
Abstract
Introduction:
The toe-brachial index is typically an adjunctive examination to the ankle-brachial index, which has long been the primary physiologic modality for diagnosing peripheral arterial disease. The goal of this project was to determine toe-brachial index reliability, particularly with patients with diabetes.
Methods:
We compared duplex ultrasound to the ankle-brachial index and toe-brachial index on 100 patients (200 legs) with suspected symptomatic peripheral arterial disease. Duplex ultrasound stenosis in the femoral/popliteal/infrapopliteal arteries was at least a doubling of velocity between adjacent segments. A blunted systolic Doppler waveform was consistent with proximal occlusive disease. Normal physiologic ranges were arbitrarily set as ankle-brachial index 1.2 to 0.9 and toe-brachial index 0.9 to 0.5. We calculated overall sensitivity/specificity values by averaging.
Results:
Both physiologic modalities had overall low sensitivity (ankle-brachial index 62%, toe-brachial index 56%). In diabetics, ankle-brachial index sensitivity was 61% and toe-brachial index sensitivity was 57%. Sensitivity improved in the presence of inflow disease (ankle-brachial index 78%, toe-brachial index 63%). Both modalities had good overall specificity (ankle-brachial index 96%, toe-brachial index 86%). In patients with diabetes, the ankle-brachial index specificity was 94% and toe-brachial index specificity was 79%. Both physiologic modalities had identical accuracy (0.43) in comparison to duplex ultrasound.
Conclusion:
Routine toe-brachial index in conjunction with the ankle-brachial index may not be clinically productive.
Keywords
Introduction
Atherosclerotic lesions in the peripheral arteries can cause claudication or tissue loss by reducing, or eliminating, oxygenated blood to the limb. 1 The ankle-brachial index (ABI) and the toe-brachial index (TBI) are physiologic tests to diagnose peripheral arterial disease (PAD). 2 Compliant arterial walls allow a diagnosis of true arterial blood pressure while medial sclerosis hardens the arterial wall resulting in an artifactually elevated pressure reading. 3 Medial sclerosis does not affect the digital microcirculation to the same degree as it does to the medium sized infrapopliteal arteries thus offering an attractive alternative site for evaluating peripheral arterial circulation of the lower extremity.4-6
Methods and Materials
We used a Philips iU-22 duplex ultrasound (DUS) scanner (Andover, MA) with a linear segmental array L9-3 MHz probe. Peak systolic velocities (PSVs) were recorded in the longitudinal plane from the inflow arteries, namely, the common femoral, deep femoral, superficial femoral, and popliteal, and from the runoff arteries (infrapopliteal), the posterior tibial and anterior tibial. A Unetixs MultiLab pulse-volume machine (Warwick, RI) recorded the ABI in all 200 legs with an 8-MHz continuous wave probe and obtained the TBI with a photoplethysmographic diode sensor. Both ABI and TBI were performed only once on each patient. Data were stored on an Excel spreadsheet (Microsoft Corporation, Redmond, WA).
Sonographic presence of occlusion or stenosis confirmed the presence of PAD. Arterial stenosis was defined as a >50% stenosis with, at minimum, a doubling of the PSV between adjacent arterial segments.7,8 Disease localization was defined as either inflow or runoff vessels. The normal ABI range9,10 was arbitrarily set as 1.2 to 0.9 and the normal TBI range11-15 was 0.9 to 0.5. ABI and TBI values below these ranges were “abnormal.” Values above these ranges were “artifactually elevated,” and, for the purpose of this project, were included as normal values.
We randomly selected 100 patients and tested 200 legs. This patient cohort consisted of in-patients with heel and toe ulcers and outpatients with suspected exercise pain. Diabetes mellitus (DM), systemic hypertension, obesity, and smoking were the predominant vascular risk factors and recorded through a review of the patient’s electronic chart. We excluded amputees and patients with bypass grafts or endovascular procedures. The study calculated specificity and sensitivity in several subsets of patient’s legs (Figure 1).
