapted to these patients’ level of physical conditioning by increasing the speed or elevation and extending the exercise time. The appropriate modification to the treadmill protocol is unique for each patient, at the speed, elevation, and duration necessary to produce patient symptoms. These adjustments allow for correlation with symptoms and produce a larger, more easily detected pressure decrease. Patients with IE should come to the laboratory prepared to walk very fast or run on the treadmill. Advise the patient ahead of time to bring running shoes and gym shorts for the exam. We ask patients to exercise close to their standard training levels and continue until they become symptomatic (Table 2).
Resting Ankle/Brachial Indices and Postexercise Pressures with Extended Treadmill Protocol
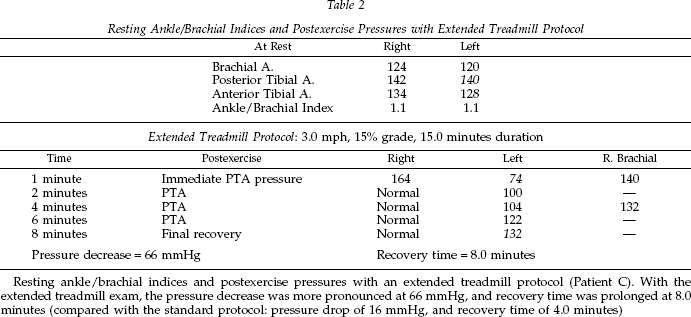
Resting ankle/brachial indices and postexercise pressures with an extended treadmill protocol (Patient C). With the extended treadmill exam, the pressure decrease was more pronounced at 66 mmHg, and recovery time was prolonged at 8.0 minutes (compared with the standard protocol: pressure drop of 16 mmHg, and recovery time of 4.0 minutes)
Postexercise Duplex Evaluation
Analysis of postexercise Duplex evaluation or continuous-wave (CW) Doppler waveforms from the common femoral arteries is helpful to further confirm and localize the level of obstruction. In patients with IE, these postexercise common femoral artery (CFA) waveforms are monophasic with elevated velocity, prominent Doppler bruits, and post stenotic turbulence (Figure 3A and 3B).
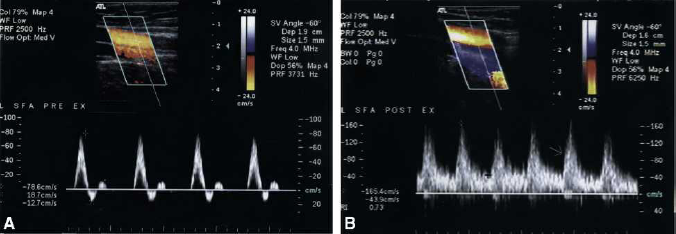
The proximal superficial femoral artery is insonated using duplex ultrasound pre- and post- exercise using the extended treadmill protocol (Patient B). (A) demonstrates a normal, resting Doppler flow signal that has normal waveform contour (triphasic, brisk acceleration, sharp peak, no spectral broadening) and normal flow velocity of 79 cm/sec. (B) is obtained in the same vessel segment post-exercise, where the Doppler flow signal has become abnormal (monophasic, delayed acceleration, post-stenotic turbulence) and elevated flow velocity of 165 cm/sec.
Treatment
Once the diagnosis is made, the goal of treatment is to eliminate the relative stenosis in the external iliac artery segment and restore a widely patent lumen that can transmit the high blood flow rates required during vigorous leg exercise. Although catheter-based intervention with balloon angioplasty and stenting may correct the anatomic defect, this approach is not recommended because of the repetitive bending and compression that occurs at this site. Resection of the stenotic segment and replacement with a prosthetic interposition graft would also address the hemodynamic problem, but the relatively young age of most patients with IE and the repetitive stress of athletic activity make the use of prosthetic graft material undesirable. Because the pathological lesion in IE is fibrotic rather than atherosclerotic, removal of the lesion by endarterectomy is not possible. However, the lesion is typically smooth and diffuse, so leaving the arterial wall intact and enlarging the lumen with a long vein patch angioplasty is very effective, and this has been the approach used in our patients. Inspection of the arterial lumen at the time of surgical repair reveals a smooth, fibrous-appearing lesion with diffuse thickening of the arterial wall (Figure 4A and 4B).

