
Abstract
Branched endoprostheses for endovascular repair of pararenal and thoracoabdominal aortic aneurysms are undergoing evaluation in prospective clinical trials. Duplex ultrasound has been a cornerstone of surveillance for vascular reconstructions. This paper describes the development and deployment of a standardized duplex imaging protocol to evaluate individuals who have undergone endovascular repair of their thoracoabdominal aortic aneurysm. Ultrasound imaging is performed after an 8 to 12 hour fast to minimize the presence of bowel gas and allow for optimal imaging of abdominal vascular structures. Doppler measurements of peak systolic and end diastolic velocity are made at specific arterial segments in the aorta and the celiac, superior mesenteric, and renal arteries. Resistive indices are also recorded in the segmental and arcuate arteries of both kidneys. Pulsed-wave Doppler is used to record spectral Doppler data and color Doppler is used to image all arterial segments and ensure proper placement of the Doppler sample volume and ensure correct angle of interrogation. Implementation of a standardized duplex ultrasound imaging protocol can be used to image and follow individuals who have received the Thoracoabdominal Branch Endoprosthesis (TAMBE) device and branched endovascular aneurysm repair (BEVAR). Ultrasound may provide complementary findings and may add information to the computed tomography angiography imaging for following these individuals.
Introduction
Aortic aneurysm is a degenerative disease, resulting in a weakening of the wall and dilation of the aorta. 1 Once the aortic diameter is ≥50% more than its original diameter, it is referred to as an aneurysm. 1 A thoracoabdominal aortic aneurysm (TAAA) is an aneurysm which extends from the thoracic aorta distally to the abdominal aorta.1,2 TAAAs are complex lesions to treat as the extension into the abdomen may involve the visceral branches to include the celiac, superior mesenteric, and renal arteries. 1 The most serious complication from a TAAA is rupture.1,3,4 Other clinical manifestations of TAAA include congestive heart failure (associated with aortic regurgitation), compression of the trachea and/or bronchi, and compression of the esophagus. 4
Fenestrated and branched endovascular aneurysm repair (FB-EVAR) is increasingly being used to treat TAAAs.2,5–7 The GORE® EXCLUDER® Thoracoabdominal Branch Endoprosthesis (TAMBE; W.L. Gore & Associates, Flagstaff, Arizona) is an aortic endoprosthesis system designed to treat pararenal and thoracoabdominal aortic aneurysms (PRAA, TAAA) and is currently under investigation in an ongoing food and drug administration (FDA) investigational device exemption (IDE) trial. The TAMBE device is a modular multicomponent system (multi-branch stent graft, bifurcated distal component and iliac limb extensions) with 4 portals to allow branched endovascular aneurysm repair (BEVAR) treatment for complex PRAA and TAAA that involve the mesenteric and/or renal arteries (Figure 1).
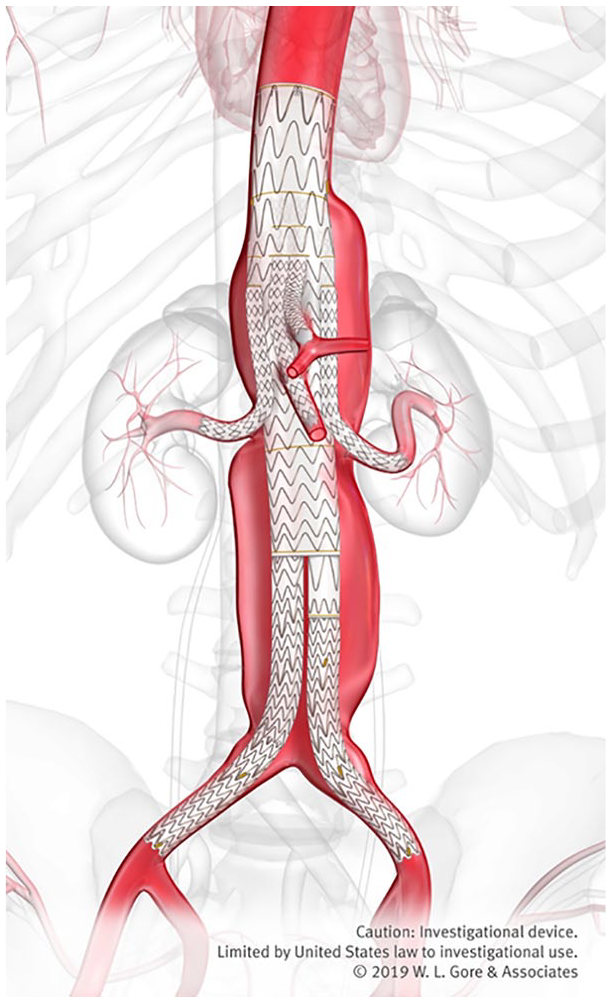
Thoracoabdominal Branch Endoprosthesis device demonstrating 4 portals: celiac artery, superior mesenteric artery, left renal artery, and right renal artery.
