
Abstract
Recent research into mammalian cortical neurophysiology, after 6 decades of Berger's seminal work on electroencephalography, has shifted the older concept of interictal epileptiform activity (IEA) away from that of a mere electrographic graphoelement of relevance to diagnostic implications in epilepsy. Instead, accumulating information has stressed the neuropsychological implications, cognitive and/or behavioral consequence of these electrophysiological events, which are the phenotypic expression of aberrations of actual biophysical cellular function.
We feel that this review is germane to neuropsychiatry, however, a rather neglected area of research. There is a great scope for brain-behavior-EEG research in the future that can be complimented by other techniques of “neurobehavioral electrophysiology.” This review does not address the “pearls, perils and pitfalls” in the use of EEG in epilepsy, but critically and systematically reappraises the published electroencephalographic correlates of human behavior. We reiterate that epileptiform and other paroxysmal EEG dysrhythmias unrelated to clinical seizures do have neuropsychological, cognitive and/or behavioral implications as seen in the various neuropsychiatric and neurobehavioral disorders discussed in this article. IEA and EEG dysrhythmias should neither be ignored as irrelevant nor automatically attributed to epilepsy. The relevance of these EEG aberrations in the disorders of the brain-mind interface extend beyond epilepsy, and may be an electrophysiological endophenotype of aberrant neuronal behavior indicative of underlying morpho-functional brain abnormalities.
Magnetoencephalography (MEG), data fusion models (EEG-fMRI-BOLD), transcranial magnetic stimulation (TMS), evoked potentials (EP); intracranial electrophysiology, and EEG neurofeedback complemented by current functional neuroimaging techniques (fMRI and PET) would certainly help in further understanding the broader relationship between brain and behavior.
Keywords
INTRODUCTION
Ever since the introduction of the electroencephalogram (EEG) by the psychiatrist Hans Berger, 1 an important target of clinical neurophysiology had been to identify the electroencephalographic correlates of human behavioral disorders and psychopathologies. Many pioneering EEG laboratories were in psychiatric hospitals, and over the years, many of studies on the EEG correlates of abnormal human behavior and psychopathology have become evident. However with the advent of neuroimaging technology and other advances made in both neurology and psychiatry, studies on electrophysiological aberrations in behavioral and neuropsychiatric disorders have become scarcer over the past few decades.
Over the course of the last six decades, a voluminous literature has emerged that has substantiated a high prevalence of conventional EEG findings in the psychiatric population. Although the existing EEG literature is replete with reports of abnormalities in association with different neuropsychiatric disorders, only a few generalizations can be made between particular EEG patterns and specific syndromes. The strong correlation that has been established between EEG abnormalities and epilepsy has overshadowed the more complex relationship between EEG abnormalities and psychiatric disorders.
A number of EEG phenomena have been consistently shown to be more prevalent in psychiatric populations. While the primary value of EEG in neuropsychiatry has been in differentiating brain disease from primary psychiatric disorders, recent advances in EEG and other electrophysiology techniques have emerged as powerful tools in exploration of the biological substrate for neuropsychiatric disorders. This knowledge will not only contribute to our understanding of the basic pathophysiology underlying psychopathologies and altered behavior, but also contribute to developing better bio-psychosocial formulations and treatment plans for individual patients. The subject will be discussed under several sections: Diagnostic and behavioral implications of interictal epileptiform activity (IEA), IEA/cerebral dysrhythmia in normal subjects, IEA/cerebral dysrhythmia in various neuropsychiatric disorders; and IEA/cerebral dysrhythmia in neurobehavioral disorders.
Diagnostic and behavioral implications of IEA/cerebral dysrhythmia
The EEG represents summated post synaptic synchronized excitatory or inhibitory potentials in the apical dendrites from a large ensemble of cortical pyramidal neurones in the superficial neocortex. The EEG interictal spike-wave is representative of the intracellular burst of dendritic action potentials from the pyramidal cells which represents the intracellular “paroxysmal depolarizing shift” followed by hyperpolarization. The relationship between distinctive interictal epileptiform electroencephalographic patterns and epileptic seizures has remained unchallenged. However, there are controversies relating to the interictal spikes (IIS)/epileptiform activity (IEA) and epileptogenesis; “Do IIS/IEA trigger seizures or protect against them?” 2,3 The physiological, pathological, and clinical meaning of interictal spikes does remain controversial. Source-related parameters (source geometry: spatial extent, location, synchronization); properties of EEG signals (amplitude of spikes, amplitude gradient along intracerebral electrodes, topography over scalp electrodes); its spatio-temporal organization; frequency, occurrence, and distribution of IISs (scalp-EEG, high resolution EEG, magnetoencephalography (MEG), depth cerebral EEG) are crucial variables for explicating the role of IIS/IEA in epileptogenesis. Simultaneous HR-EEG (high resolution EEG) and functional magnetic resonance imaging (EEG-fMRI) recording has now become a noninvasive tool for investigating epileptogenic networks. 4 HR-EEG (high resolution EEG) and MEG allow the recording of cerebral electromagnetic activities with excellent temporal resolution and now constitute real methods of Electric and Magnetic Source Imaging. Furthermore, the sensitivity of whole-head MEG versus intracranial EEG (ICEEG)/depth electrode EEG in the study of interictal epileptiform spikes have been found to be comparable.
Subclinical electroencephalographic epileptiform discharges in neurobehavioral and neuropsychiatric disorders are not uncommon. The clinical, behavioral, diagnostic and therapeutic implications of these epileptiform discharges, as well as the significance of other EEG cerebral dysrhythmia, have not been fully examined. Currently, the only interpretation for distinctive epileptiform electroencephalographic patterns is epileptic seizures. Given the prevailing dogma of not treating EEGs, these potential aberrations are either disregarded as irrelevant or are misattributed to indicate epilepsy.
The IEA is more than an epiphenomenon, and not simply an EEG graphoelement. IEA has been documented to be associated with altered neurophysiology, neurometabolism, neurovascular changes, and neurochemical milieu resulting in cognitive, behavioral and affective changes in disorders without clinical seizures. 5,6 Indeed, subclinical IEA represents an index of brain functioning, with resultant neuropsychological abnormalities being implicated in specific cognitive disorders such as autistic spectrum disorders, attention deficit hyperactivity disorder (ADHD) and Landau-Kleffner syndrome (LKS). Subclinical IEA in such settings should be viewed as a biological variable or electrophysiologic endophenotype marker contributing to the development of neuropsychiatric and neurobehavioral disorders.
The seminal publication by Prince and Wilder 7 advanced some of the earliest insights into the functional significance of IEA. They have stressed, not the cellular marker of IEA, i.e., paroxysmal depolarizing shift (PDS), instead on the zone of “surround” inhibition surrounding the focus of IEA. This results in functional impairment of a neuronal population (remote neural inhibition) during the IEA with measurable cerebral metabolic and blood flow changes. Future efforts targeted to achieve true integration of electrical and hemodynamic measures of neuronal activity using data fusion models such as simultaneous recording of brain activity (EEG) and neurophysiological modalities (blood oxygen level-dependent (BOLD) functional MRI) should be able to yield insights that reach beyond those obtained by each technique individually. We will be able to understand the dynamic effects of IEA on normal brain function, cerebral epileptogenic networks, and the cause of neuropsychological regression in “cognitive epilepsies” unrelated to clinically overt seizures.
The relationship of IEA to neuropsychological function and resultant cognitive-behavioral changes has been convincingly elucidated by the work of Browne et al. 8 where they documented impaired auditory reaction times during the initial period following the onset of 3 Hz spike and wave IEA. Ten years after the publication of Browne et al., another study further strengthened the neuropsychological effects of focal IEA on written and spatial perception and memory. 9 In this study, left hemisphere IEA were reported associated with reading memory impairment, whereas right hemisphere IEA were associated with spatial memory impairment. Other similar studies have lent evidence that focal IEA could interrupt the normal hemispheric language and spatial orientation performance. 10 –13 Few studies explored the effect of the location of interictal spikes on visual perception and reaction time. 14 –16 These studies documented visual misperception and reaction time to be affected just before the spike onset until the termination of the after-going slow wave. The amplitude of the after-going slow wave of the IEA was found to correlate with longer reaction time as the slow wave component is associated with neuronal inhibition. Thus, focal spike-induced transient cerebral dysfunction can disrupt auditory, somatosensory, motor, visual, and memory functions commensurate with alterations in cerebral metabolic and blood flow rates. The spike wave discharge represents an alternation of overexcitation (spikes) and overinhibition (waves), and the recurrent overinhibition interferes with gamma activity correlated cognitive processes. High-frequency neural synchrony is critical for cognitive and linguistic development, 17 and thus the recurrent inhibition could explain the co-existence of infraclinical seizures and the simultaneous frequently observed cognitive deficit symptoms.
The subclinical or infraclinical IEA in pediatric neurobehavioral disorders may represent an epiphenomenon of cerebral dysfunction or underlying cortical morpho-functional abnormalities, and/or reflect a brain neurophysiological disorder which is not sufficient to be expressed as epilepsy. This phenomenon is postulated to be due to the lack of properly functioning corticocortical fibers which restrict the spread of epileptiform activity from one brain area to another and prevent its evolution to a clinical seizure. The subclinical epileptogenesis in the developing maturing brain may also directly impair cognitive-behavioral functioning by way of “transient cognitive impairment” (TCI) mechanisms, which is well described by Binnie and his colleagues. 9,18 The practical implications of TCI in pediatric neurobehavioral disorders could be taken as prima facie evidence of cerebral dysfunction and a few randomized, double-blind controlled trials of antiepileptic drugs have reported on behavioral improvement by suppressing subclinical IEA. 19 –22
Given the far-reaching implications of existing studies, focal IEA should therefore not be assumed to be clinically benign, and available information does suggest therapeutic benefit from antiepileptic drugs to suppress all IEA. The maxim “treat the patient, not the EEG” may be an oversimplified clinical standpoint, as evidence from the anecdotal reports suggested that antiepileptic pharmacotherapy improves the neuropsychological deficits.