Intraoperative photographs taken during the surgical repair (vein patch angioplasty) of the external iliac artery (Patient C). (A) demonstrates that the smooth intimal lesion is visible on the posterior wall of the vessel. (B) shows the atheroma after endarterectomy.
Optimal treatment requires enlarging the lumen along the entire involved arterial segment, typically from the distal common iliac artery to the proximal common femoral artery. Adequate exposure can be obtained through a lower quadrant, extraperitoneal “renal transplant” type of incision, sometimes supplemented with a vertical groin incision for access to the common femoral artery. The ipsilateral great saphenous vein or one of its large branches serves as patch material (Figure 5). This repair corrects the anatomic lesion using autogenous tissue with minimal disruption of the native arterial wall and excellent long-term durability.

Intraoperative photograph taken during surgical repair (vein patch angioplasty) of the external iliac artery (Patient C). The procedure enlarges the lumen along the entire involved arterial segment, typically from the distal common iliac artery to the proximal common femoral artery. Patch material may be taken from either the great saphenous vein or one of its large branches.
Results
Diffusely elevated velocities were demonstrated, localized to the external iliac artery in all of our patients. The decrease in systolic pressure is demonstrated with the standard exercise treadmill test. However, recovery times are easier to appreciate with an extended protocol, which has been modified from the standard protocol to accommodate the patient's unique level of physical conditioning and cause them to be symptomatic.
Postexercise Doppler waveforms are abnormal in all patients and verify the level of disease. Doppler arterial waveforms and systolic pressure measurements confirm that physiologic testing is a paramount diagnostic tool for this patient population (Table 3A–3E).
Patient Demographics and History
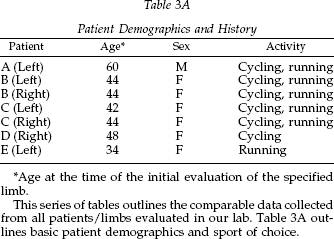
Age at the time of the initial evaluation of the specified limb.
This series of tables outlines the comparable data collected from all patients/limbs evaluated in our lab. Table 3A outlines basic patient demographics and sport of choice.
Patient Resting Diagnostic Information
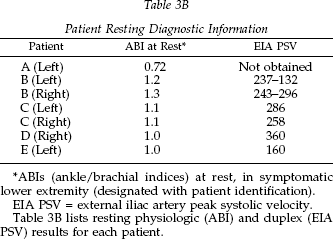
ABIs (ankle/brachial indices) at rest, in symptomatic lower extremity (designated with patient identification).
EIA PSV = external iliac artery peak systolic velocity.
Table 3B lists resting physiologic (ABI) and duplex (EIA PSV) results for each patient.
Patient Exercise Treadmill Information
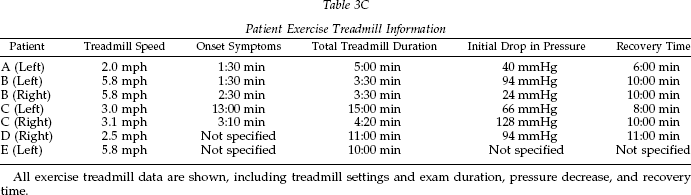
All exercise treadmill data are shown, including treadmill settings and exam duration, pressure decrease, and recovery time.
Patient Diagnostic Information
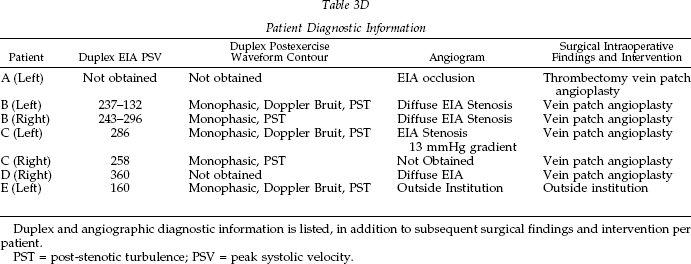
Duplex and angiographic diagnostic information is listed, in addition to subsequent surgical findings and intervention per patient.
PST = post-stenotic turbulence; PSV = peak systolic velocity.
