
Abstract
Varicose veins are common in the adult population, occurring in approximately one third of men and women. Several endovenous treatment options are now available, including radiofrequency, laser thermal, and foam ablation. These minimally invasive procedures rely on the use of ultrasound for safe and efficacious treatment. Ultrasound has become standard for diagnosis of venous pathology, and its increasing use has lead to a more thorough description of the variability in lower-extremity venous anatomy. The presented patient case exemplified variations in venous anatomy that may be encountered during endovenous ablative procedures and how these variables can be managed under ultrasound guidance. The patient was a 58-year-old woman who was experiencing leg pain from her calf varicose veins despite conservative therapy. Her superficial reflux was greater than 0.5 seconds, and radiofrequency ablation was recommended. At time of the procedure a large, incompetent anterior accessory saphenous vein (AASV) with a corresponding segment of hypoplastic great saphenous vein (GSV) at the proximal thigh was noted. Her AASV was transmitting venous reflux to the lower, more medial, true GSV through a large collateral. With the use of ultrasound, the GSV was accessed distally at the upper calf and a guidewire passed through the collateral vein to the AASV. This allowed the radiofrequency catheter to pass from the lower GSV to the saphenofemoral junction and treat both segments of incompetent vein from a single access site. To the authors' knowledge, this selective cannulation of the AASV from the true GSV during radiofrequency ablation has not been previously reported in the literature. Alternative treatment would have required separate sheath access of each vein, leading to greater patient discomfort, extended procedure time, and a less-effective therapy. This case highlights the integral role of skilled ultrasonography during radiofrequency venous ablation in a certified laboratory, especially when dealing with variations in venous anatomy of the lower extremity.
Introduction
Venous insufficiency resulting in varicose veins is common in the adult population, occurring in approximately one third of men and women. 1 Severity of resulting morbidity may lie on a wide spectrum, from esthetic dissatisfaction, to continuous pain and pruritus, to loss of skin integrity from ulceration. The impact venous insufficiency can have on a patient's daily function is reflected in the Venous Clinical Severity Score and quality of life measurements recording detriment equal to that of other chronic diseases such as arthritis.2,3 Historically, the accepted treatment has been surgical intervention, with high ligation of the great saphenous vein (GSV) at the saphenofemoral junction (SFJ) combined with vein stripping with or without concurrent isolated phlebectomy. Although complications from surgery generally are minor, postoperative pain and bruising can be significant enough to delay a return to normal activities. There are currently several less-invasive modalities available for the treatment of venous insufficiency. These include endovenous radiofrequency thermal ablation (RFA), endovenous laser thermal ablation (EVLA), liquid sclerotherapy, foam sclerotherapy, or a combined approach. Major advantages of these less-invasive procedures include the ability to perform them in a clinical setting using only local anesthesia. During the last decade, there has been a significant increase in the use and investigation of these endovenous treatments. Recent randomized controlled trials and meta-analyses have found that these less-invasive therapy options are as effective as surgery, with less procedural morbidity and an earlier return to normal activities.4–7
Case Report
A 58-year-old woman was referred to our vascular clinic for evaluation of her bilateral lower-extremity varicose veins. Symptoms at that time included bilateral leg pain that was worse on the left, muscle cramping at night, and swelling of the left ankle. Swelling and pain were increased with standing and relieved by elevation of legs. She had suffered from thrombophlebitis of the left paratibial GSV 4 months previously, which had resolved at time of presentation. She had no history of trauma to either legs or any deep vein thromboses in the past. She was gravid 2 para 2 and had no previously attempts of conservative treatment for varicose veins. She did not exercise regularly and was an everyday smoker. The remainder of her medical and surgical history was not contributory.
On examination, the patient had brownish discoloration at both gaiter areas, with edema at the left ankle. Bilateral varicose veins were present, tender to palpation, and without a palpable cord. Bilateral posterior tibialis and dorsalis pedis pulses were normal. Patient had no skin ulceration or bleeding. The patient underwent bilateral lower extremity duplex ultrasound that revealed no deep venous pathology. The true GSV in the upper thigh was small. The anterior accessory saphenous vein (AASV) was dilated up to 12 mm in diameter with greater than 0.5 seconds of reflux (Figure 1). This reflux collateralized to the true GSV at the lower thigh. CEAP designation was C4 EP AS PR.
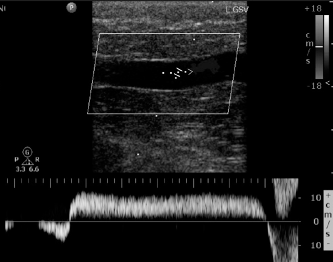
Duplex ultrasound of the patient's left GSV at initial consultation showing more-than 5 seconds of reflux after calf compression.