While BEVAR provides a less invasive treatment option for individuals with TAAA,2,5 once placed, lifelong surveillance is required to ensure stent patency 5 and ensure successful protection against rupture. Thus, imaging modalities that are widely available and are low risk to patients are desirable. The current gold-standard imaging for stent patency is computed tomography angiography (CTA), which allows for evaluation of aortic diameter, identification and classification of endoleaks, and detection of stent deformations.8,9 However, this imaging modality has higher cost and is not without risk, such as exposure to ionizing radiation and adverse reaction to iodinated contrast. 5 Duplex ultrasound (DUS) has been used for surveillance of abdominal aortic aneurysms and to provide surveillance of stent-grafts.5,6 DUS is widely available with favorable cost and safety (no exposure to ionizing radiation, nor use of iodinated contrast), thus making it an ideal modality as a tool for monitoring individuals post BEVAR treatment. However, limitations of DUS imaging do exist and include the technical skill of the sonographer (operator), and imaging limitations due to obesity and bowel gas which may impede visualization of arterial segments.5,8
While CTA imaging is important in the surveillance of these devices, CTA imaging does not provide hemodynamic information and has limitations in the evaluation of visceral stents given the size and metallic artifact. DUS imaging can provide important hemodynamic information regarding stent patency and changes in hemodynamics over time. For example, DUS can be used to examine quantitative hemodynamic information (i.e., velocity and resistive index [RI] data) and also monitor changes in these data over time. Qualitative changes in the Doppler waveform associated with proximal stenosis (such as a tardus parvus waveform) can also be examined to provide indirect information regarding stent patency. The protocol described in this document is intended to help define a process to identify branch stent issues prior to occlusion.
As stated previously, DUS has been used to monitor the patency and function of stents in the celiac, superior mesenteric, and renal arteries.5,10–19 Studies have reported velocity thresholds for stented vessels and described technical standards regarding use of a Doppler angle of 60 degrees or less to detect elevated peak systolic velocities (PSV) and decreased end diastolic velocities (EDV). However, there is little data available for applying velocity criteria to fenestrated and branched stent-grafts, and thus prospective longitudinal studies evaluating DUS velocity values and changes in velocity over time are needed to allow for the development of criteria that would indicate when the stent-graft is patent and function is normal or when intervention may be needed. Suggested protocols for imaging native visceral vessels and stented vessels have been reported.5,20–23 Components from published protocols were incorporated into the creation of the TAMBE pre- and postprocedure DUS imaging protocol.5,7,10,14,15,17–22 The purpose of this study is to describe the DUS protocol for imaging pre- and postplacement of the TAMBE device and show an example of how DUS is able to detect branch vessels at risk for thrombosis in patients with branched and fenestrated endovascular aneurysm repair.
Duplex Ultrasound Protocol
Patient Preparation
The patients should be fasting for at least 8 hours prior to the DUS examination. This helps to eliminate bowel gas and therefore will enhance the technical success and quality of ultrasound images and ability to identify arterial segments required for a complete examination.
Patient Position
The patient is placed in the supine position for the start of the examination for imaging of the proximal aorta and the celiac and superior mesenteric arterial segments. The patient may be positioned in oblique or lateral decubitus or prone positions for imaging the renal arteries.
Ultrasound Equipment
An ultrasound system with B-mode, color Doppler, and spectral pulsed-wave Doppler is required. In addition, dedicated abdominal ultrasound imaging transducers (sector, vector, curvilinear) with appropriate frequency bandwidth should be used (2.5-10.0 MHz). It is recommended that laboratories performing these procedures utilize system presets that are dedicated for the abdominal Doppler examination. This may require consultation with ultrasound clinical applications specialists to optimize presets for this examination.