Patient Follow-up Information
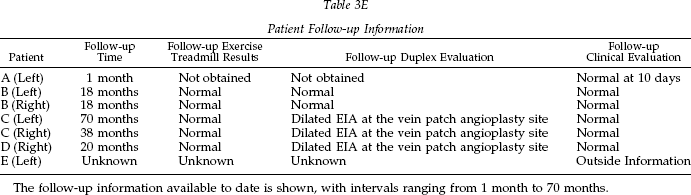
The follow-up information available to date is shown, with intervals ranging from 1 month to 70 months.
Long-term Follow-up
Five limbs have been evaluated with Duplex ultrasound post-operatively. Long-term follow-up ranges from 18 to 70 months. The 5 limbs with follow-up exercise treadmill exams all had normal postexercise pressures and did not develop claudication symptoms. All were able to resume their training regimens at normal levels. All subsequent duplex evaluations have shown dilated external iliac arteries, and no evidence of pseudoaneurysm or stenosis (Figure 6).
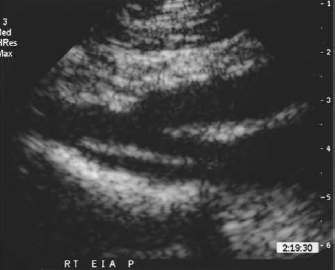
Postoperative follow-up duplex ultrasound image of a dilated external iliac artery. All external iliac arteries evaluated thus far appear dilated, with no evidence of pseudoaneurysm or stenosis.
Discussion
The pathologic mechanism of IE is not fully understood. As previously discussed, the common history of patients who exercise vigorously either cycling or running and the unique location of these lesions in the iliac arteries suggests that repeated stretching or bending of the vessels or high flow/shear forces leads to scarring of the vessel wall. Some authors have also proposed that external compression from well-developed hip flexors (including the psoas and iliacus muscles) may be a contributing factor. 1
Physiologic testing and noninvasive Duplex evaluation of IE is a unique and specialized application of vascular testing. Although angiography remains the gold standard in diagnosis of arterial stenoses, detection of IE lesions is not as straightforward as the identification of atherosclerotic lesions. Many recent case reports are in agreement that duplex ultrasonography, together with physiologic arterial testing, may provide greater sensitivity to IE than angiography alone. 2 Physiologic testing is an essential step and emphasizes that imaging alone is not always adequate.
Because the diagnosis of IE by noninvasive means is difficult, its true prevalence is unknown. The resting clinical examination is generally completely normal. A soft bruit may be auscultated in the inguinal region of the symptomatic leg, which becomes more pronounced after exercise. Palpable pedal pulses are usually obtained, with normal resting ABIs. These findings suggest that the lesions are not hemodynamically significant under resting conditions. 3 However, the possibility of true claudication and arterial occlusive disease should not be prematurely ruled out, and the possibility of false negative diagnoses should lead the technologist to a thorough noninvasive evaluation for these athletes who are in excellent physical condition. 4 We are able to document these arterial lesions indirectly by increasing the patient's limb blood flow with extended exercise and observing a decrease in ankle systolic pressures after exercise. Duplex evaluation is then used to directly evaluate the lesions.
Doppler flow velocities and waveform characteristics are far superior to B-mode imaging in documenting IE lesions. B-mode imaging can demonstrate softly echogenic intimal thickening and vessel tortuosity. Many sources, in correlation with our own findings, describe a segmental narrowing or thickening.3,5,6 Abraham et al. 7 compared the B-mode appearance of the intimal thickening to that of other investigations (i.e., arteriography, histological evaluations, etc.) and found that B-mode imaging alone had a sensitivity of 0.78 and a specificity of 0.80 in the diagnosis of IE. Technologist experience and advances in ultrasound technology have undoubtedly contributed to the increase in sensitivity and specificity in the time since their findings were published. Because of the tortuosity of the iliac arteries in many documented cases and the eccentric rather than concentric nature of many of the lesions, multiple-projection angiography views are mandatory to adequately evaluate the vessel.3–6,8 Long-term follow-up reveals that the external iliac arteries dilate over the postoperative course.
For many people, physical exercise is a tremendous outlet for stress and the key to their healthy lifestyle. To be told that one must give up the activity they've dedicated their life to can be devastating to one's livelihood and sense of self. Accurate diagnosis of IE can change the lives of these patients, and the rewards for the patient, as well as the vascular technologist, and interventionalists are priceless.