Increased daily exercise, smoking cessation, elevation of foot of bed at night, and daily use of 30–40 mmHg compression stockings were recommended. Patient returned to clinic 6 months later with persistent bilateral leg pain despite compliance with conservative therapies. At that point, RFA of her left GSV was recommended.
Methods
Procedure
The RFA procedure was performed in a surgical suite under guidance of a Philips HD11 ultrasound system and a Philips L9-3 linear vascular probe (Philips Healthcare, Bothell, WA). Patient's left incompetent superficial anatomy was mapped by ultrasound, along with other varicose tributary veins, and suitable access sites. At that time the AASV was noted. Its course was traced from the SFJ to its connection with the GSV through a large collateral vein at the mid-thigh. A corresponding segment of hypoplastic GSV without reflux in the proximal thigh also was noted (Figure 2). With the patient in supine position, her leg was prepared and draped. A 7-F radiofrequency catheter (ClosureFast Catheter, VNUS Medical Technologies Inc, San Jose, CA) with a 7-cm heating element was placed on the sterile field, flushed, and wiped down. Local anesthesia was instilled in the skin overlying the access site just below the knee. The true GSV was punctured at the upper calf, and a guidewire was introduced through the needle, which was then exchanged over the guide wire for a 7-F sheath.
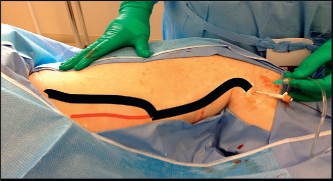
Patient's left leg prepared for RFA. Black line indicate the major reflux channel, including the GSV distally and the anterior accessory saphenous vein proximal connected by a large collateral vein. Red line indicates the segment of hypoplastic great saphenous in proximal thigh.
A Berenstein II catheter was inserted through the sheath and advanced to the level of the mid-thigh. A Merit 0.018 angled tip hydrophilic guide wire was then placed through the large collateral from the GSV into the AASV. This allowed passage of the radiofrequency catheter from the GSV at the level of the mid-thigh trough the collateral vein, into the AASV, and up to a point 2.8 cm distal to the SFJ.
After the radiofrequency catheter tip position was reverified by ultrasound, and tumescent anesthesia was infiltrated precisely into the perivenous compartment along the entire length of vein from the insertion site to SFJ, until a “halo” of fluid was noted around the vein. Using a Covidien RFG2 radiofrequency generator, we increased the radiofrequency catheter to temperatures of 110 ± 5°C in 20-sec treatment intervals. The radiofrequency catheter was withdrawn in 6.5-cm segments. The first and second segments were treated with two cycles each and the third, fourth, fifth, and sixth segments with one cycle each. Total treatment time was 160 seconds, eight cycles, treating a total venous length of 42 cm. The radiofrequency catheter and sheath were removed, and after assuring hemostasis, the skin incision was closed with a bandage.
Immediately after the procedure a repeat duplex ultrasound of the treated veins was performed for identification of vein occlusion, compressibility, and wall thickness. A graduated compression stocking was applied from the level of the foot to the most proximal level of the thigh. Continued ambulation was stressed and per protocol patient wore a thigh high graded compression stocking 24 hours a day for one week after the procedure.
Literature Search
A search of MEDLINE for all English language articles from 1996 through September 2013 with MeSH terms catheter ablation, ultrasonography, and veins was performed. The search returned 16 articles, which were reviewed. None of the articles addressed selective cannulization of the AASV during RFA, supporting the belief that this approach has not been reported previously in the literature.
Results
Immediate postprocedure ultrasound confirmed successful treatment with complete loss of flow through the AASV and GSV, along with increased echogenicity and decreased compressibility of the venous wall. Repeat duplex ultrasound of patient's left lower extremity at 1-week (Figure 3) follow-up showed no deep venous pathology and no flow through either the AASV or GSV. At 8 weeks' follow-up, the patient's pain had resolved, and her leg was relieved of varicosities (Figure 4).
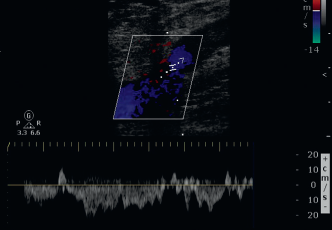
Duplex ultrasound of patient's SFJ 1 week postprocedure. Color duplex confirming cessation of flow through the anterior accessory saphenous vein.

Patient's left leg 2 months postprocedure.
Discussion
Our RFA procedure was successful as all main refluxing braches were identified and treated. The aforementioned case underscores the required familiarity with common anatomical variation of the lower-extremity venous anatomy and the use of ultrasonography for anatomic identification of this anatomy.