Imaging Protocol
The DUS examination is performed prior to treatment to determine baseline velocities in the proximal aorta, celiac artery (origin, proximal, and distal arterial segments), superior mesenteric artery (SMA) (origin, proximal, mid, and distal arterial segments), aorta at the level of the renal arteries, left and right renal arteries (origin, proximal, mid, distal and hilar arterial segments). The intra-renal vessels (segmental and arcuate arteries) are also examined in the upper pole, mid kidney, and lower pole. If the celiac artery cannot be evaluated, the hepatic artery and splenic artery are evaluated at liver hilum (hepatic artery) and splenic hilum (splenic artery). In addition to imaging and recording the PSV and EDV, RIs are also calculated for the segmental and arcuate arteries (Table 1).
Thoracoabdominal Branch Endoprosthesis Imaging Protocol Preprocedure.


Postprocedure, imaging is performed at hospital discharge, 1 month, 3 months, 6 months, 12 months, and annually thereafter for 5 years (Table 2).2,20–22 The postprocedure protocol entails imaging and recording of the PSV and EDV in the following arterial segments: proximal aorta, celiac artery (the stent is imaged at the origin of the native artery and then a color Doppler and pulsed-wave Doppler spectral waveform is captured at the proximal stent, distal stent, and distal native artery), and superior mesenteric artery (the stent is imaged at the origin of the native artery and then a color Doppler and pulsed-wave Doppler spectral waveform is captured at the proximal stent, mid stent, distal stent, mid native artery and distal native artery). If the celiac artery cannot be evaluated, the hepatic and splenic arteries are evaluated at the liver hilum and splenic hilum. The right and left renal arteries are also imaged from their native vessel origin to the renal hilum. Images with color Doppler and a pulsed-wave spectral Doppler waveform are captured at the native vessel origin, proximal stent, mid stent, distal stent, and distal native renal arterial segments (See Figures in Table 1 and Table 2). The intra-renal vessels, arcuate and segmental vessels are imaged with color Doppler and a spectral waveform is acquired from the upper, mid kidney, and lower poles. For each spectral Doppler waveform the PSV and EDV are obtained and the RI calculated. All information is entered into a sonographer worksheet. Different worksheets exist for both pre- and postprocedure (see Appendix A and B in the online article).
Thoracoabdominal Branch Endoprosthesis Imaging Protocol Postprocedure.


Technical Considerations
B-mode images to demonstrate anatomical structures should be acquired at a 90 degree angle (perpendicular) to the transducer face to demonstrate the best tissue interfaces. All spectral Doppler waveforms are to be acquired at an angle of 60 degrees or less to ensure accurate velocity estimations.5,10,24 Sonographers are instructed to use the worksheets to record Doppler velocities and angle of acquisition. Sonographers are instructed to try to acquire the image at each follow-up examination as close to the prior angles as possible to allow for noting subtle changes in velocity or qualitative properties of the Doppler waveforms. If a sonographer cannot achieve an image at the same angle they are instructed to place a note in the sonographer comments detailing why the same Doppler angle was not used.
Sonographer Training
All sonographers performing the TAMBE DUS examination are provided a link to online training materials. The online training materials provide narrated examples of all images to be acquired for the protocol and also review information regarding whom to contact with questions and instructions for filling out the worksheets.
Discussion
Many professional organizations have provided suggested imaging protocol guidelines for diagnostic ultrasound examinations20–22,25,26 and laboratory accreditation organizations mandate the use of specific protocols to ensure quality examinations are being performed.27–30 Adherence to specific protocols enhances diagnostic accuracy and ensures reproducibility of results from different imaging laboratories. 31 Adherence to strict protocols may also facilitate the development of new imaging practice standards and contribute to the development of new diagnostic criteria.
