
Abstract
Keywords
Introduction
Chimeric antigen receptor (CAR)-T cell therapy is a personalised immunotherapy that has drastically improved outcomes in people diagnosed with several cancer lines. 1 It has been offered as a specialist treatment for refractory haematological malignancy in the United Kingdom's (UK's) National Health Service (NHS) since 2018. At present, CAR-T is mainly used to treat leukaemia, particularly acute lymphoblastic leukaemia (ALL), and lymphomas, such as large B-cell lymphoma (LBCL) and mantle cell lymphoma (MCL).2–4
CAR-T cell therapy involves extracting T cells from a blood sample, inserting genes that code for the production of specific surface proteins, amplification of these cells, and reinfusion back into the person living with cancer. 1 The surface proteins expressed are known as chimeric antigen receptors (CARs). T cells with CARs (CAR-T cells) work by binding to a target antigen found on the surface of cancer cells. In leukaemias and lymphomas, the target antigen tends to be the cluster of differentiation 19 molecule (CD19). 5 CAR-T cells produced for other cancers may target different antigens on cell surfaces, such as B-cell maturation antigen (BCMA) in multiple myeloma. 6
Neurotoxicity, encephalopathy, and seizures are known sequelae following CAR-T cell therapy. 7 Many patients develop immune effector cell-associated neurotoxicity syndrome (ICANS), for which there is no specific objective biomarker, but has been reported in up to 70% of CAR-T patients in research populations. 8 ICANS describes a group of neurological symptoms that include confusion, headache, attention deficits, word finding difficulties, focal neurological deficits, transient coma, and seizures.8,9 The severity and duration of ICANS experienced is highly variable, ranging from a mild self-limiting course to severe life-threatening effects and death.
Local and national guidelines recommend the use of electroencephalography (EEG) to assess patients who develop toxicity following CAR-T cell therapy.10,11 The CAR-T-cell-therapy-associated TOXicity (CARTOX) Working Group recommends daily use of EEG in all grades of encephalopathy following CAR-T therapy, 11 whereas guidelines from the Society for Immunotherapy of Cancer (SITC) state EEG should be used in the ‘workup’ of all patients with possible encephalitis. 10 Our local guidelines recommend the use of EEG in patients who develop ICANS grade 2 or higher.
These guidelines are likely to increase referrals for EEG in this clinical scenario, which may be a relatively new field to some electroencephalographers. This single centre retrospective observational cohort study investigates EEG following CAR-T cell related neurotoxicity in routine clinical practice. The purpose of this study was to assess what value, if any, EEG adds to clinical assessment in this patient group. This included analysis of the diagnostic, clinical management, and possible neuroprognostic roles of EEG.
Methods
Ethical Approval
This study did not require ethical approval. Our institutional research and development department confirmed this study was not classed as clinical research under the UK's National Health Service (NHS)/Health Research Authority (HRA) policy framework for health and care research. It did, however, conform to relevant information governance requirements for retrospective data analysis.
Data Acquisition
Department records were searched with relevant keywords to identify all adult patients that had been referred to the neurophysiology department following initiation of CAR-T cell therapy. Patients were eligible for inclusion if they had received CAR-T cell therapy for any reason and had subsequently been referred to neurophysiology for EEG. The timeframe included all patients who received their first CAR-T infusion from inception of its use (first licensed in our institution in December 2018), up to and including 31st December 2023. Data of interest were retrospectively extracted and anonymised from written notes and online records that were deemed relevant and that were available. This included information from CAR-T cell therapy consent meetings, pre-infusion health assessments, inpatient notes, intensive care unit (ICU) admissions notes, outpatient haematology appointment notes, EEG referral forms, EEG reports, discharge summaries, and internal administrative summaries of death.
EEG Recording
EEG recordings were performed at the patient's bedside by qualified healthcare scientists (in neurophysiology). EEGs were acquired for 20–30 minutes using SystemPLUS Evolution (Micromed SpA Treviso, Italy). A minimum of 9, up to 19, silver/silver chloride recording electrodes were placed according to the 10–20 international system, with additional ground and reference electrodes. Occasionally a wide-spaced EEG montage was used where the primary clinical objective was to exclude non-convulsive status epilepticus or seizures in patients with delirium or disordered consciousness. The EEG was band-pass filtered between 0.53-70 Hz at −3 dB. A single channel electrocardiogram (ECG) was recorded simultaneously. During the recordings, auditory stimulation (calling of patient's name, requesting eye opening and closure) was performed. Where response to auditory stimulation was absent, somatosensory stimulation (trapezius squeeze) was attempted. Stimuli were applied with a minimum of 10 s intervals. The qualitative EEG findings were relayed to the treating clinicians at the time.