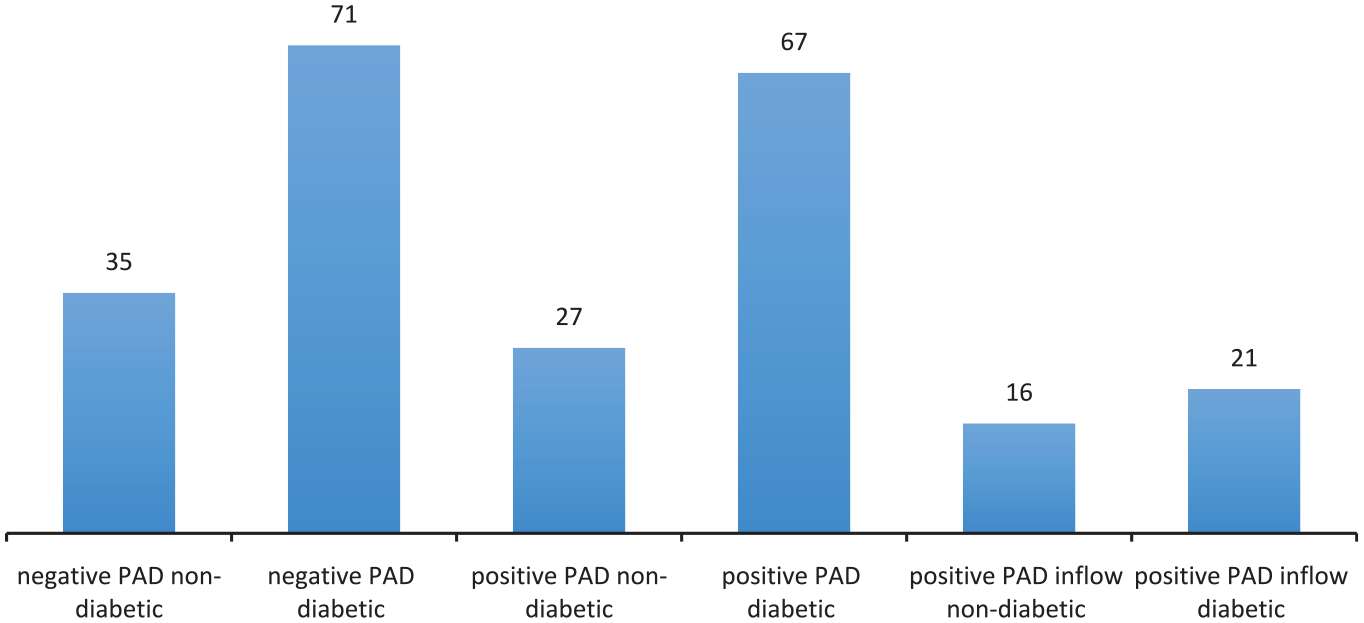
Breakdown of 200 legs that are negative or positive for PAD by DUS, nondiabetic or diabetic. PAD = peripheral arterial disease; DUS = Duplex Ultrasound.
Cohen’s kappa (κ) statistic expressed accuracy for the 62 legs negative for DM and 138 legs positive for DM.
Results
Legs negative for PAD (nondiabetic) had ABI specificity 97% and TBI specificity 93%. Legs negative for PAD (diabetic) had ABI specificities of 94% and TBI specificities of 79% (Figure 2).
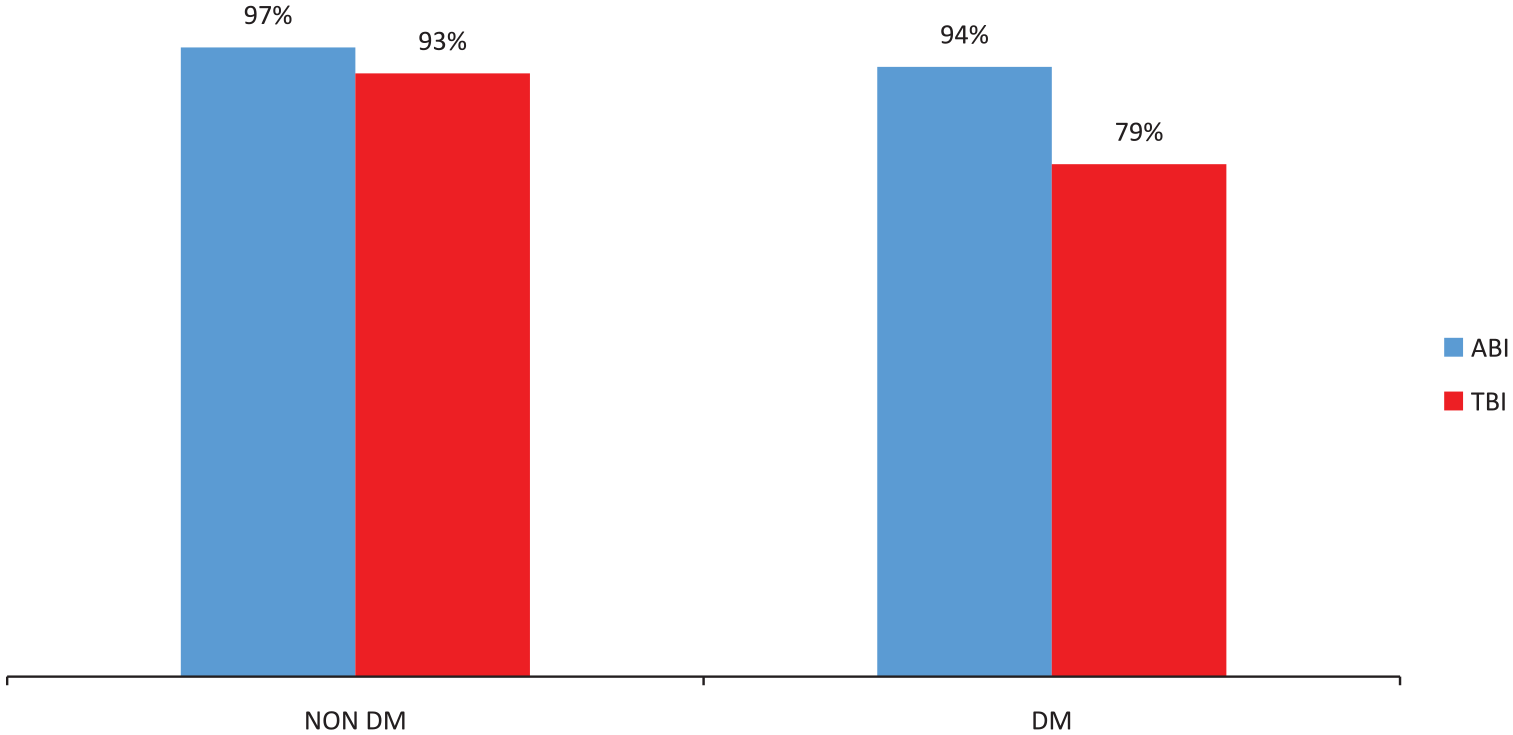
Specificity of ABI and TBI for nondiabetic and diabetic patients with negative DUS.