One of the limitations of ultrasound imaging has been that it is operator dependent.5,8,31 Facilitating the development of imaging protocols to answer specific clinical questions and teaching sonographers to utilize these new protocols may have the potential to reduce the operator variability in that protocols provide guidance for technical standards and required images that limit the ability of pathology to be missed. As protocols become more sophisticated this may lead to change in imaging standards, particularly in areas of medicine that are constantly developing new methods of treatment, such as BEVAR. Implementation of standards has been linked to superior practice and enforcing standards in laboratory accreditation has led to standardization of medical imaging, higher quality images, and improved patient outcomes.27,31–36
For this study, the imaging protocol was specifically designed for reproducibility of images over time. The sonographers were instructed to begin imaging the stent for the branched vessels at the level of the origin of the native artery. Imaging from the origin of the native artery serves as a standard landmark over time and allows for hemodynamic changes to be monitored in this arterial segment. This strategy was employed to ensure that sonographers were sampling the same level of the stent over time. Sonographers were also provided specific annotation to use to label images and asked to record the Doppler angle for each arterial segment at each examination. Sonographers were instructed to try and match the exact angle over time to ensure that the arterial segment was being imaged from similar planes and to be able to compare hemodynamics over time. Using different Doppler angles will alter the velocity values (see Appendix C in the online article). If a sonographer could not acquire the same Doppler angle on a subsequent exam they were asked to make a note on the sonographer worksheet as to why the same Doppler angle could not be used (i.e., different image planes and approaches were used due to bowel gas presence). In addition to the protocol details provided above, sonographers are also asked to image branch vessels downstream if an arterial segment is not visible. In this protocol, if no segment of the celiac artery is visualized, sonographers are asked to acquire a Doppler signal in the hepatic artery as it enters the liver hilum and the splenic artery as it enters the splenic hilum. This allows for evaluation of hemodynamic properties of these vessels to discern if proximal stenosis may be present (i.e., evaluate for tardus parvus waveform and/or other abnormalities of the waveform which may indicate proximal stenosis).
In addition to improving the quality of ultrasound imaging, specific protocols may also add information to other standard imaging surveillance techniques, such as CTA. DUS imaging has been able to identify thrombosed vessels that were missed on CTA imaging due to small size of the vessel/stent and metallic artifact (Figures 2 and 3).
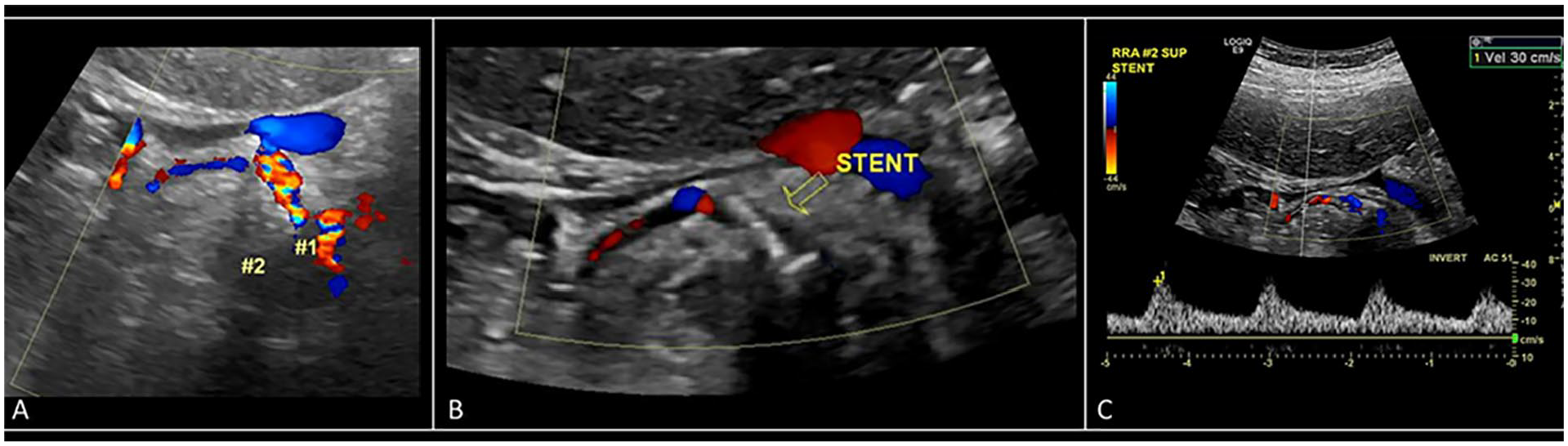
Example of a thrombosed renal artery on DUS examination in a patient with a fenestrated stent. Note. This lesion was missed on computed tomography angiography initially and the DUS led to changes in patient management based on this finding. Panel A shows 2 renal arteries. Panel B shows the stent and thrombosed renal artery. Panel C shows the Doppler waveform in right superior renal artery. DUS = duplex ultrasound.