Lower-Extremity Venous Anatomy
Knowledge of the venous anatomy in the lower extremity is required for both the diagnosis and treatment of venous diseases. When discussing lower-extremity venous anatomy the deep and superficial systems are separated. The deep venous system comprises the deep plantar venous arch, posterior tibial, anterior tibial, peroneal, popliteal, and femoral veins. The superficial system references the dorsal venous arch, small saphenous, great saphenous, and the numerous collateral and accessory veins that drain to the saphenous vein. These two systems, deep and superficial, are connected to each other through perforator veins. In contrast to the relatively constant arterial anatomy of the lower extremity, venous anatomy is highly variable, especially in the superficial system. This has been further complicated in the past by an inconsistent nomenclature that has only recently been standardized.8,9 Because the majority of symptomatic varicose veins stem from incompetence in the superficial system, we focus on the variations of anatomy in the superficial system.
The GSV originates from the dorsal venous arch of the foot and runs anterior to the medial malleolus. It ascends along the medial side of the leg and joins with the common femoral vein at the level of the groin skin crease. Several common variations of the GSV at the thigh have been reported. The GSV can be with, or without, large subcutaneous tributaries. These tributaries may be at times larger than the saphenous but are never found in the saphenous compartment. Alternatively, these subcutaneous tributaries may enter the saphenous compartment to become the GSV. Patients may demonstrate a GSV and an AASV within their respective fascial compartments, but true duplication of the GSV only occurs 1% of the time. 10 Again, variation is seen as the GSV approaches the knee. In approximately 25% of limbs, a solitary GSV will cross the knee. Fifty percent of patients will have a large tributary vein cross the knee to join with the GSV somewhere in the thigh. In 30% of legs this large tributary is bypassing an absent or hypoplastic GSV at the knee. 11
The SFJ also receives flow from the superficial circumflex iliac, superficial epigastric, and superficial external pudendal veins. These tributaries drain directly to the GSV 80% of the time, but they may also join the femoral vein directly or as a common trunk with another saphenous tributary. In only 20% of the patients will all three of these veins join the GSV as separate tributaries. 12 The AASV and posterior accessory veins are larger veins that also drain to the SFJ. The AASV, present in 41% of people, courses the lateral thigh, and joins the GSV. In addition to the draining pattern, the AAVS displays variable diameter, course, and distance. The AASV is contained within its own fascial compartment and may become incompetent, forming a source of reflux. 13
The small saphenous vein (SSV) courses behind the lateral malleolus and ascends along the midposterior calf, penetrating the deep fascia of the calf to join the popliteal vein at the saphenopopliteal junction (SPJ). The SPJ itself has a variable location, often 2–4 cm above the knee crease, or higher in 25% of the population. There are occasional true duplications of the SSV, with multiple small veins running in the saphenous compartment. The SSV joins the popliteal vein most commonly from a lateral or posteromedial approach. It may also join the popliteal via a smaller “anastomotic” vein, and in some legs will not join the SPJ at all. Regardless of its union with the popliteal vein, the SSV will give off a thigh extension (TE) in 95% of limbs. The TE courses cranially along the posterior thigh, deep to the fascia. The TE may divide into superficial branches in the posterior thigh, join the deep femoral vein, or connect with the GSV. 13 If the TE communicates with the GSV, it is then termed the vein of Giacomini. The TE and Giacomini vein are capable of both transmitting reflux from proximal veins to the SSV and generating reflux in an ascending fashion to varicosities of the posterior thigh.
Ultrasound Markers of Venous Anatomy
Common ultrasound makers of venous anatomy include the saphenous eye, the alignment sign, and the tibiogastrocnemious angle sign. 13 The saphenous eye describes the characteristic appearance of the saphenous compartment by ultrasound; the echogenicity of the superficial and deep aponeurotic fascia form the eyelids and the translucent lumen of the GSV represents the iris (Figure 5). This compartment is always present, and the GSV is always found within its boundaries. The AASV also is contained within a fascial compartment separate from that of the GSV. The alignment sign is used to distinguish between these two veins. The AASV lies anterior and lateral to the GSV, and the lumen of the AASV can be seen with ultrasound to align directly over the femoral artery and vein. The alignment sign may be necessary for proper identification of anatomy at the SFJ in cases where the GSV is absent and only an AASV is present. Proper designation of the GSV in a fascial compartment can be more difficult toward the knee, as the fascial layers come closer. The tibiogastrocnemious sign is a triangle formed from the tibia, medial gastrocnemius muscle, and fascial sheet. An empty tibiogastrocnemious triangle is indicative of a hypoplastic or absent GSV.
