
Abstract
The vascular laboratory was called to the neonatal intensive care unit to perform a carotid duplex examination on a 2-day-old infant. This term female newborn was delivered via caesarian because of labor that failed to progress. There were no significant maternal risk factors. On day 2, the infant was noted to have seizures. Magnetic resonance imaging of the brain demonstrated a large left hemispheric infarct with a midline shift. The findings of an echocardiogram were normal. The carotid system was evaluated by the use of a “hockey stick” 15–7 MHz linear array transducer. The common, external, and internal carotid arteries were well visualized bilaterally, as well as the vertebral and subclavian arteries. The right side was normal. The left common carotid artery signal was high resistance and a drumbeat, high resistance signal was noted at the origin of the internal carotid artery. The internal carotid artery appeared to be filled with soft echoes, and no signal was detected within the internal carotid artery beyond the origin. The infant was then transferred to Children's hospital for further evaluation and possible tissue plasminogen activator treatment.
Neonatal cerebral infarction has been reported to be present in 1 in 4,000 full-term infants. Neonatal cerebral infarct was found in 12% of infants who developed neonatal seizures. Newborns with arterial ischemic stroke usually present with seizures. Primary risk factors for arterial ischemic stroke include cardiac disease, perinatal complications, and other acute illnesses, including dehydration and prothrombotic disorders. Mortality rates after arterial ischemic stroke in newborns are less than 10%. In many cases, the outcome is normal. Duplex imaging of the carotid vessels is feasible in neonates and can provide the treating physician with valuable diagnostic information.
Introduction
Carotid duplex examinations are routinely ordered for adult patients with cerebrovascular symptoms and have been extensively reported in the literature. Evaluation of the extracranial carotid arteries in infants and newborns routinely is not performed and few studies have been published on the efficacy of cerebrovascular ultrasound in this group of patients.
Case Report
The neonatal intensive care unit requested a carotid duplex exam on a 2-day-old newborn because magnetic resonance imaging (MRI) revealed a large left hemispheric infarct. The female, full-term newborn was delivered by caesarian delivery because of labor that failed to progress. There were no significant maternal risk factors. On day two of life, the infant was noted to have seizures, at which point an MRI was performed, which showed a large left hemispheric infarct involving the entire middle cerebral artery (and anterior cerebral artery (ACA) territories with an associated mass effect, midline shift, and herniation (Figure 1). The differential diagnosis suggested by radiology included hypercoagulability, embolic infarct or a possible dissection of the internal carotid artery (ICA).
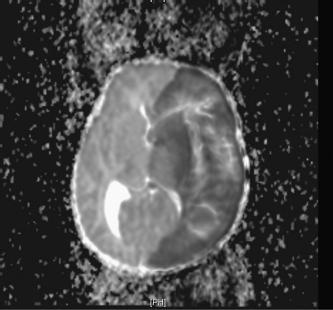
MRI of the brain shows a large left hemispheric infarct with midline shift and herniation.
We performed a carotid duplex examination by using a 15–7 MHz “hockey stick” linear array transducer. Because of the seizures, the infant was sedated, which facilitated the examination. The common, external, internal, vertebral, and subclavian arteries were well visualized bilaterally. The right side was normal (Figures 2 and 3). The left common carotid signal had low end diastolic velocities (Figure 4). The external was patent. The proximal ICA signal had a drumbeat, high-resistance signal with very low velocities (Figure 5). The ICA appeared to be filled with soft echoes, and no Doppler signal or color filling was detected in the ICA beyond the origin of the artery (Figures 6 and 7). After the carotid examination, the infant was transferred to Children's Hospital for further evaluation.
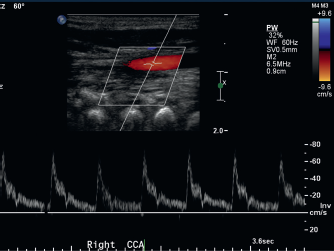
Doppler signals and color flow of the right common carotid artery demonstrates normal color filling and normal spectral waveforms.