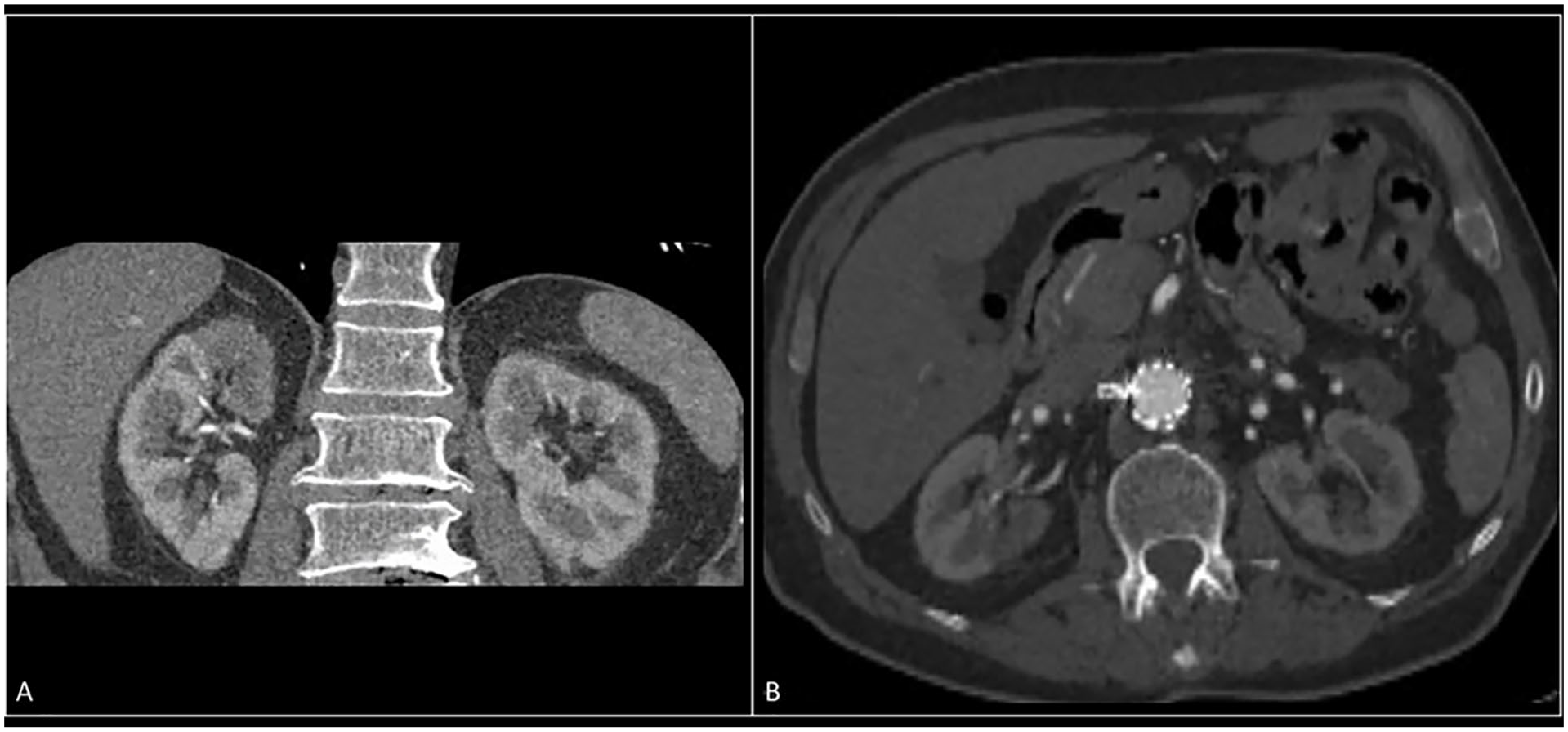
Computed tomography angiography images from patient described in Figure 2.
Finally, adherence to an imaging protocol has the potential for identifying signs of device failure prior to patient symptoms or events such as thrombosis which may lead to permanent end-organ damage. In this instance, using DUS in addition to CTA for surveillance of individuals with the TAMBE device has the potential to develop diagnostic criteria for evaluating stent patency and function through establishing velocity criteria for stenosis and change in function (such as PSV, EDV, or changes in velocities over time that may indicate stenoses and/or trickle flow in near occlusion).
As these procedures for treatment of TAAAs are increasing and off-the-shelf devices are becoming available, it is important to develop imaging protocols and determine how DUS may be used independently or serve as an adjunct to CTA for surveillance. This paper focused on the DUS examination which is being performed for follow-up of the TAMBE device. To determine the full role that DUS could play in surveillance of these patients, future studies that incorporate diameter measurements (to monitor aortic aneurysm sac size changes) and identify endoleaks are needed to compare DUS imaging to CTA imaging for following these patients.