Should the practice of antiepileptic treatment response only limited to clinical seizure remission be revised? Do we under treat patients with epilepsy by aiming only to suppress clinically obvious seizures? The classical principal of only treating clinical seizures perhaps needs to be reconsidered. The benefit of pharmacotherapy for children without epilepsy with behavioral problems and EEG epileptic discharges needs to be clarified. The question arises whether the cognitive and behavioral problems are related to the presence of the epileptic discharges, and this can be answered by future randomized trials; involving blinded pre-and post-treatment assessments of behavioral, cognitive, and neuropsychological domains as outcome measures. This will be further discussed under the section on pediatric neurobehavioral disorders.
IEA/CEREBRAL DYSRHYTHMIA IN NORMAL NONEPILEPTIC POPULATION
Numerous epidemiological studies have documented normative EEG data in healthy persons and several reports of EEG dysrhythmia in nonepileptic general population. In this paper, EEG cerebral dysrhythmia denotes isolated episodic paroxysmal bursts of slow activity, controversial/anomalous spiky waveforms and/or truly interictal epileptiform activities (IEA). The tumult of World War II was conducive for large scale studies on EEG abnormalities in the military and air force personnel. It is not rare for the neurologists to find such interictal abnormalities in the EEGs of nonepileptic patients, and for neuropsychiatrists to come across such EEG paroxysmal dysrhythmias, both epileptiform and nonepileptiform in association with various psychopathologies.
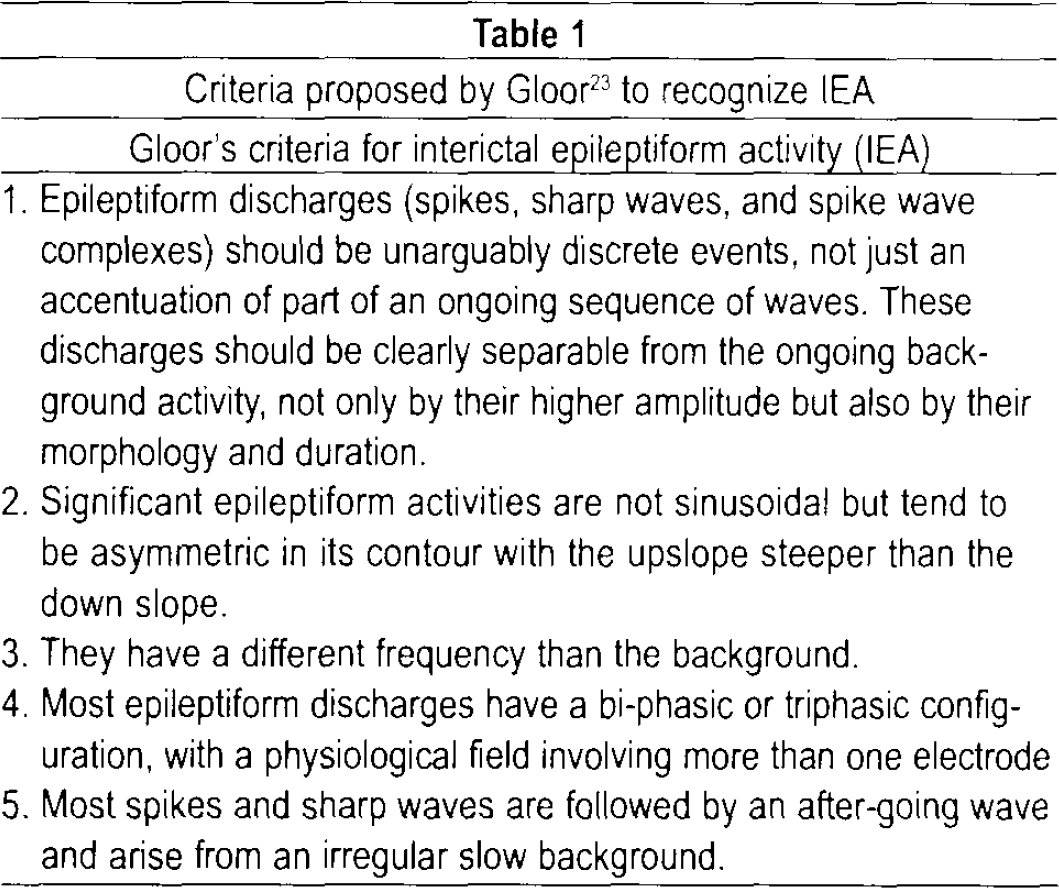
The discovery of epileptiform abnormalities on electroencephalographic screening in these settings that are unrelated to a clinical seizure disorder should be approached with caution and not misconstrued as synonymous to epilepsy. In this regard, it is critical to be familiar with criteria that have been formulated for the proper identification of IEA and avoid over-reading of the EEG. The proper identification of IEA is based on Gloor's five point criteria, 23 (Table 1).
Criteria proposed by Gloor 23 to recognize IEA
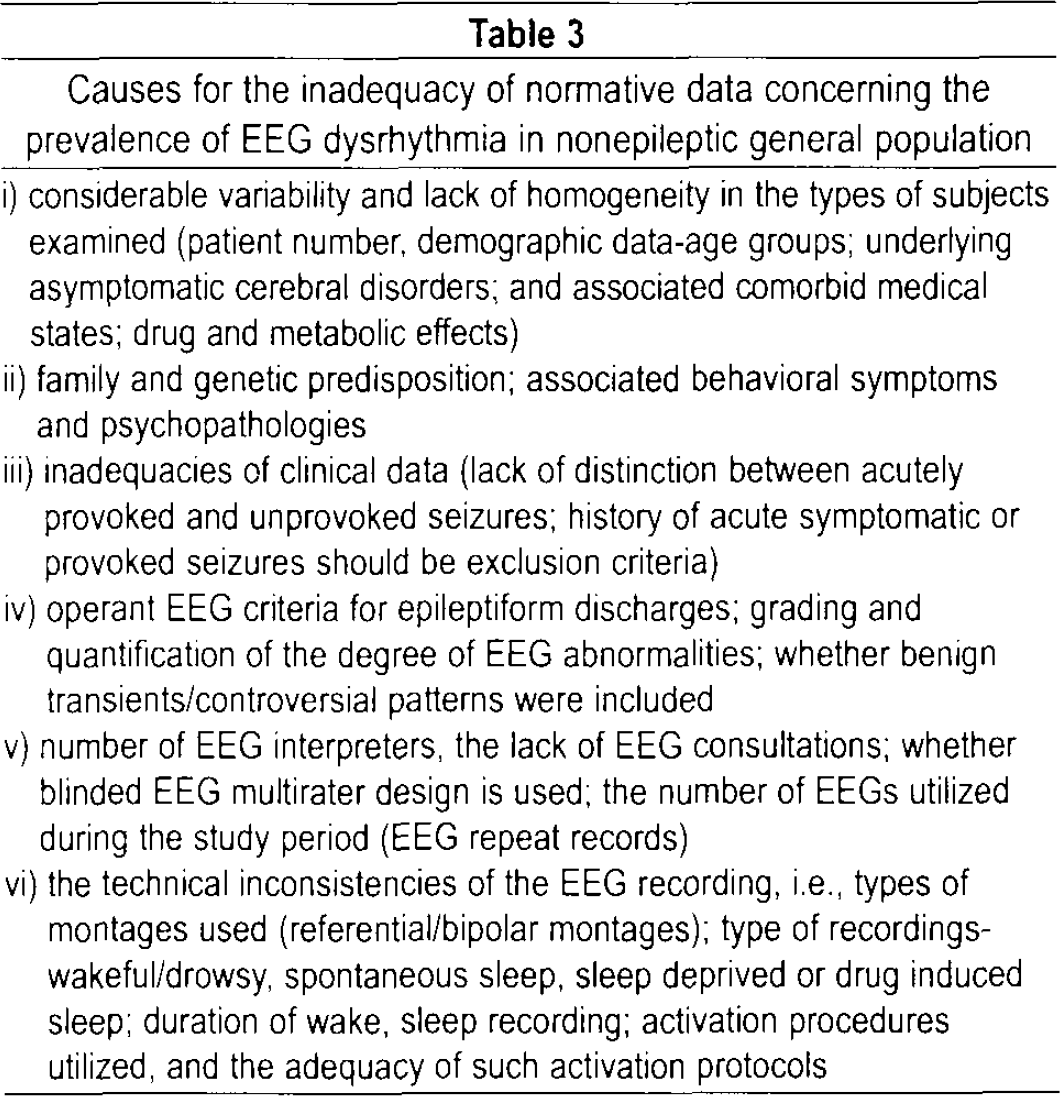
Numerous epidemiological studies of large “healthy” nonepileptic populations were conducted to define and establish the limits of the normative EEG. Such studies have documented a wide range of prevalence rates of EEG dysrhythmia in the nonepileptic general population. IEA ranged from 0.8% to 18.6% in reportedly normal children and 0.3% to 12.3% in reportedly normal adults. These studies have been summarized in Table 2. We predict that the reasons for the wide range of normative data are due to the inadequacies of the methodological design as shown in Table 3.