QEEG Grading
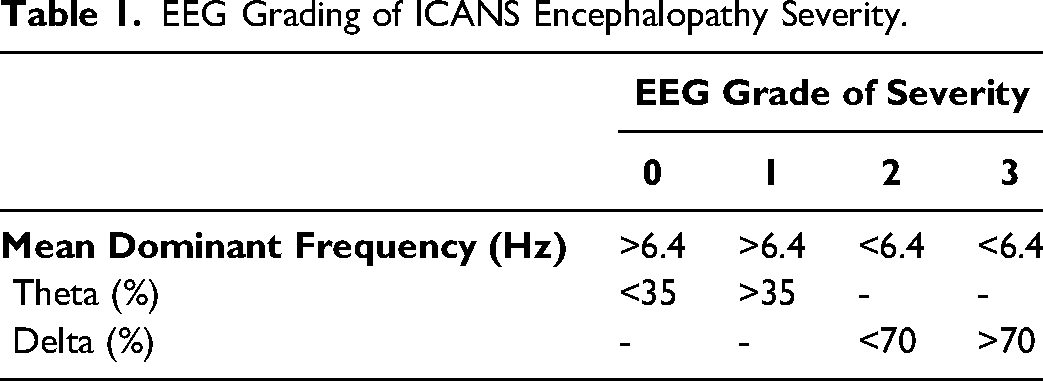
A validated quantitative approach was used retrospectively to grade EEG encephalopathy severity for the purpose of prognostic associations. 12 This analysis was performed by visual inspection of the quantitative EEG (QEEG) mean dominant frequency derived from the density spectral array (DSA) using SystemPLUS Evolution software (Micromed SpA Treviso, Italy) (see Table 1), by a single, experienced consultant clinical neurophysiologist blinded to all outcomes. Where a patient was referred for EEG more than once, all EEGs were graded, but the highest grade was used for prognostication. Examples of different grades using the DSA are given in Figure 1.
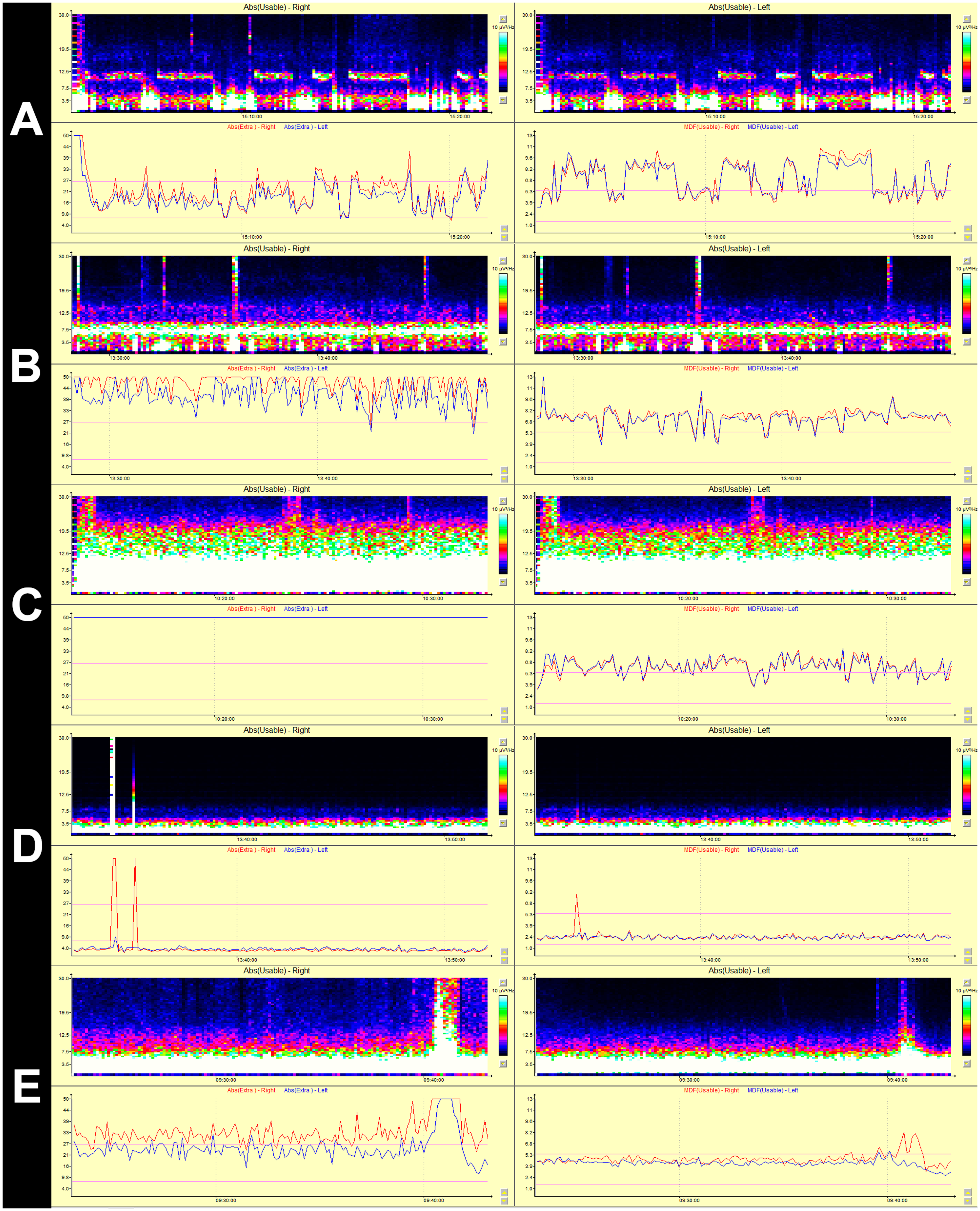
Density spectral array (DSA) examples of EEG grades 0 (A), 1 (B), 2 (C), 3 (D), and 3 with a seizure (E). The electroencephalogram DSA is a method of representation for spectral analysis. It uses a colour scale to display the power of each frequency component. Each spectrum is displayed by a coloured strip where the horizontal axis of each time point represents the EEG frequency, the colour of the point indicates the power.
EEG Grading of ICANS Encephalopathy Severity.
Clinical Measures
ICANS grade is calculated by combining scores across 5 different domains. These domains are:
Immune effector-cell associated encephalopathy (ICE) score, Level of consciousness, Presence and extent of seizures, Motor findings, and Raised intra-cranial pressure (ICP) or presence of cerebral oedema.
The way ICANS score is calculated is given in detail in the supplementary information.
The patient's level of functioning was measured using the Eastern Cooperative Oncology Group (ECOG) performance status scale. 13 This is a validated scale commonly used to assess function in people living with cancer. Scores used for analysis were taken at admission (baseline), at 1 month post CAR-T, 3 months post CAR-T, and the time at which values returned to baseline (in months) post CAR-T.
Data Analysis
Simple thematic analysis was used to identify and categorise the specific reasons for EEG referral. These word data were extracted from the text field of EEG requests. Themes were identified and split into three broad categories, albeit not mutually exclusive:
