
Abstract
Conventional duplex ultrasound is a well-established imaging modality for the surveillance of endovascular aortic repair. A unique case of liquefied thrombus mimicking an endoleak on color and spectral Doppler ultrasound is presented. Contrast computed tomography and contrast-enhanced ultrasound were used to further assess the patient and exclude an endoleak.
Keywords
Case
A 79-year-old man presented for routine surveillance of his endovascular aortic repair (EVAR) performed 18 months before for the treatment of a 5.1-cm abdominal aortic aneurysm. Previous duplex ultrasound (DUS) examinations were normal with a stable sac size of 5.2 cm. On this occasion, the aortic sac appeared to have increased in size from 5.2 to 5.5 cm and demonstrated a crescent-shaped internal cavity with pulsatile flow surrounding the central graft and thrombus (Figure 1). Spectral Doppler sampling revealed a pulsatile low-velocity to-and-fro waveform (Figure 2). The assumption was made that this appearance represented a new endoleak; however, the source could not be identified. Contrast-enhanced ultrasound (CEUS) was not available at this center, and the patient was referred for a contrast computed tomography angiogram (CTA) instead. Computed tomography angiogram revealed no evidence of endoleak (Figure 3); however, the radiologist also commented about a small increase in aortic sac size and considered the possibility that an occult endoleak may be present.
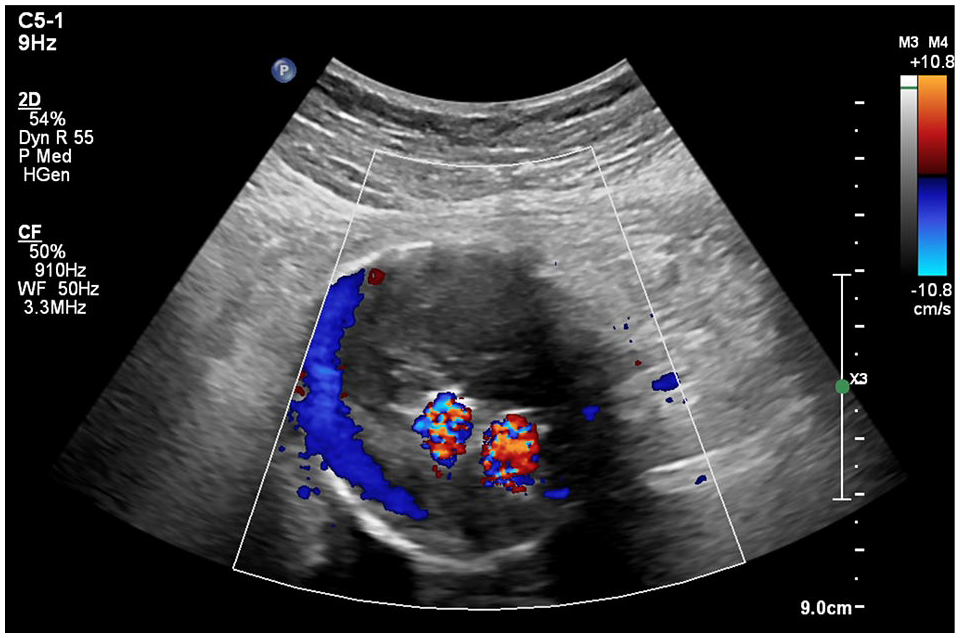
Color Doppler ultrasound demonstrated flow within the abdominal aortic aneurysm.
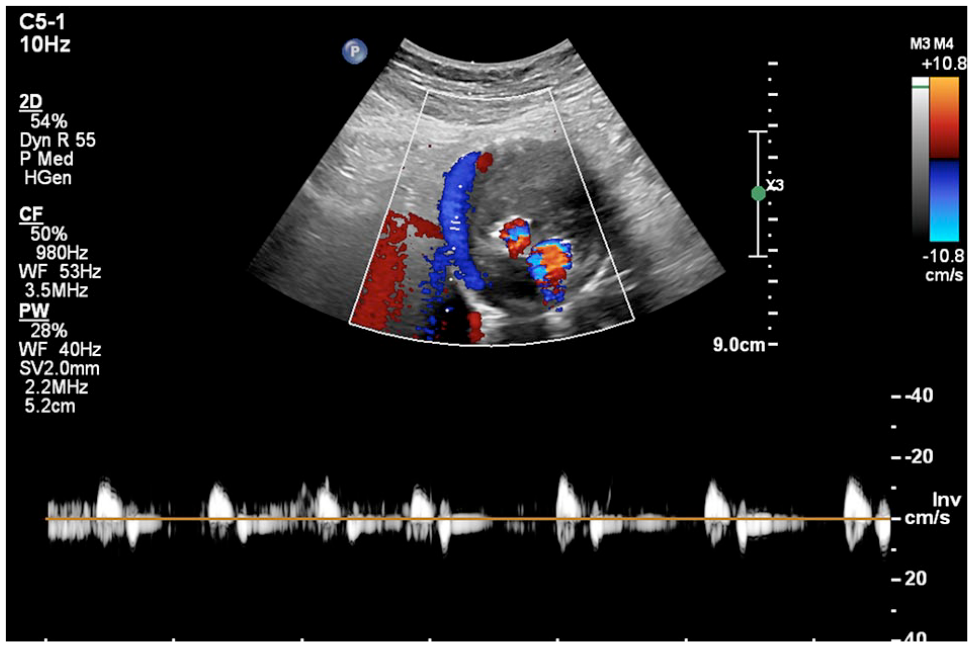
Spectral Doppler sampling revealed a pulsatile low-velocity to-fro waveform.