Summary of studies of EEG dysrhythmia in normal nonepileptic population
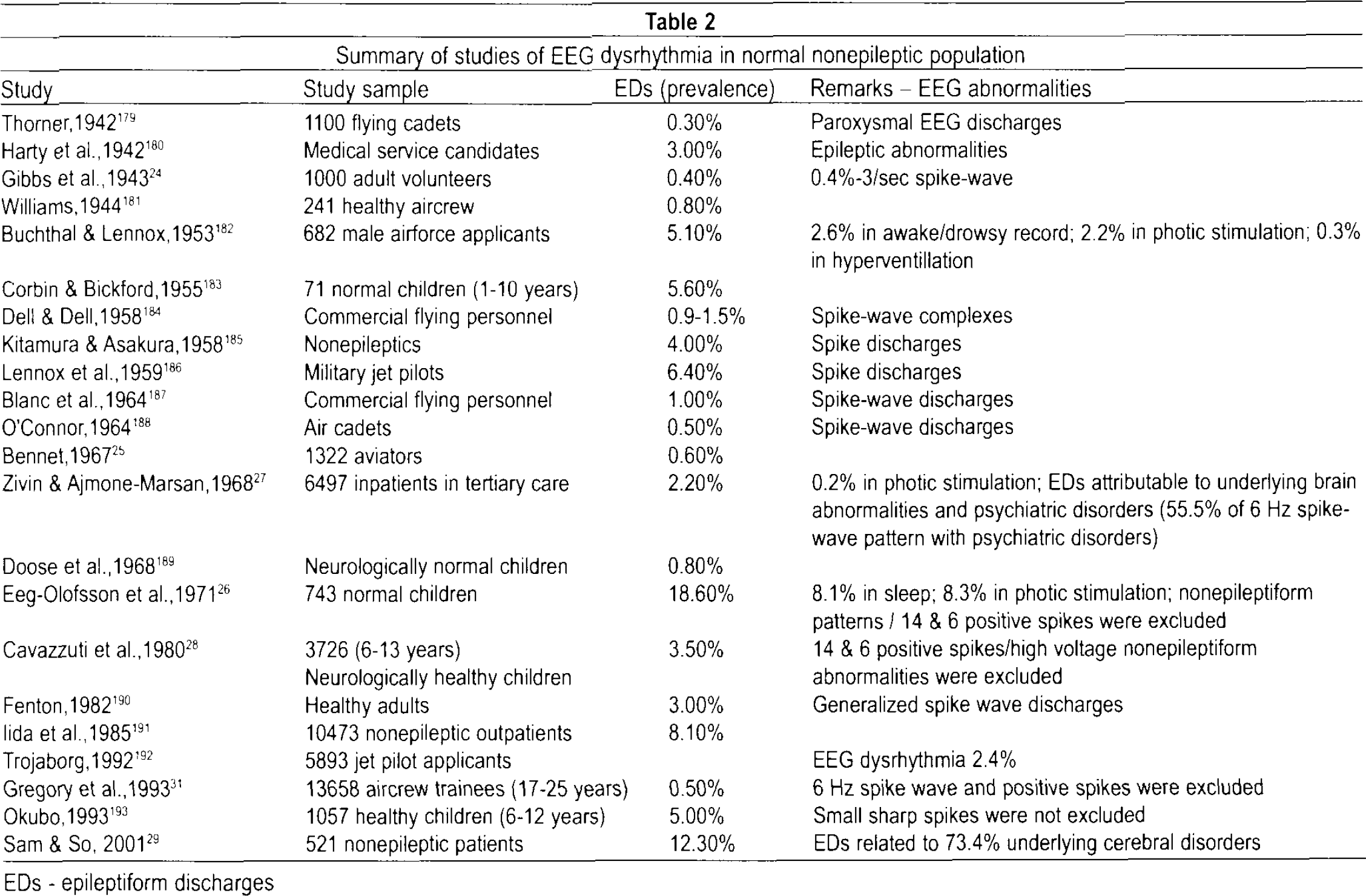
EDs - epileptiform discharges
Causes for the inadequacy of normative data concerning the prevalence of EEG dysrhythmia in nonepileptic general population
The low estimates presented in the studies of Gibbs et al. (1943) 24 (0.4%), and Bennet (1967) 25 (0.6%) employed minimum EEG requirements, where only three head regions were examined, without a sleep record, and for a limited duration of 10–15 minutes. Furthermore, Bennett's study focussed on only spike-wave abnormalities and the noninclusion of other IEA accounted for the relatively low rates of epileptiform discharges (EDs). Eeg-Olofsson et al. (1971) 26 reported a high prevalence of EDs as they considered all the EEG dysrhythmia in children during wakefulness, in addition to sleep, photic stimulation, hyperventilation, and also included non-epileptiform activities.
In the study by Zivin and Ajmone-Marsan, 27 factors that were incriminated in high prevalence estimates were the inclusion of individuals with a psychiatric history, and/or a history of significant head trauma. In this series of 6,497 nonepileptic subjects, the prevalence of epileptiform discharges was 2.2% with careful definition of EDs, complete recording, and sleep tracings. In this nonepileptic group, EDs were attributable to underlying brain abnormalities (traumatic-congenital and perinatally acquired brain damage, cranial operations; vascular; neoplasms; biochemical and metabolic disorders), medications, mental retardation and psychiatric disorders. The prevalence of EDs in this group was reported as 5.5% in those with mental handicap, 9.8% with congenital or perinatal brain insults, 10.6% after cranial operations and 8.2% in individuals with cerebral tumors. The risk of subsequent epilepsy in this study was reported to be as high as 14.1% due to the inclusion of individuals with histories of underlying brain abnormalities. Cavazzutti et al. 28 reported the prevalence rate of EDs to be 3.54% from 3726 children from 6 to 13 years of age without evidence of seizures or neurological deficits. A genetic predisposition, neurodevelopmental or environmental factors were postulated to be responsible for the expression of EEG abnormalities in this study even in the absence of a history of neurological insults or neurological deficit.
In a community study by Sam and So, 29 the prevalence of EDs was reported as 12.3%, but 73.4% of the nonepileptic patients had underlying cerebral disorders. The study was well designed using stringent criteria for the techniques of the EEG recording procedure; utilization of the Mayo system of EEG classification with exclusion of benign variants; exclusion of patients who had a history of unprovoked seizure occurrence, and patients with history of acute symptomatic or provoked seizures before the index EEG. This finding emphasized that the presence of EDs in subjects without epilepsy should be inferred as “electrographic markers” of underlying brain dysfunction without the vulnerability to clinical seizures. These abnormal neuronal discharges most closely associated with seizures, do occur in people who do not have epilepsy (subclinical EDs), but most have been linked to underlying cerebral disorder.
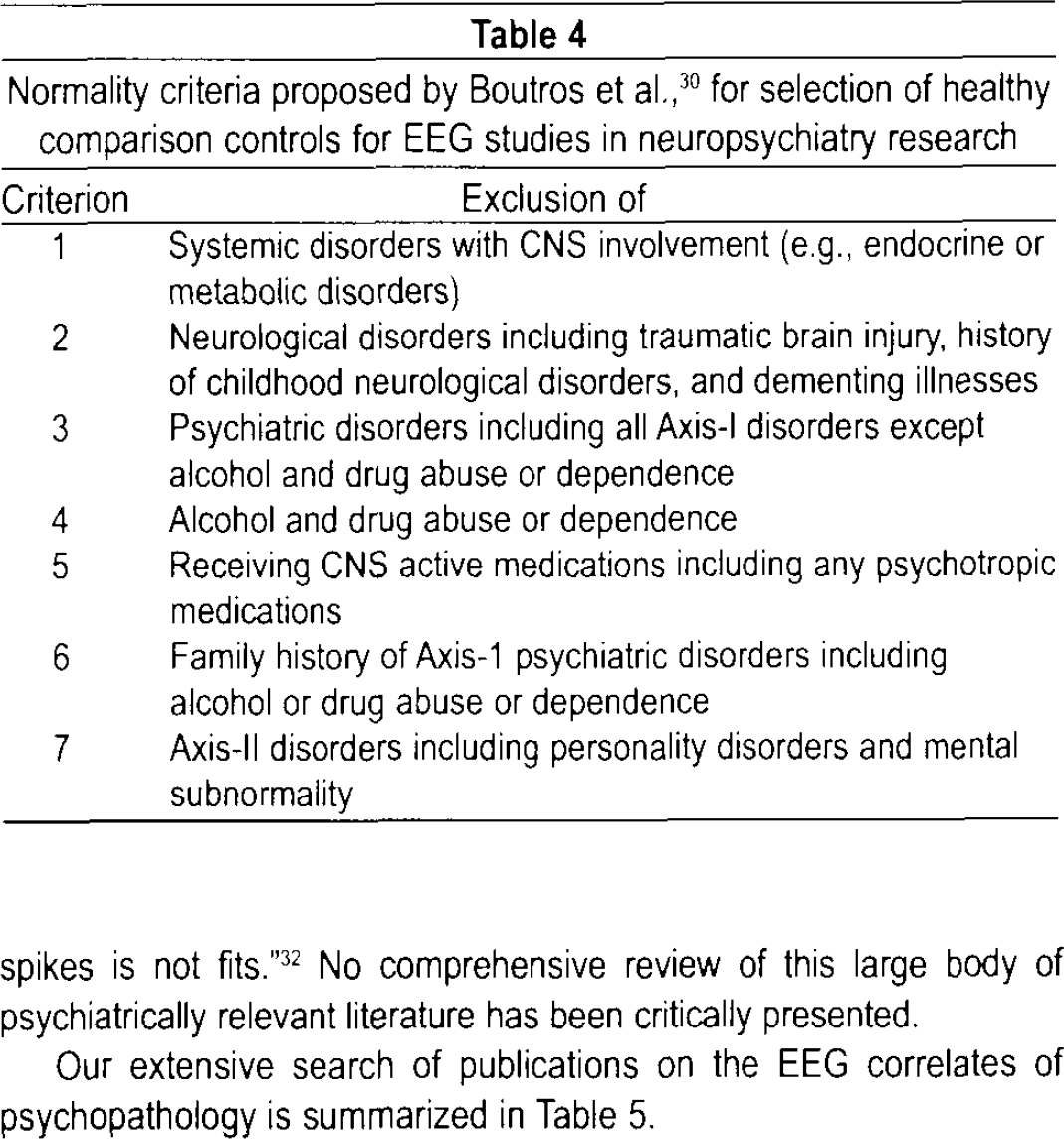
Another crucial source for the wide range prevalence of EEG abnormalities in the nonepileptic normal adult population is the lack of rigorous selection criteria for choosing the normal healthy control comparison subjects. In order to clearly define the boundaries of the normative EEG that is critical to derive valid generalizations for consensus opinion on the electroencephalographic correlates of neuropsychiatric disorders, Boutros et al. (2005) 30 proposed a seven point normality criterion for selecting healthy comparison subjects that is shown in Table 4. In their literature search from 1936 to 2005, a total of 38 articles examining the EEG of “normal” individuals were included, out of which about 60% of studies did not fulfil any of the proposed normality criteria. The EEGs of large samples of well characterized healthy individuals, meeting the criteria specified in Table 2, suggest the need for new research to provide more clearly defined boundaries of normality and to establish more uniform criteria for abnormality.