Supplemental Material
sj-docx-4-jvu-10.1177_15443167211037082 – Supplemental material for Development of a Duplex Ultrasound Protocol for Baseline and Follow-Up Imaging of a Branched Aortic Endoprosthesis
Supplemental material, sj-docx-4-jvu-10.1177_15443167211037082 for Development of a Duplex Ultrasound Protocol for Baseline and Follow-Up Imaging of a Branched Aortic Endoprosthesis by Carol Mitchell, Jon S. Matsumura, Wendy Meadows, Mark A. Farber, Gustavo S. Oderich and Thanila Macedo in Journal for Vascular Ultrasound
Supplemental Material
sj-docx-5-jvu-10.1177_15443167211037082 – Supplemental material for Development of a Duplex Ultrasound Protocol for Baseline and Follow-Up Imaging of a Branched Aortic Endoprosthesis
Supplemental material, sj-docx-5-jvu-10.1177_15443167211037082 for Development of a Duplex Ultrasound Protocol for Baseline and Follow-Up Imaging of a Branched Aortic Endoprosthesis by Carol Mitchell, Jon S. Matsumura, Wendy Meadows, Mark A. Farber, Gustavo S. Oderich and Thanila Macedo in Journal for Vascular Ultrasound
Supplemental Material
sj-pdf-1-jvu-10.1177_15443167211037082 – Supplemental material for Development of a Duplex Ultrasound Protocol for Baseline and Follow-Up Imaging of a Branched Aortic Endoprosthesis
Supplemental material, sj-pdf-1-jvu-10.1177_15443167211037082 for Development of a Duplex Ultrasound Protocol for Baseline and Follow-Up Imaging of a Branched Aortic Endoprosthesis by Carol Mitchell, Jon S. Matsumura, Wendy Meadows, Mark A. Farber, Gustavo S. Oderich and Thanila Macedo in Journal for Vascular Ultrasound
Supplemental Material
sj-pdf-2-jvu-10.1177_15443167211037082 – Supplemental material for Development of a Duplex Ultrasound Protocol for Baseline and Follow-Up Imaging of a Branched Aortic Endoprosthesis
Supplemental material, sj-pdf-2-jvu-10.1177_15443167211037082 for Development of a Duplex Ultrasound Protocol for Baseline and Follow-Up Imaging of a Branched Aortic Endoprosthesis by Carol Mitchell, Jon S. Matsumura, Wendy Meadows, Mark A. Farber, Gustavo S. Oderich and Thanila Macedo in Journal for Vascular Ultrasound
Supplemental Material
sj-pdf-3-jvu-10.1177_15443167211037082 – Supplemental material for Development of a Duplex Ultrasound Protocol for Baseline and Follow-Up Imaging of a Branched Aortic Endoprosthesis
Supplemental material, sj-pdf-3-jvu-10.1177_15443167211037082 for Development of a Duplex Ultrasound Protocol for Baseline and Follow-Up Imaging of a Branched Aortic Endoprosthesis by Carol Mitchell, Jon S. Matsumura, Wendy Meadows, Mark A. Farber, Gustavo S. Oderich and Thanila Macedo in Journal for Vascular Ultrasound
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: C.Mitchell: Davies Publishing, Inc, textbook author, Elsevier, Wolters-Kluwer, author textbook chapters, and W. L. Gore & Associates contracted research grants to University of Wisconsin-Madison; JS Matsumura: University grants from Abbott, Cook, Gore, Endologix, and Medtronic; W Meadows: W. L. Gore & Associates contracted research grants to University of Wisconsin-Madison; M Farber: WL Gore- consultant, clinical trial support; Centerline Biomedical- stock options, consulting; Cook Medical research Support, clinical trial support, consulting; GS Oderich: Consulting- Cook Medical Inc., WL Gore, GE Healthcare, and Centerline Biomedical; Research grants- Cook Medical Inc., WL Gore, and GE Healthcare; Scientific advisory board- Cook Medical, Centerline Biomedical, and GE Healthcare; Investigational, off-label use of devices- Cook Fenestrated and Branched Grafts, Gore Branched Technology; T Macedo: None
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This trial was funded by W.L. Gore and Associates.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.