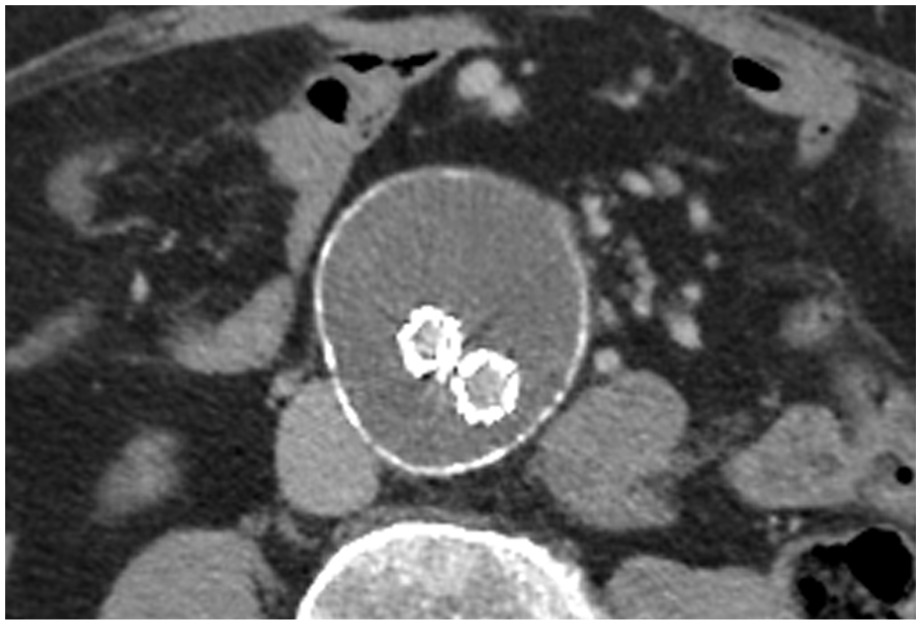
Computed tomography angiogram detected no endoleak.
The patient was then referred for CEUS at our regional tertiary teaching hospital. The identical DUS appearance was again noted as shown in Figure 1. Contrast-enhanced ultrasound was performed on a Philips EPIQ Elite system using Definity perflutren microspheres (Lantheus, Massachusetts). The examination showed no contrast entering the aneurysm sac at any phase of imaging lasting a total of 5 minutes (Figure 4) effectively ruling out an endoleak as the cause of the duplex appearance.
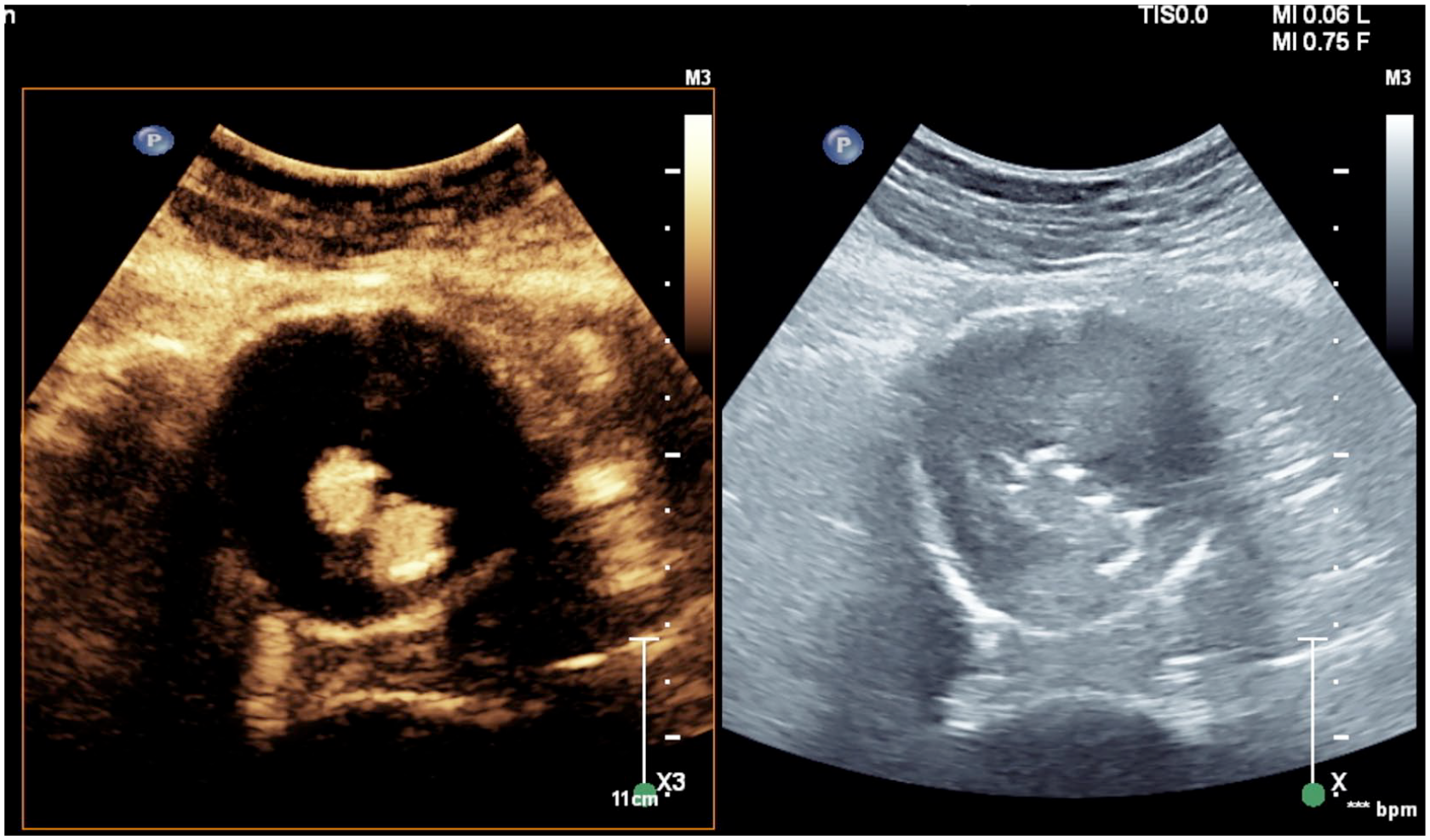
Contrast-enhanced ultrasound demonstrated no contrast microspheres within the abdominal aortic aneurysm sac, confirming the absence of endoleak.
This is an unusual case where liquefied thrombus within the aneurysm sac swirls around in response to arterial pulsation of adjacent structures, generating a Doppler signal that mimics an endoleak. The DUS appearance is real (not artifactual) in the sense that it represents real flow; however, it is not blood flow. The absence of ultrasound contrast agent within the aortic sac on CEUS imaging conclusively proves that the Doppler signal seen on DUS does not represent an endoleak.
Discussion
Conventional DUS is a well-established imaging modality for the surveillance of EVAR.1,2 Although CTA has a better sensitivity to endoleak detection than DUS, CTA is not suitable for long-term follow-up due to ionizing radiation, use of nephrotoxic contrast, and higher costs.1,3 Contrast-enhanced ultrasound plays an increasingly important role in the evaluation of EVAR because it combines the advantages of DUS with the benefit of intravascular contrast agents. Contrast-enhanced ultrasound has been found to be more sensitive at detecting endoleaks than CTA, particularly in patients with slow endoleaks. 