Normality criteria proposed by Boutros et al., 30 for selection of healthy comparison controls for EEG studies in neuropsychiatry research
After excluding contaminating factors, the true prevalence of EDs in a healthy normal population should be extremely low. The current estimate of EEG epileptiform dysrhythmia in the nonepileptic healthy population would be less than 1%, as supported by the work of Gregory et al. (1993). 31
IEA/CEREBRAL DYSRHYTHMIA IN NEUROPSYCHIATRIC DISORDERS WITHOUT CLINICAL SEIZURES
Numerous reports of EEG abnormalities in neuropsychiatric disorders exist in literature spanning the last six decades and this attests to the robustness of conventional EEG studies and their clinical utility in disorders at the brain-mind interface. Dysrhythmic EEG aberrations associated with various neuropsychiatric disorders do emphasize that these electrophysiological events go beyond epilepsy, and that “all that spikes is not fits.” 32 No comprehensive review of this large body of psychiatrically relevant literature has been critically presented.
Our extensive search of publications on the EEG correlates of psychopathology is summarized in Table 5.
Summary of studies of EEG cerebral dysrhythmia in neuropsychiatric disorders without clinical seizures
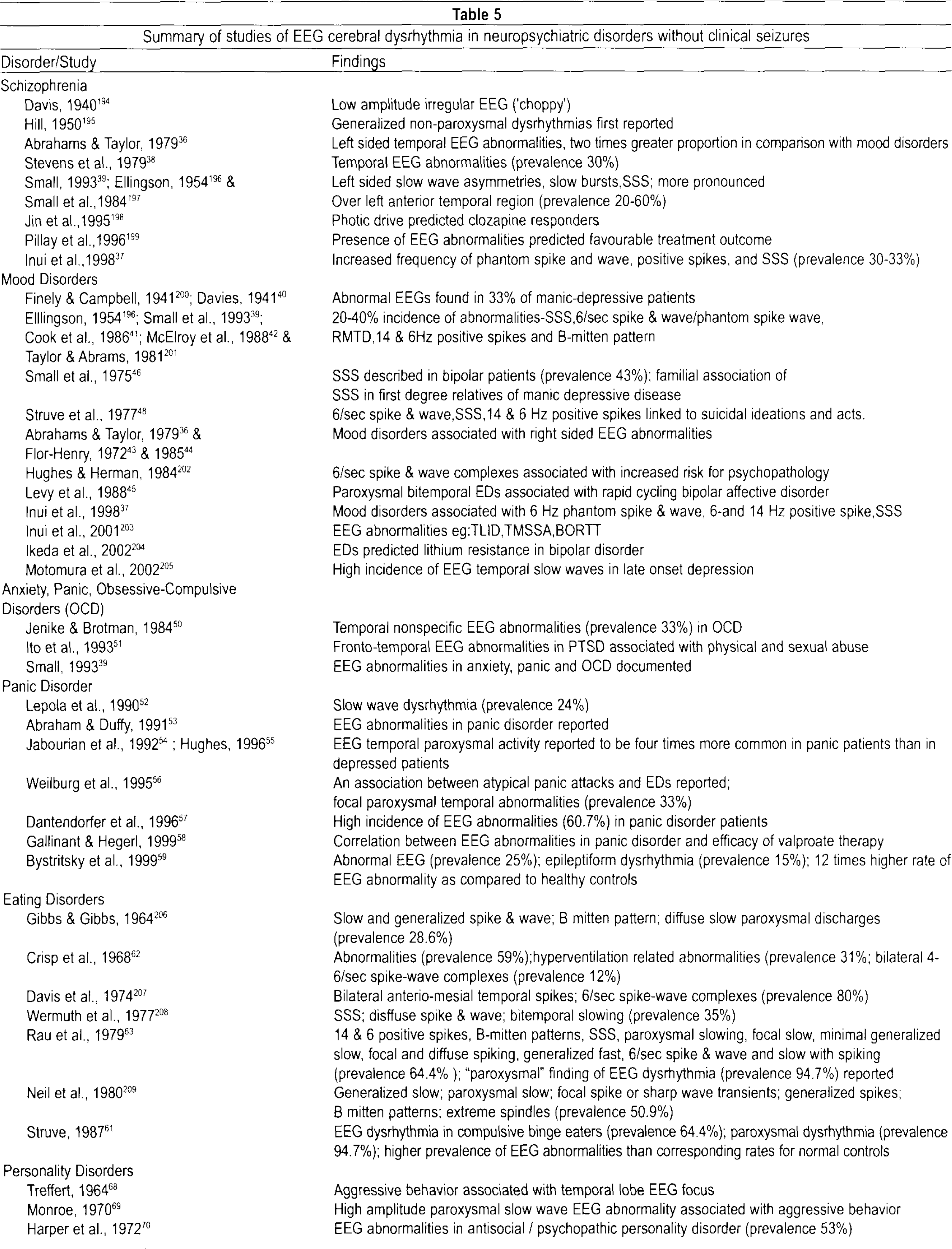

SSS-small sharp spikes; TLID-temporal low voltage, irregualr delta wave; TMSSA-temporal minor slow and sharp activity; BORTT-bursts of rhythmical temporal theta; RMTD-rhythmic midtemporal theta of drowsiness; PTSD-post-traumatic stress disorder; MMPI-Minnesota multiphasic personality inventory
The occurrence of epileptiform dysrhythmic abnormalities in a nonepileptic psychiatric hospital population had been reported by Bridgers (1987), 33 who studied the results of 3225 inpatients undergoing EEG examination from a general hospital psychiatric service during an eleven and a half year period. After the exclusion of patients with a prior diagnosis of epilepsy, epileptiform EEG abnormalities were documented in 2.6% of cases, and consisted of photoparoxysmal responses, focal temporal complexes, generalized spike-wave or polyspike- wave discharges, and focal central/frontal complexes. The likelihood of IEA was observed in younger patients (age <25 years) and in those patients on major tranquilizers, antidepressants, or lithium. Such IEA were found to correlate with diagnostic impressions of anorexia nervosa (21.1% IEA for patients on drug treatment; 6.9% for drug-naïve patients), depression (2.9% IEA for patients on drug treatment; 0.6% for drug-naïve patients), mania (3.7% IEA for patients on drug treatment; 0% for drug-naïve patients), schizophrenia (2.7% IEA for patients on drug treatment; 1.7% for drug-naïve patients), personality disorders, suicidal patients without depression, recent barbiturate abuse, non-psychotic explosive behavior, and effects of psychotropic medications such as major tranquilizers (4% IEA), antidepressants (7.7% IEA), and lithium (3.9% IEA). The results of the study of Bridgers not only confirmed the occurrence of IEA in nonepileptic psychiatric population but emphasized the role of underlying cerebral dysfunction without necessarily indicating a susceptibility to clinical seizures.
The following section will briefly review the dysrhythmic EEG aberrations that have been reported to be associated with some of the major neuropsychiatric disorders.
Schizophrenia
Since the pioneering work of Hans Berger, much of his original research involved schizophrenic and other serious psychiatric disorders. The earliest treatise on the EEG study of psychopathic behavior and schizophrenia was by Denis Hill and Geoffrey Parr (1950), 34 and the interested reader is referred to the historical compilation on “EEG and Behaviour” by Gilbert H. Glaser (1963) 35 that was based on a research conference on “Electroencephalographic Correlates of Behaviour” held at Yale University School of Medicine in November 1961.
Numerous studies have documented conventional EEG abnormalities in 20% to 60% of schizophrenics. Abrahams and Taylor (1979) 36 showed that schizophrenic patients had almost twice as many left-sided temporal abnormalities than patients with affective disorders, who were observed to have more right-sided EEG findings. Many of the EEG abnormalities documented in schizophrenia were minor, nonspecific, and conjectural. This included left-sided slow wave asymmetries, especially at the left anterior temporal area and occasionally involving the left frontal and parietal areas, slow bursts, and spikes or sharp waves. Telemetric EEG abnormalities in the temporal lobe have been reported to occur in 30% of schizophrenic patients. Schizophrenic patients with EEG abnormalities that appeared either before or during neuroleptic treatment had more evidence of brain dysfunction than did patients without such EEG abnormalities. Clozapine responders were found to demonstrate increased EEG abnormalities when compared to “nonresponders.”