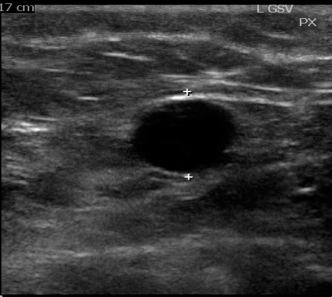
Ultrasound of “saphenous eye.”
Ultrasound in the Diagnosis of Venous Pathology
Duplex ultrasonography may be the most used modality in the diagnosis of lower-extremity venous disease. Ultrasound is fast, noninvasive, without radiation exposure, and yields both anatomic and hemodynamic information. The use of ultrasound in the diagnosis of venous insufficiency is reflected in the standardized CEAP (i.e., Clinical, Etiologic, Anatomic, and Pathophysiologic) classification system. 14 Specifics of ultrasound use for the diagnosis of venous disease can be found in the recently published clinical practice guidelines from the Society for Vascular Surgery and the American Venous Forum, 15 which includes suggestions for probe frequency, patient positioning, descriptions of the anatomy to be detailed, and necessary reporting information. Again, even with protocol standardization, use of certified and experienced ultrasound technologist for accurate diagnosis would be recommended.
Ultrasound during Endovenous Ablative Procedures
Along with the use of duplex ultrasonography in the diagnosis of lower-extremity venous insufficiency, real-time ultrasound imaging is required for safe and effective endovenous treatment. Ultrasound is used for preprocedural vein mapping, guidance of venous access, catheter advancement, and confirmation of catheter tip placement at the SFJ. Precise location of heating catheter tip near SFJ must be observed as risk for thrombosis in the deep venous system is increased if the catheter tip is within 1 cm of the SFJ. Placement of tumescent anesthesia into the perivenous space is also facilitated by ultrasound guidance. Needle penetration of the superficial fascia is observed and deposition of the tumescent into the saphenous compartment confirmed. We aimed to create a “halo” of anesthetic indicating complete coverage, compression, and increased surface depth of the vein. The ultrasound probe often is used to apply pressure at the segment of vein undergoing treatment. Immediately after the procedure, and during subsequent follow-up, ultrasound is used to measure success of treatment and monitor for recurrence. The presence of venous flow, compressibility, and echogenicity of the vein wall, along with luminal reduction are all noted. For safety, screening for induced thrombus in the deep venous system is also done at this time.
Because of the integral role of ultrasound throughout the procedure, it is important the procedure be performed in certified ultrasound laboratories with experienced ultrasound technologist.
Use of RFA for the Treatment of Venous Reflux
Surgical ligation and stripping of the GSV has shown to have a 3-year success rate of 78%. Foam sclerotherapy, RFA, and EVLA have 3-year success rates of 77%, 84%, and 94% respectively. 5 Not only is endovenous treatment as effective as surgery, return to normal activities is significantly shorter; 4 days with stripping, compared with 2 days with EVLA and 1 day with RFA. 4 In the presented case it was decided to use RFA over EVLA because of the high procedure success rate coupled with increased patient tolerance. Although RFA and EVLA both have better postprocedure morbidity compared with surgery, RFA has been shown superior to EVLA in earlier return to work and activities, lower postprocedure pain, and less bruising. 16 New endovenous technologies and long-term outcomes of these procedures continue to be studied, but the procedural role of ultrasound is well established.
Case Relevance
The variability in lower-extremity venous anatomy has the potential to impact the success of endovenous ablative procedures. Even with the successful ablation of the GSV, the capacity for adjacent veins to transmit reflux is a potential source for continued varicosities. Continued reflux of an AASV after RFA treatment of the GSV was specifically described by Proebstle et al. 17 Leaving the presented patient's AASV untreated could allow reflux from the SFJ to continue with persistence of varicosities in the lateral proximal thigh. Alternatively, the AASV could have been treated separately from the GSV. This would have resulted in another venous puncture, increasing the patient's risk for discomfort and adding to the overall procedural time and cost. Additionally, the separate ablative treatment of the AASV and the GVS would have left the large collateral vein at the mid-thigh open and a potential source for continued varicosity. Only with the ability to visualize the patient's anatomy in real-time was it possible to cannulate the AASV from the GSV and successfully treat all segments of incompetent vasculature. Not only does this case illustrate a novel treatment approach during RFA, it demonstrates the need for proper identification of the venous anatomy. With high anatomic variability, an intimate knowledge of the common variations that may be encountered is paramount to the proper identification of a patient's dominant refluxing channel. Without proper localization of major refluxing branches and their anatomic relation to each other, any endovenous treatment may be at high risk for failure.