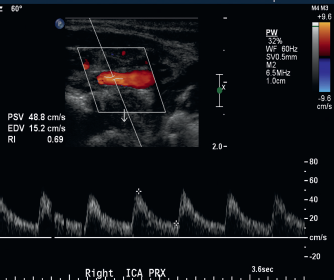
Doppler signal and color flow of the right internal carotid artery demonstrates normal color filling and normal spectral waveforms.
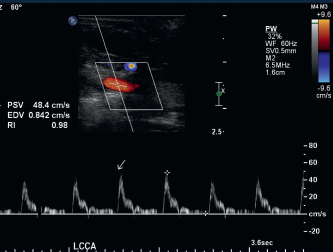
Doppler waveforms and color flow of the left common carotid artery demonstrates normal color filling but low diastolic velocities in the spectral waveforms.
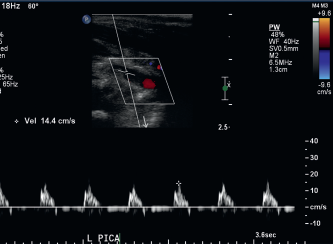
High-resistance waveforms present in the proximal left internal carotid artery.
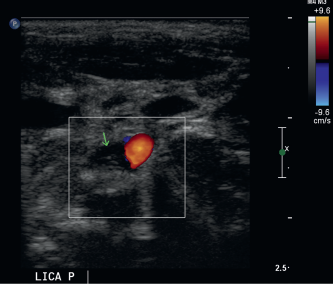
Absence of color flow in this transverse image of the carotid bifurcation. Low-density echoes appear to fill the lumen of the internal carotid artery (arrow).
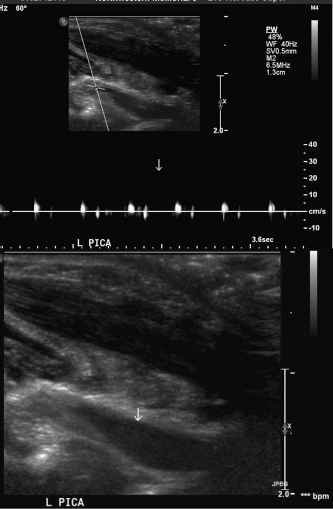
(A) Drumbeat, high-resistance signal in the proximal-mid left internal carotid artery. (B) Soft echoes filling the lumen of the proximal-mid left internal carotid artery in long axis.
A hypercoagulability workup was negative. She was placed on enoxaparin and phenobarbital. She experienced no further seizures. At 17 months of age, she is off enoxaparin, aspirin (ASA), and phenobarbital. She is receiving physical therapy for right hemiplegia and right visual neglect. Follow-up duplex examination demonstrates a patent left ICA.
Discussion
The prevalence of neonatal cerebral infarction is estimated to be 1 in 4,000 and is found in 12% of infants presenting with neonatal seizures.1,2 Newborns with arterial ischemic stroke usually present with seizures or lethargy in the first few days of life. 2 Systemic risk factors for arterial ischemic stroke include cardiac disease, perinatal complications, and other acute illnesses, including dehydration and prothrombotic disorders. 2
The mortality rate after an arterial ischemic stroke is less than 10%. 2 Neurologic deficits are detected in survivors by several years of age. 2 These can include motor disability, continued seizure disorders, recurrent systemic or cerebral thrombosis, and the possibility of learning disorders. In the study by Estan and Hope, 1 one infant developed hemiparesis, and the other 11 had normal motor development when examined at a mean of 33 months. None of the 12 infants had overt cognitive deficits or a persistent seizure disorder.
Treatment of arterial ischemic stroke is controversial. Thrombolytic treatment is rarely used because of the risk of bleeding. When the etiology of the ischemic stroke is clearly embolic, anticoagulation therapy should be considered. 2
Conclusions
Carotid duplex imaging was successfully completed in this newborn, providing the physician with valuable diagnostic information to assist in determining treatment options.