EEG abnormalities were more frequent in the cohort of schizophrenic patients who had a positive family history of schizophrenia. These EEG aberrations may have reflected abnormalities in cortical neuronal architecture, cellular neuropathology, and neurochemical transmitter abnormalities that underpin the schizophrenia pathophysiology, in addition to possible neuroleptic medication effects. These EEG aberrations, along with neuroimaging and neuropsychological abnormalities, lend objective evidence for the brain dysfunction in genesis schizophrenia. Psychotic mood disorders and “atypical” psychoses have been reported to have a higher frequency of epileptiform variants, including the phantom spike and wave, positive spikes, and small sharp spikes. 37
Mood disorders
The incidence of abnormal conventional EEG findings in mood disorders appears to be substantial, ranging from 20 to 40%. 38 –42 These abnormalities were found to be higher in (a) manic than depressed patients, (b) female than male bipolar patients, and (c) nonfamilial cases with late-age onset disorder. Specific patterns noted in mood-disorders include: (a) small sharp spikes (SSS), (b) 6/sec spike and wave complexes (RMTD), (c) B-mitten pattern, and (d) positive spikes. Abrahams and Taylor (1979) 36 and Flor-Henry 43,44 have reported mood disorders to show predominantly right-sided EEG abnormalities, in contrast to the left temporal EEG abnormalities in schizophrenia. Furthermore, a few reports have demonstrated that rapid cycling bipolar affective disorder patients have more prevalent EEG evidence of bitemporal epileptiform paroxysmal activities than patients with non-rapid cycling mood disorders. 45 In patients with bipolar affective disorder, 43% have been shown to reveal small sharp spikes, which may be significantly related to a family history. 46
Suicide
Several studies have suggested links between EEG abnormalities and suicidality. Small sharp spikes, have been associated not only with affective disorders, but with a tendency to suicide. The study by Small, 1970 47 and Struve et al., 1977 48 reported a highly significant positive relationship between paroxysmal EEG abnormalities and suicidal ideation and acts, which were unrelated to medication. They identified rhythmic mid temporal discharges (RMTD), 6/sec spike waves, and small sharp spikes (SSS) to be associated with suicidality. Struve (1985) 49 also observed that patients with EEG dysrhythmias taking oral contraceptives have a significantly higher incidence of suicidal behavior than did women with normal EEGs.
Anxiety, Panic, Obsessive-Compulsive disorders
Several studies have suggested a high incidence of EEG abnormalities in patients with anxiety disorders, panic disorders, and obsessive-compulsive disorders. 50 –59
Of the neuropsychiatric symptoms most confused with epileptic seizures, panic attacks and rage attacks are the most frequent. Panic symptoms have a significant resemblance to symptoms induced by temporo-limbic epileptic activity. The phenomenology of panic attacks and of complex partial seizures overlap, and at times distinguishing between the two entities is difficult. Further since panic attacks and dissociative phenomena like fugue states have some similarities to temporal complex partial seizures, it is imperative to rule out the possibility of an epileptic origin to these conditions before an alternative diagnosis may be confidently established. 60
Hughes (1996) 55 reported that EEG paroxysmal dysrhythmia was four times more common in panic patients than in depressed patients. Our literature review indicated that about 25–30% of panic attack patients have demonstrable EEG abnormalities, especially in atypical presentations of panic attacks. Some studies have documented an epileptic pathophysiology that underlies some atypical panic attacks. 56
Weilburg et al. (1995) 56 reported focal temporal paroxysmal EEG changes in 33% of patients during actual panic attacks using prolonged ambulatory EEG monitoring, and 40% of these patients with panic-related EEG changes had a normal routine EEG. They stressed the need for EEG monitoring during multiple attacks to reveal any association between atypical panic attacks and epileptiform EEG changes. Dantendorfer et al. (1996) 57 reported an increased incidence of EEG abnormalities in panic disorder patients in addition to MRI structural abnormalities in septo-hippocampal regions. They reported 60.7% of such patients with EEG abnormalities to have MRI abnormalities as compared to patients without EEG abnormalities (17.9%) and healthy controls (3.6%). In this study complete remission of symptoms was obtained only with a combination therapy of carbamazepine and clonazepam. Other studies include that of Gallinant and Hegerl (1999) 58 who emphasized the positive response of panic attack patients to valproate therapy whose detailed work up revealed EEG abnormalities.
Antiepileptic drug trials may be warranted in those patients with atypical panic attacks with abnormal EEGs. However, there are no studies and only large well-controlled studies will answer the question whether antiepileptic treatment should be a first line of treatment in abnormal EEG/panic disorder subjects.
Eating disorders
Disorders of eating behavior and its EEG correlates have been attributed to the scholarly work of Struve (1987) 61 in his paper titled “Clinical EEG correlates of Anorexia and Bulimia: Historical review and current findings.” The study of Crisp et al., (1968), 62 in 32 subjects with anorexia nervosa reported an abnormal EEG background in 59% with 31% showing unstable responses to hyperventilation and 12% had paroxysmal abnormalities (bilateral 4–6/sec spike-wave complexes) which were attributed to the often profound metabolic and neuroendocrinological alterations seen in severe anorexics. 62
Rau et al., (1979), 63 had studied the prevalence and type of EEG dysrhythmias among compulsive binge eaters with those obtained with normal controls and several independent samples of unselected and selected psychiatric patients. The prevalence of abnormal EEG was 64.4% and included abnormalities such as 14 & 6 positive spikes, mitten patterns, small sharp spikes, paroxysmal slowing, focal slow, minimal generalized slow, focal and diffuse spiking, generalized fast, 6/sec spike and wave and slow with spiking. Amongst these patients with abnormal EEGs, 94.7% displayed a “paroxysmal” finding of EEG dysrhythmia.
Andy and Jurko, (1972), 64 using depth electrode study confirmed that the 14 & 6 positive spike pattern in anorexics was subcortical and thalamic in origin.
Thus, our literature review (Table 5) suggests that anorexia nervosa and other eating disorders have been documented to have the highest prevalence of EEG dysrhythmia. The co-occurrence of EEG abnormalities consisting of B-Mitten and small sharp spike (SSS) dysrhythmic patterns reflect the cross relationships between anorexia nervosa, depressive disorder and suicidality. These findings may be related to dietary factors, neuroendocrine and nutritional deficiencies that would undoubtedly cause cerebral metabolic aberrations contributing to brain dysfunction.
Personality disorders and criminal behavior
The studies of Hill, (1952) 65 ; Williams, (1969) 66 ; Stafford-Clarke and Taylor, (1949) 67 have described high incidence of abnormal EEGs in aggressive psychopaths, criminals and motiveless murderers.
Many previous EEG findings on personality disorders, forensic populations, violence and criminal behavior have been found to suffer from methodological problems. The EEG data were thus considered nonspecific as the results could not always be replicated by all investigators. Therefore, the significance of these EEG abnormalities is still a matter of debate. From our literature review, the abnormal EEG findings that were documented to occur in personality disorders, criminal behavior and borderline personality disorder have been summarized in Table 5. 65,66,68 –96 One of the interesting findings in earlier studies was that relatively good personality structure relates to a normal EEG. 66 The initial studies did reveal positive trends in relating EEG dysrhythmic abnormalities to personality traits, and a psychopathic MMPI profile. 66,77,96 These EEG aberrations in personality and impulsive behavior reflect the presence of cerebral dysfunction that may hamper the natural process of psychological maturation.
Hill and Watterson (1942) 77 were the first to postulate that EEG dysrhythmia in aggressive psychopaths reflected a failure in functional cortical development (maturational retardation hypothesis). Although some evidence supports the maturational retardation hypothesis, 97,98 the finding that many aggressive psychopaths had normal EEGs argued against it. Other studies, however, failed to find a relationship between EEG abnormalities and aggressive tendencies. 99 –102 Carvalhal Ribas et al. (1974), 103 on the other hand, found evidence of cerebral dysrhythmia in 69% of youngsters with behavior disorders with predominance of aggressiveness. Earlier literature did link criminal behavior, and aggression to an “epileptic etiology.” However, there is lack of convincing current evidence for such a proposition of an association between violence and epileptiform EEG disturbances. 72
Antisocial and criminal populations studied had EEG abnormalities in 24% to 78% of individuals. These EEG abnormalities were found to be more prevalent in subjects with violent crimes, repeated violence, and motiveless crimes. No specific relationship had been found between the type of EEG abnormality and characteristics of the crime, or between EEG changes and the degree of violence committed. 85,86 Several types of EEG abnormalities had been found in violent offenders: generalized slowing, focal slowing, and EDs. A few studies summarized in Table 5 have established violent behavior to be linked to left-sided temporal lateralization of EEG abnormalities. 84,85 These EEG aberrations suggest underlying brain dysfunction in violent behavior. 104 The validity of these EEG aberrations had also been confirmed by some quantitative EEG studies, 105 and neuropsychological data. 106 Quantitative EEG data, neuropsychological data, and other EEG studies lend support to the concept of a connection between left hemispheric (frontal, temporal) cerebral dysfunction and the propensity for violence. 85,105,106 The presence of EEG dysrhythmia, instead of having any specific associations with criminal behavior, may actually represent underlying comorbid factors such as multiple head injuries, coexisting substance abuse, and associated toxic and metabolic disorders.
Currently, an increasing body of knowledge from brain imaging research has implicated brain abnormalities in the etiology of psychopathic and antisocial behavior. Functional brain imaging techniques such as fMRI and PET will certainly be tools to further explore the existing relationship between the EEG and deviant personality traits.
In borderline personality disorder (BPD), literature has suggested two types of conventional EEG abnormalities (i) epileptiform dysrhythmia, and (ii) diffuse EEG slowing. The presence of EDs in BPD possibly indicated cortical excitability disturbances that may be predictive of responsiveness to anticonvulsant therapy, 86 whereas diffuse EEG slowing possibly reflected underlying metabolic or degenerative etiologies. Boutros et al, 2003 107 reviewed the literature during the period 1966 to 2000 on the electrophysiological aberrations in BPD. It was found, that the EEG investigations of the BPD were limited as only nine articles could be evaluated. Furthermore, the majority did not have adequate control groups, adequate evaluation of Axis I or Axis II comorbidity, and controls for medication effects.