4 In the past, CEUS was considered a trouble-shooting modality in difficult cases or in cases where DUS and CTA show conflicting findings; however, CEUS is now being increasingly integrated as a routine component of post-EVAR surveillance, reducing the need for CTA.5,6
Contrast-enhanced ultrasound is easy to implement and perform and should be a standard part of the imaging repertoire in vascular laboratories attached to vascular surgical and interventional units.7,8 In general, ultrasound contrast agents have an excellent safety profile. 9 Minor, transient, and self-limiting symptoms such as headache, back pain, nausea, chest pain, and dizziness may occur in a small percentage of patients. Severe anaphylactoid reactions are rare (approximately 1:10 000) 10 and occur in patients with hypersensitivity to polyethylene glycol (PEG). 11 Suspected PEG hypersensitivity is the only contraindication to the administration of contrast agents containing PEG, such as Definity, which was used in this case. Users of contrast agents must have access to monitoring and resuscitation equipment and must be able to recognize and manage an anaphylactoid reaction.8,10 In a hospital setting, resuscitation teams or emergency departments are readily available to assist in the unlikely event of anaphylaxis.
Our case demonstrates an unusual DUS pitfall and the usefulness of CEUS in reaching the correct diagnosis. Had CEUS been available when the misleading DUS appearance was first identified, CTA could have been avoided, shortening the time to diagnosis, saving the patient another radiation dose as well as nephrotoxic contrast, and reducing health care costs.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.