Legs positive for PAD (nondiabetic) had ABI sensitivities of 52% and TBI sensitivities of 48%. Legs positive for PAD (diabetic) had ABI sensitivities of 40% and TBI sensitivity 51%.
Legs positive for PAD inflow disease (nondiabetic) had ABI sensitivities of 75% and TBI sensitivities of 63%. Legs positive for PAD inflow disease (diabetic) had ABI sensitivities of 81% and TBI sensitivities of 62% (Figure 3).
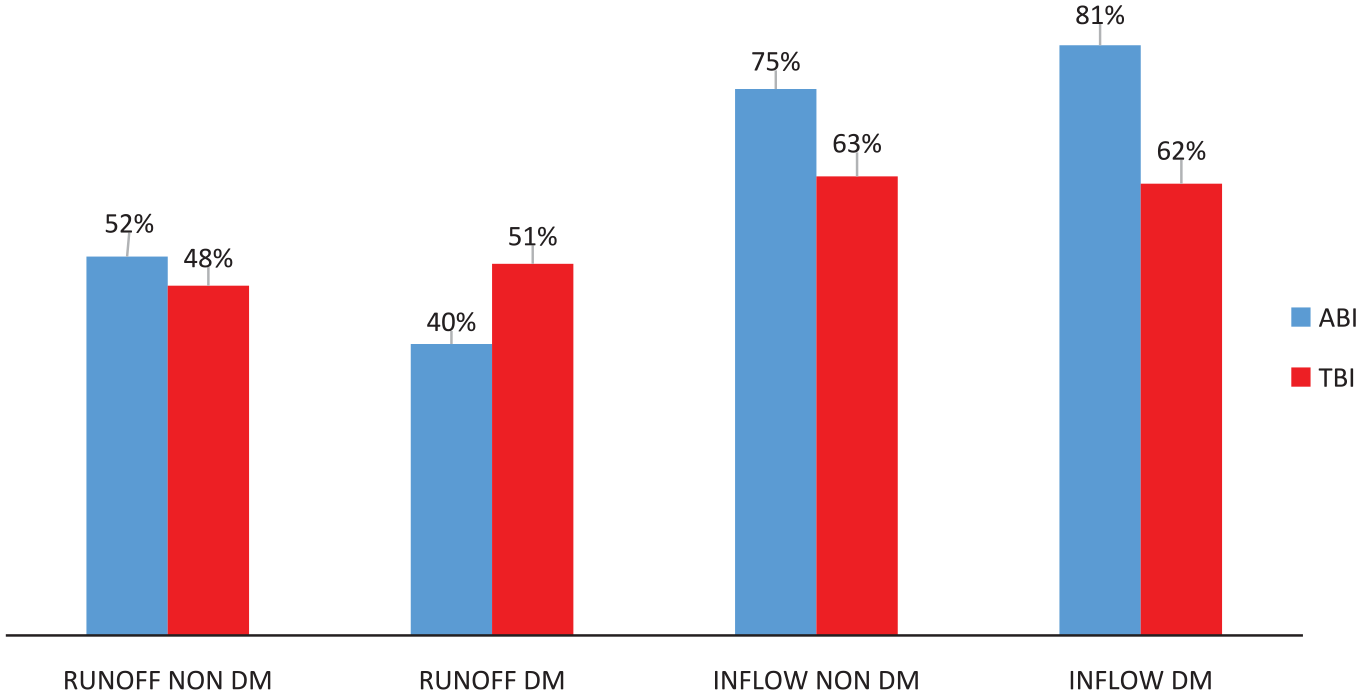
Sensitivity of ABI and TBI, for nondiabetics and diabetics, with inflow or runoff disease by DUS.