Psychogenic nonepileptic seizure disorders
Psychogenic nonepileptic seizures (PNES) are another area in the psychiatric EEG literature that merits a reappraisal. The incidence of this disorder approximates 5–20% in epileptic outpatients, and represents 20–30% of adults with “refractory” seizures contributing to 10–40% of inpatient admissions to EEG monitoring units at tertiary referral centres. To further complicate the clinical scenario, the coincidence of PNES with epilepsy ranges from 3.6% to 58%. 108 This re-emphasises the need to recognize studies that investigated and reported on the occurrence of EEG epileptiform abnormalities in PNES since their detection in the interictal EEG may cause diagnostic problems in diagnosis of PNES. 109
In our review of literature, the only study that specifically focussed on the prevalence of IEA in PNES was that of Reuber et al. (2002). 110 Other studies related to PNES have been summarized in Table 5, and relevant data extracted from these articles pointed to a mean prevalence of interictal EEG abnormalities in PNES to be estimated at 25.9%. 111 –119
The incidence of paroxysmal nonepileptiform dysrhythmia has been reported by several workers: 20%-25% (King et al. 1982 112 and Luther et al. 1982) 113 ; 40% (Standage 1975) 111 ; 44% (Wilkus et al. 1984) 115 ; 37% (Cohen and Suter. 1982) 114 ; and 8%-37% (Bowman 1993). 118 Most of the paroxysmal dysrhythmic EEG patterns reported by these studies included (a) abnormal temporal theta (unilateral or bilateral), sometimes with sharp components, and (b) paroxysmal temporal slow waves accompanied by abnormalities in background activity. Truly epileptiform spikes or spike-wave discharges and temporal lobe spikes have been reported in 12% of PNES by Cohen and Suter. Lelliott (1991) 117 reported 74% incidence of EEG abnormalities in PNES which comprised of temporal lobe spikes, spikes elsewhere, temporal slow waves, paroxysmal slow waves and abnormalities in background activity. Various investigators have implicated the association of brain abnormalities and antecedent head injury in the genesis of PNES, both of which could contribute to EEG abnormalities.
In Reuber's study, 110 the rates of abnormal nonspecific, and epileptiform EEG abnormalities in PNES were documented to be 53.8% and 12.3% respectively. When PNES was compared with an appropriately selected control group, nonspecific EEG abnormalities were seen 1.8 times as often in PNES as in healthy controls. Such EEG abnormalities may be attributed to the complex interaction of (i) comorbid psychiatric disorders and various psychopathological variables, (ii) underlying brain abnormalities, (iii) head trauma, 120 –122 and (iv) physical and sexual abuse, which plays a pivotal role in the final clinical expression of PNES vulnerability. It is imperative to be cognizant of the fact that EEG dysrhythmias do occur in PNES, and it is crucial to understand that the mere presence of paroxysmal EEG dysrhythmia in PNES should not be rapidly concretized to an epileptic connotation, and to avoid the misdiagnosis as epilepsy.
Psychotropic drugs
The heterogeneity of conventional EEG abnormalities in schizophrenia and mood disorders can in part be attributed to medication effects. However, most of studies that we have reviewed here had comprised of unmedicated subjects, at the same time, several studies had not discerned the effects of psychotropic medications on EEG. The few studies that addressed the relative contribution of drug treatments in neuropsychiatric disorders to EEG aberrations are discussed below.
In studies antedating widespread use of modern atypical antipsychotic agents, Stevens et al., (1979), 38 reported about 30% of hospitalized psychotic patients had EEG abnormalities over temporal lobes and Bridgers et al., (1987), 33 detected epileptiform EEG abnormalities in about 2.6% of cases. Major tranquilizers, antidepressants, and lithium have been reported to be associated with a variable propensity to induce both clinical seizures and EEG epileptiform abnormalities by Itil et al., (1982) 123 ; Betts et al., (1968) 124 and Itil, (1971) 125 respectively.
EEG abnormalities have been reported in nearly 65% of patients treated with lithium inducing high voltage anterior delta activity and 17% risk of IEA. 126 When combined with haloperidol an increase in paroxysmal EEG abnormalities has been reported. Thus, the use of lithium in bipolar disorders may have contributed to the association found that is found between EEG abnormalities and bipolar disorders.
Hughes, (1996), 55 reviewed the EEG abnormalities associated with the prescription of psychotropic agents. Chlorpromazine induces clusters of slow dysrhythmic waves, in the form of a slowed alpha frequency and an increase in theta and delta rhythms, sharp waves, or spikes and slow-wave discharges that may antedate overt epileptic seizures. With tricyclic antidepressants, an increase in slow activity is seen in addition to an increase in fast beta rhythms. Lithium is reported to induce slow wave dysrhythmia as an increase in theta and an early decrease in alpha frequency.
Given the limited knowledge of EEG abnormalities (dysrhythmias and IEA) among patients treated with modern antipsychotics, Centorrino et al., (2002), 127 studied the risk factors for EEG abnormalities, and dose-dependent risk for epileptic seizures of various antipsychotic drugs from the EEG recordings of 323 (293 belonged to the treated group, 30 who did not receive antipsychotic drugs) hospitalized psychiatric patients. In this study, a strict EEG assessment protocol with considerations on EEG rating reliability and EEG scoring for abnormalities were emphasized. They reported EEG abnormalities in 19.1% of the antipsychotic treated group with 13.3% in the untreated group. EEG spike discharges or spike-and-wave activity were associated, in order of risk, with thiothixene, trifluoperazine, olanzapine, chlorpromazine, clozapine, combination antipsychotic therapy, risperidone, and perphenazine.
Among antipsychotics considered atypical the risk of EEG abnormalities were 47.1% for clozapine, 38.5% for olanzapine, 28.0% for risperidone and 0% for quetiapine. Co-morbid risk factors significantly and independently associated with EEG abnormalities included hypertension, older age, and a diagnosis of bipolar disorder, whereas co-treatment with a benzodiazepine was a protective factor. Freudenreich et al., (1997), 128 postulated that seizure risk with clozapine probably increases with drug dose and serum concentration. These data support the view that EEG abnormalities can be a direct drug effect rather than to an underlying organic cerebral disorder.
Another recent study by Amann et al., (2003) 129 looked into the EEG abnormalities associated with the use of atypical antipsychotics quetiapine and olanzapine, and the typical antipsychotic haloperidol in a retrospective analysis in 81 patients under stable monotherapy compared with an age and sex matched control group. Abnormal EEGs were more frequent in the olanzapine and haloperidol groups, whereas epileptiform activity was seen in only the olanzapine group. It was concluded that EEG abnormalities seem to occur rarely in patients treated with quetiapine comparable to the control group, but significantly more often with haloperidol and olanzapine, possibly due to different receptor profiles of these substances.
EEG studies need to be done in drug naïve as well as during psychotropic drug treatment so as not to misattribute an EEG abnormality to the underlying disorder rather than to the drug effect. Whether the appearance of specific EEG aberrations in various neuropsychiatric disorders help identify a subgroup of patients within the same DSM construct most likely to benefit from treatment (pharmaco-EEG) is not fully established and awaits well designed controlled studies. Pharmaco-EEG is a potential application in the future that will provide sensitive methods to monitor psychotropic drug therapy, and would have a role in the prediction of clinical response to treatment with psychotropic drugs. 130
IEA/CEREBRAL DYSRHYTHMIA IN CHILDHOOD NEUROBEHAVIORAL DISORDERS WITHOUT CLINICAL SEIZURES
Common neurobehavioral disorders of childhood include autistic spectrum disorders (autism, pervasive developmental disorder not otherwise specified, Asperger's syndrome, Rett's syndrome, and disintegrative disorder), and attention deficit disorders with or without hyperactivity (ADHD or ADD). Autistic spectrum disorders (ASD), Landau-Kleffner syndrome (LKS), electrical status in slow wave sleep (ESES), developmental dysphasia, and benign rolandic epilepsy (BRE) have overlapping features, and from our review, the high incidence of epilepsy and/or subclinical or infraclinical IEA does seem to be the interesting common thread that exists among these conditions (Figure 1).
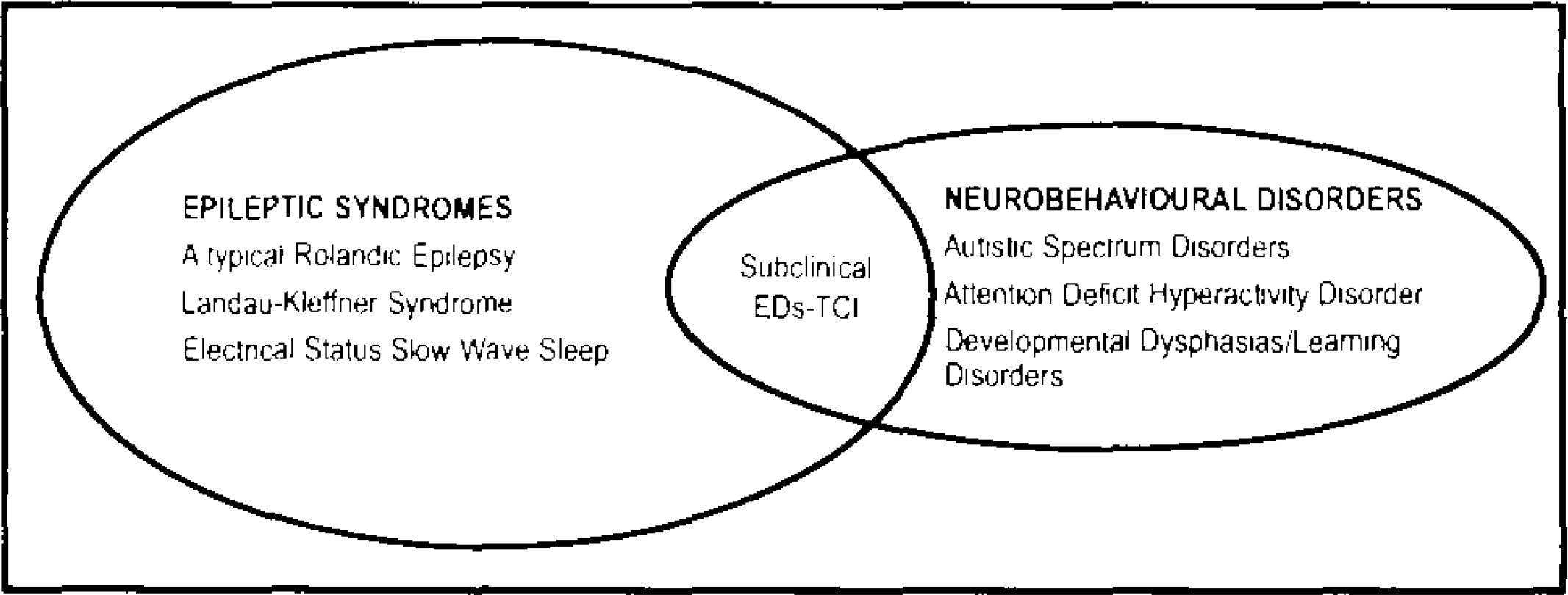
Figure depicting an overlap between certain epileptic syndromes and neurobehavioral disorders linked by the common EEG expression of subclinical epileptiform discharges (EDs) (TCI- Transitory cognitive impairment).