ABI and TBI accuracy (k agreement) with nondiabetic legs was ABI 0.50 and TBI 0.54.
Accuracy with diabetic legs was ABI 0.35 and TBI 0.31 (Figure 4).
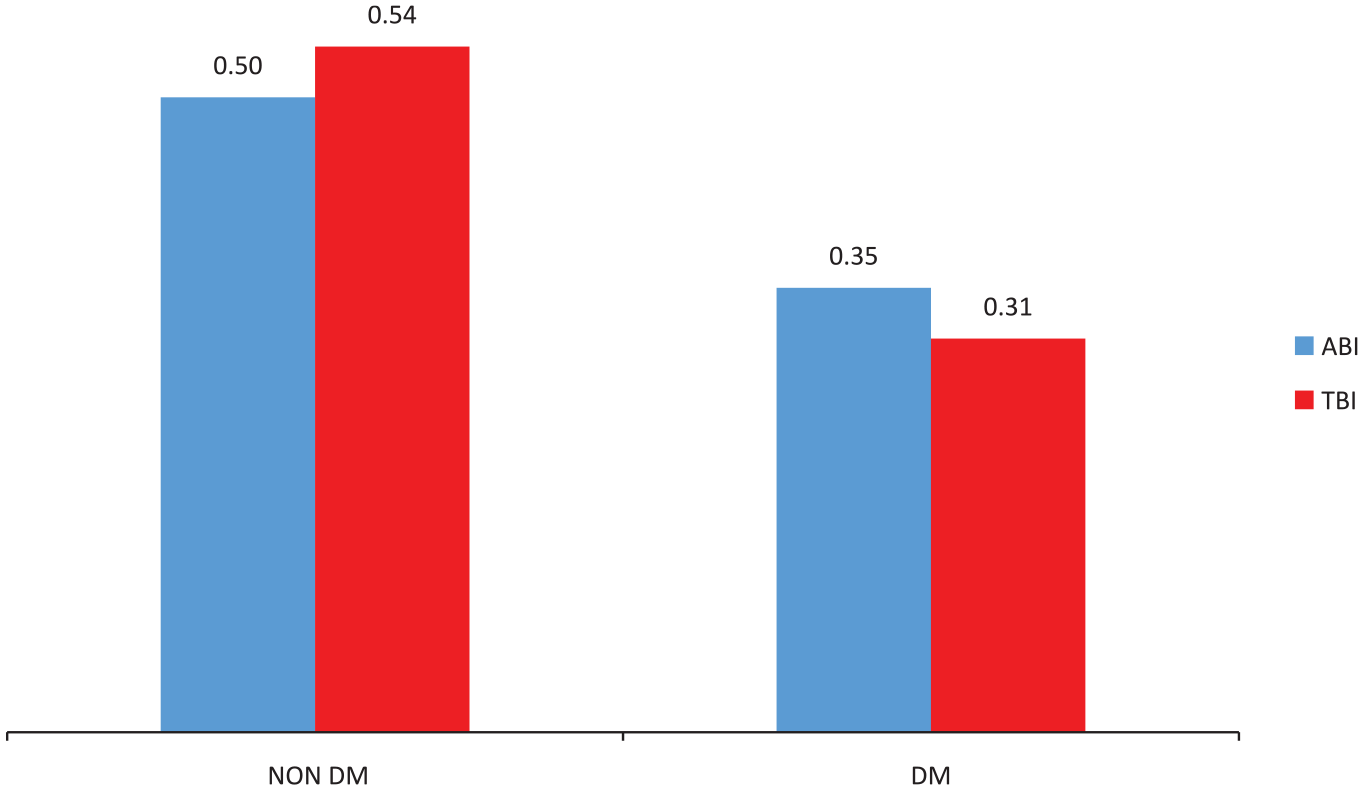
Overall accuracy (K number) of ABI and TBI compared to DUS.
Discussion
Peripheral arterial disease is a condition that results in decreased lower extremity perfusion and symptomatic PAD, and is a major health concern for hundreds of millions of patients.16,17
Hemodynamically significant peripheral arterial lesions were correlated to physiologic results. Moderate lesions were not recorded because, per the Bernoulli equation, they do not produce pressure gradients. 18 We used monophasic waveforms to diagnose probable proximal occlusive disease.19,20
In the hands of trained operators, DUS is accurate, 21 particularly in the femoral/popliteal arteries, and less accurate below the knee. 22 Duplex ultrasound was our “gold standard” for evaluating physiologic modalities. 23
Specificity of both modalities was good for non-PAD, nondiabetic legs ABI (97%) and TBI (93%). ABI specificity with non-PAD diabetic legs was 94%; however, TBI specificity was lower (79%) in those same non-PAD diabetic legs. This resulted in a higher number of false positives. A test with low specificity should carry high sensitivity; however, low TBI sensitivity does not bear this out.
ABI sensitivity was 52% for patients who were positive for PAD, and nondiabetic, and TBI sensitivity was 48% for these patients. For patients positive for PAD, and diabetic, the ABI sensitivity was 40% and the TBI sensitivity was 51%, which was better than the ABI but still unacceptable. These results confirm reports of low ABI sensitivity. 24 Although TBI sensitivity was better than ABI for diabetic PAD patients, these data confirm reports of low TBI sensitivity. 3
The prognostic value of the ABI is widely accepted, 12 even though ABI underestimates parallel occlusive disease in the infrapopliteal arteries. 2 This might explain improved ABI sensitivity in the presence of inflow PAD, 75% in nondiabetic legs and 81% in diabetic legs. Toe-brachial index sensitivity with inflow PAD was essentially the same in nondiabetic legs (63%) and diabetic legs (62%). In the case of inflow disease, ABI sensitivity was superior to TBI.
In the 13 legs with a normal ABI, positive for PAD and negative for diabetes, 5 legs (38%) had an abnormal TBI. Of the 40 legs with normal ABI, positive for PAD and positive for diabetes, 17 legs (43%) had an abnormal TBI. Although the TBI identified more legs with inflow disease, particularly in patients with diabetes, it did not diagnose even half of the ABI false negative legs with inflow disease.
Overall accuracy (k number) of ABI and TBI was in the acceptable range (0.50 and 0.54, respectively) for nondiabetics and in the lower range (0.35 and 0.31) for diabetics, confirming that “TBI has a variable diagnostic accuracy.” 25
There remains insufficient information about the nature of toe-brachial indices. 26 The diagnostic criteria for a pathologic TBI remains ambiguous 11 and standardized normal values still need to be established. 2 Toe-brachial index reliability is also adversely affected by inconsistent equipment and single digital measurements, 22 demonstating inherent inconsistency 11 and lack of pretest resting. 27 For this project, there was no resting or warming times, calibration was infrequent, and we obtained pressures exclusively from the great toe. Finally, the physiologic examinations included in this study were done without cross-checking for accuracy. Despite these limitations, however, this article presents interesting data about TBI utility.
According to numerous authors, TBI compensates for limited ABI reliability 5 secondary to infrapopliteal artery stiffness in diabetics 3 and is an appropriate modality to identify PAD in the presence of normal or elevated ABIs. 9 Patients with elevated ABI are at higher risk of cardiovascular disease. 6 Many clinicians recommend that TBI should be routinely included in the evaluation for PAD28-30 because TBI derives information from digital blood vessels that are usually less affected by calcification. 4
Our data, however, like that in Stoekenbroek’s 2015 article in the European Journal of Vascular and Endovascular Surgery, shows that ABI and TBI are strongly associated and TBI does not allow for earlier detection of ischemia in diabetes. 31
Conclusions
The TBI and ABI moved concordantly for both diabetics and nondiabetics. Both modalities demonstrated low sensitivity, moderate specificity, and almost equivalent accuracy. These results suggest that the TBI may not be adequate as a routine adjunctive examination to the ABI. There is also a need for additional research in this area of physiologic testing.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.