Benign focal childhood epilepsy, LKS, and electrical status epilepticus in sleep are best considered as a spectrum of disorders with a common transient, age dependent, nonlesional, genetically based epileptogenic abnormality. The electro-clinical features of these syndromes are congruent with the different degree involvement of the perisylvian cognitive network and with variable degree of involvement of the thalamo-cortical associative system. These epileptic syndromes are characterized by the occurrence of rare overt seizures, abundant regional interictal epileptiform discharges and epileptogenic cognitive impairments. The nature and severity of interictal cognitive symptoms are closely related to localization within the network and amount of epileptic interictal discharges. Spike-wave discharges are attributed to an alternation of overexcitation (spikes) and overinhibition (waves). The recurrent overinhibition represented by the wave of the discharges interferes with the continuous depolarization of the cells of a large population of neurons, which is a requirement of the overt seizures. The overinhibition also interferes with cognitive processes which are correlated with the continuous presence of the fast (gamma) activity, binding the required cortical areas. Thus these focal IEA interfere with cognitive development (“cognitive epilepsies”), and EEG-triggered fMRI, which is interictal, and equivalent current dipole (ECD) analysis of MEG should be useful investigative tools for observations between the location of spikes and their behavioral-cognitive sequelae.
The studies that have linked the various pediatric neurobehavioral disorders without overt clinical seizures to EEG abnormalities have been summarized in Table 6. 131 –157
Summary of studies of EEG cerebral dysrhythmia in childhood neurobehavioral disorders without clinical seizures
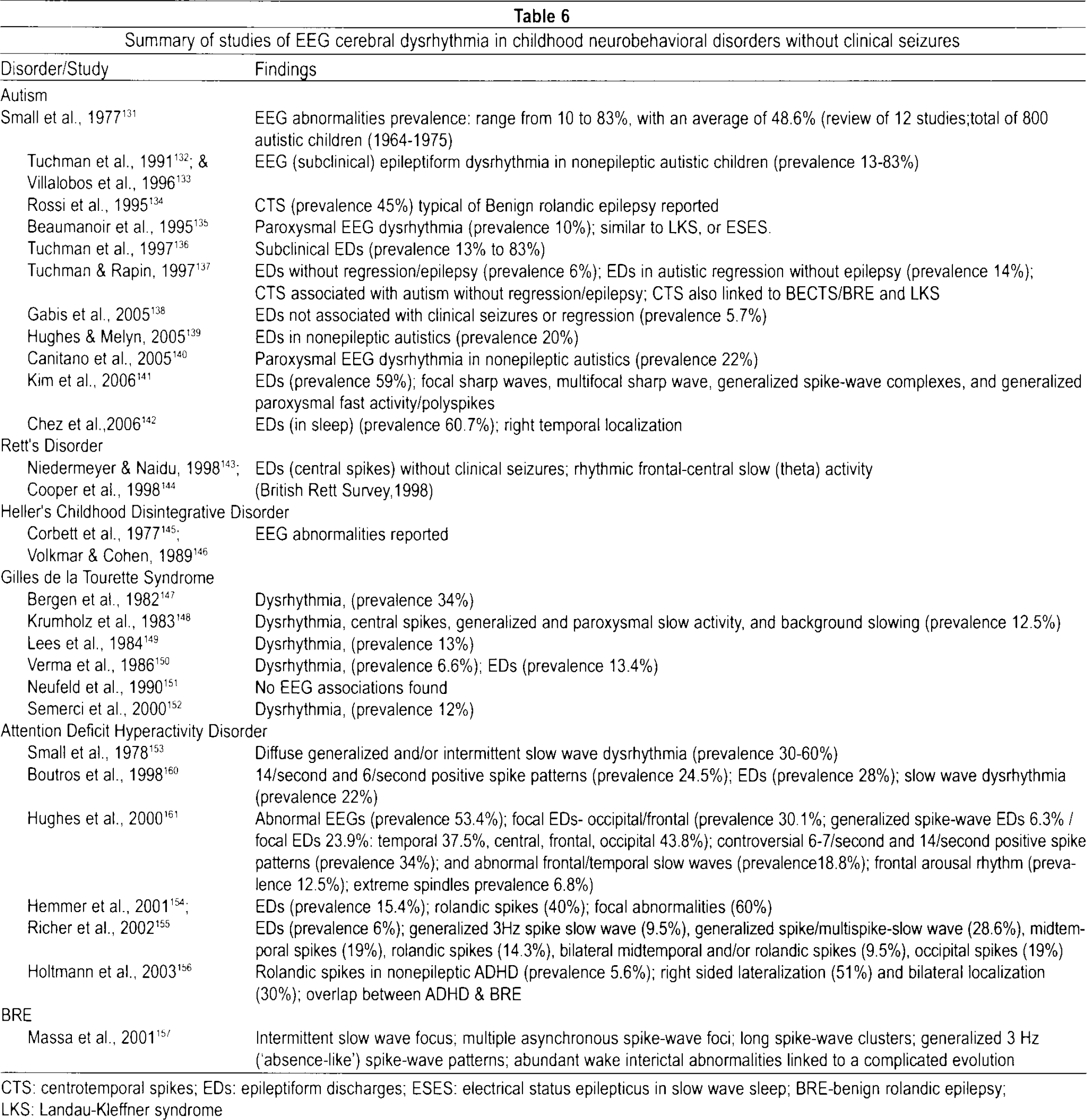
CTS: centrotemporal spikes; EDs: epileptiform discharges; ESES: electrical status epilepticus in slow wave sleep; BRE-benign rolandic epilepsy; LKS: Landau-Kleffner syndrome
Several studies have reported conventional EEG abnormalities in 30 to 60% of children with ADHD or with specific developmental learning disorders (SDLD). 158,159 Seizures have been reported to occur in 10–15% of children with PDD and 8 to 10% have epileptiform EEG abnormalities without clinical seizures.
Several studies summarized in Table 6 have documented positive correlations between subclinical paroxysmal EEG dysrhythmia in nonepileptic autism 132,133,136 –142 and nonepileptic ADHD 154,155,160,161 and also brought to light, the clinical overlap between nonepileptic ADHD and typical BRE as evidenced by the increased frequency of EEG subclinical rolandic spikes. 156 ASD and LKS have been documented to have a neurobiological overlap of perisylvian epileptiform discharges using MEG, and suggested antiepileptic therapy to ameliorate the IEA may lead to an improvement in autistic features. 162
Autism
Autism is associated with a high frequency of epileptiform EEG abnormalities (prevalence range 10.3–72.4%) and epilepsy (prevalence range 0–44.5%). A significant subgroup of autistic children (20–49%) experience autistic regression. The relationship among EEG abnormalities, epilepsy, and regression in autistic patients is not yet well understood.
The earliest study on autism contributed by Small et al. (1977) 131 from 14 pooled studies reported a wide range of prevalence of EEG dysrhythmia. This large range undoubtedly arose from differences both in the populations under study and, more importantly, the diagnostic criteria used for the abnormality. Kim et al., 2006 141 reported 59% prevalence of interictal epileptiform EEG abnormalities that included focal sharp waves, multifocal sharp waves, generalized spike-wave complexes, and generalized paroxysmal fast activity/polyspikes in nonepileptic autistic children. These EEG dysrhythmias may represent an age-dependent epiphenomenon of impaired brain maturation, with cumulative effects of these EEG discharges contributing to cognitive abnormalities.
The study by Hughes et al. (2005) 139 has shown association between EEG abnormalities and autistic regression. They reported abnormal EEGs in 75% of patients, clinical seizures in 46%, EEG spike discharges in 59%, and significant slow waves (delta waves) in 54% of patients. Of patients with EEG spike discharges 20% did not express clinical seizures. Of the autistic children 21% showed bilateral generalized spike and wave complexes of a cortico-reticular type. The high incidence of slow wave abnormalities in this study clearly represents a brain neurophysiological disturbance that correlates well with changes reported in MRI and PET studies in autistic children. 163,164 In fact, the pathogenetic role of such abnormalities in autistic regression has been demonstrated by the clinical improvement of 71% of patients with antiepileptic drugs. 165
Despite controversies, it is believed that subclinical EEG epileptiform discharges are responsible for the regression of language and behavior in these disorders by disrupting the function and development of relevant neocortical systems. The debate in the neurobiology of these childhood neurobehavioral syndromes centers on the contributory role of epilepsy and/or subclinical epileptiform EEG activity to its causality. While several studies have speculated that regressive behavioral abnormalities in autism are linked to epileptiform EEG abnormalities even in the absence of overt clinical seizures and that elimination of the epileptiform activity should lead to improvement in behavior, other investigators have not been able to find such associations. However, there is no current evidence-based treatment recommendation to support such therapeutic effects on behavioral abnormalities in pervasive developmental disorder (PDD) and autism. 137,166,167
Atypical/Complicated BECTS/BRE
Recently, a few studies have challenged the axiom of benignity of EEG observations by demonstrating that children with BECTS/BRE do develop cognitive dysfunctions, behavioral problems, and learning disabilities. A complicated evolution in benign epilepsy with centrotemporal spikes (BECTS) /benign rolandic epilepsy (BRE) has been reported to occur in a proportion of BRE patients. This BRE subset developed behavioral, cognitive, and learning problems independent of their clinical seizures or treatment. The complicated evolutions were found to be correlated with certain interictal EEG variables: intermittent slow-wave focus, multiple asynchronous spike-wave foci, long spike-wave clusters, and generalized 3 Hz “absence-like” spike-wave discharges. 157 Complicated BRE does further implicate the role of subclinical intercital EEG discharges in the etiology of behavioral and cognitive problems unrelated to seizure characteristics. Thus, BRE does represent different entities amongst the subclasses of a broad continuum of brain maturation disorders ranging from typical to complicated evolution in idiopathic rolandic epilepsy. The controversies regarding the neurogenesis and functional organization of the interictal spikes in BECTS have recently been elucidated by a simultaneous EEG and MEG study. 168
Recent studies have documented the existence of language dysfunction in children with Rolandic epilepsy related to interictal dysfunction of perisylvian language areas. 169,170 and as already suggested above, BRE/BECTS have been linked with LKS and continuous spikes and waves during slow sleep (CSWS). BRE patients manifesting language disorders have been shown to strongly resemble LKS, which is characterized by continuous spikes and waves during slow wave sleep, acquired aphasia, and seizure disorder. 171,172
From these clinical overlaps (ASDs, PDD, ADHD, LKS and BRE), it maybe suggested that an interesting common thread exists among these conditions namely the high incidence of epilepsy and/or subclinical epileptiform EEG activity as shown in Figure 1.
The electrographic dysrhythmia in these pediatric neurobehavioral disorders may represent an epiphenomenon of cerebral dysfunction or underlying cortical morpho-functional abnormalities, and/or reflect a brain neurophysiological disorder which is not sufficient to be expressed as epilepsy. This may be due to the lack of properly functioning corticocortical fibers which restricts the spread of epileptiform activity from one brain area to another and prevent its evolution to a clinical seizure. The subclinical discharges in the developing maturing brain may also directly impair cognitive-behavioral functioning by way of “transient cognitive impairment” mechanisms, well described by Binnie and his colleagues. 9,18,19
Current consensus of AED treatment of subclinical IEA in behavioral outcomes in neurobehavioral disorders with/without clinical seizures
The clinical relevance of subclinical IEA that is reported in various studies in pediatric neurobehavioral disorders is unclear. It is generally agreed by neurologists and pediatricians that patients should be treated for epilepsy only if they have clinical seizures. Treating the EEG (EEG cosmetics) is generally condemned. However, the only way to determine whether these subclinical IEA cause cognitive-behavior sequelae is from studies that documented behavioral improvement when the subclinical IEA are suppressed by antiepileptic drug therapy.
In this regard, the studies summarized in Table 6 put forward arguments for an association between subclinical epileptiform discharges and neurobehavioral disorders as well as about its causality. Given the established link between EEG epileptiform abnormalities and neuropsychiatric symptoms in these overlapping disorders, EEG evaluation seems to be justified in children with cognitive and behavioral problems, even in the absence of overt clinical seizures. In this context, Engler et al. (2003) 173 had shown beneficial effects of sulthiame on EEG features, neuropsychological deficits, and speech deficits in seizure free children with rolandic spikes. Duane et al. (2004) 174 reported similar findings in their study demonstrating beneficial effects on cognitive, behavioral and EEG indices using levetiracetam in learning and attention problems. A randomized, double-blind controlled trial of lamotrigine in children with well controlled seizures and associated behavioral problems by Pressler et al. (2005) 22 did confirm the possibility of improving behavior by suppression of EEG interictal discharges. Another recent study, Chez et al., (2006) 142 reported a frequency of 60.7% abnormal EEG epileptiform activity in ASD patients with no known genetic conditions, brain malformations, prior medications, or clinical seizures. In the valproate treated group, 45% normalized on EEG and about 20% showed EEG improvement when compared with the first EEG.
There is a need for further research to explore and ascertain whether these electrophysiological aberrations are a cause, consequence, epiphenomenon or a coincidence. The clinical overlaps between autism, ADHD, BRE, LKS has received relatively little attention and future studies need to focus on this EEG-behavior relationship. There is also no current consensus on whether treatment of EEG abnormalities in these disorders does improve behavior. The benefit of antiepileptic pharmacotherapy for nonepileptic children with behavioral problems and EEG epileptic discharges must be clarified. 175 Randomized studies involving blinded pre- and post-treatment assessments of behavioral, cognitive, and neuropsychological domains as outcome measures will be needed to answer this question. Therefore from an evidence based research perspective, well designed larger studies with adequately selected control comparison group, adequate diagnostic construct, blinded EEG interpretations are needed in the future to re-evaluate and confirm the precise relationship of the behavioral/EEG equation.
At the end of this section, the maxim “treat the patient, not the EEG” may perhaps be an oversimplified clinical perspective, as evidence is mounting that in some of the disorders (ASD; ADHD associated subclinical rolandic epileptiform EEG discharges) with coincident subclinical epileptiform discharges might benefit from antiepileptic therapy even in the absence of overt clinical seizures.
DISCUSSION
Our recent work that critically and systematically reappraised the published electroencephalographic correlates of human behavior, from 1950 to 2005, has added new insights into future areas for brain-behavior-EEG research and neurobehavioral electrophysiology research. 176 From this large body of literature, we did confirm that there is a greater incidence of EEG abnormalities in neuropsychiatric population. However, the lack of valid generalizations for conventional EEG abnormalities in neuropsychiatric populations were due to methodological pitfalls, lack of controls, small sample size, differences in EEG interpretative criteria, by lack of definitive psychiatric diagnostic criteria applied, and by the inadequate selection criteria for a healthy EEG control comparison group.
The current review does reiterate that IEA seen in various nonepileptic neuropsychiatric disorders, to reflect unequivocal evidence of underlying brain dysfunction at the cortical, neuronal architectural level, as well as neurochemical perturbations that underpins several of these psychiatric pathophysiology and behavioral disorders. In addition, EEG abnormalities represent the phenotypic expression of cellular and biochemical dysfunction, and are also indicative of maturational retardation factors, possibly genetically determined, underlying subclinical earlier organic brain damage, neurotransmitter imbalance, or morpho-functional disturbances that may be aberrant in neuropsychiatric disorders.
Although the EEG has become a necessary clinical investigation in people with epilepsy, in practice it is much more useful in a telemetry situation whereby ictally related changes can be directly correlated with observed behavior changes. However, as our review shows, many patients who do not have overt epilepsy have EEG abnormalities, often epileptiform in nature. The importance of this cannot be over-emphasized, since it is one of the chief reasons why people with nonepileptic attacks (pseudoseizures) get diverted to an epilepsy clinic and mistreated.
Stevens (1977) 177 many years ago pointed out the truism that all that spikes is not fits, she pointed to the potential importance of EEG spikes, both in the awake but also particularly in sleep cycles, as physiological mechanisms of focal synchrony allowing rapid information of neuronal activity that may be linked to species survival. She also pointed out however, that such a mechanism carries a risk of the development of seizures if wide propagation occurs, hence the necessary surrounding inhibition of inhibitory neurotransmitters preventing such dissemination. To quote “the EEG spike, representing bursts of firing or synchronous polarization in closely proximate units, may thus represent a powerful mode of information transmission or amplification which is particularly associated with maturation and reproduction, including hormone release during sleep and response to changes in light, season and sexual activity.” These pertinent remarks remind us that the spikes, so readily referred to as epileptiform, may reflect disturbances of the propagation of information within the central nervous system which, depending on the time in the developmental life cycle that they occur, will lead to an alteration both of cerebral maturation, but also consequent cognitive and behavior difficulties, which are biologically closely associated with limbic activity.
The recent studies of Laufs et al. with fMRI examining the BOLD signal changes associated with interictal EEG spikes in people with temporal lobe epilepsy reveal the mechanism even further. 178 Such studies show widespread changes of BOLD activity, but of particularly interest for links between brain and behavior show altered activity in areas referred to as the “default mode of the brain,” notably the precuneus.
More studies are also needed to explore the neuroanatomic and functional brain abnormalities that may underlie these EEG abnormalities. Magnetoencephalography (MEG), a noninvasive method for identifying and evaluating patterns of epileptiform activity of deeper cortical tissue appear to be promising for precise localization of spikes and detection of subtle nonepileptiform abnormalities in the brain. MEG when compared to the conventional EEG has superior spatial and temporal resolution of spikes, may help in exploring the neurophysiologic mechanisms of nonepileptic cerebral dysrhythmia in neuropsychiatry. The science of MEG and its application to neuropsychiatry is in its infancy, and further developments are awaited.
CONCLUSIONS
It is important for both neurologists and psychiatrists to recognize this “terra incognita” that subclinical IEA are not uncommon in the various disorders at the brain-mind interface that are not associated with overt clinical epileptic seizures. At the borderlands of brain-mind disorders, the IEA is an “EEG chameleon,” since “all that spikes is not fits” that reminds us not to “mistake the woods for the trees.”
Footnotes
ACKNOWLEDGMENT
Dr. Shelley was a Visiting Research Fellow in Behavioral Neurology/Neuropsychiatry at the Raymond Way Neuropsychiatry Research Group, Institute of Neurology and Professor Trimble was funded by the Raymond Way Neuropsychiatry Research Group, Institute of Neurology, Queen Square, London.
DISCLOSURE AND CONFLICT OF INTEREST
B.P. Shelley and M.R. Trimble have no conflicts of interest in relation to this article.