Inclusion or exclusion of ongoing seizures/non-convulsive status epilepticus (NCSE), Inclusion or exclusion of encephalopathy/encephalitis or cerebral infection, and Other questions eg explanation of change in neurology, low Glasgow Coma Scale (GCS) scores (reduced consciousness), or severity of neurotoxicity.
The frequencies of thematic codes were subsequently tabulated and summarised.
Pearson correlation coefficients and area under receiver operating characteristic (AUROC) curve analyses were performed to analyse the relationship between QEEG grade and relevant health outcomes. These outcomes included: ICANS grade (see supplementary information on calculating ICANS score); functional status change at 1 month, 3 months, and time to return to baseline (in months); and survival at 1 month, 3 months, and 6 months.
Pearson correlation coefficient was used to analyse the relationship between QEEG grade and length of inpatient stay (in days). AUROC analysis was used to assess the relationship between QEEG grade and ICU admission, and between ICANS grade and ICU admission. Pearson correlation and Student's t-tests were used to assess and account for possible intergroup differences in age according to EEG grades.
Results
Summary of Data Availability
In total, 116 adult patients received their first CAR-T cell therapy infusion between December 2018 and 31st December 2023 in our institution. Fifty patients (50/116; 43.1%) developed ICANS neurotoxicity of any grade. Twenty-eight (28/116; 24.1%) were referred for EEG with ongoing neurological symptoms, regardless of their ICANS grade. Data were extracted and analysed for all 28 of these patients. QEEG grade, ICANS grade, ECOG baseline data, ICU admission data, and survival data were available for all patients (28/28; 100%). ECOG scores at 1 month post CAR-T were available for twenty patients (20/28; 71.4%); 1 patient had died, 7 did not have recorded values in written or online notes. For ECOG scores at 3 months, nineteen patients (19/28; 67.9%) had data available; 7 patients had died, 2 patients did not have recorded values in written or online notes. For ECOG return to baseline, twenty-one patients (21/28; 75.0%) had data available; 7 patients died prior to returning to baseline. Inpatient duration of stay data was available for twenty-three 23/28 (82.1%) patients, since 5 patients died as inpatients.
Relevant background information for this cohort (n = 28) has been summarised in Table 2. Further information is available in supplementary information.
Summary of Patient Characteristics.
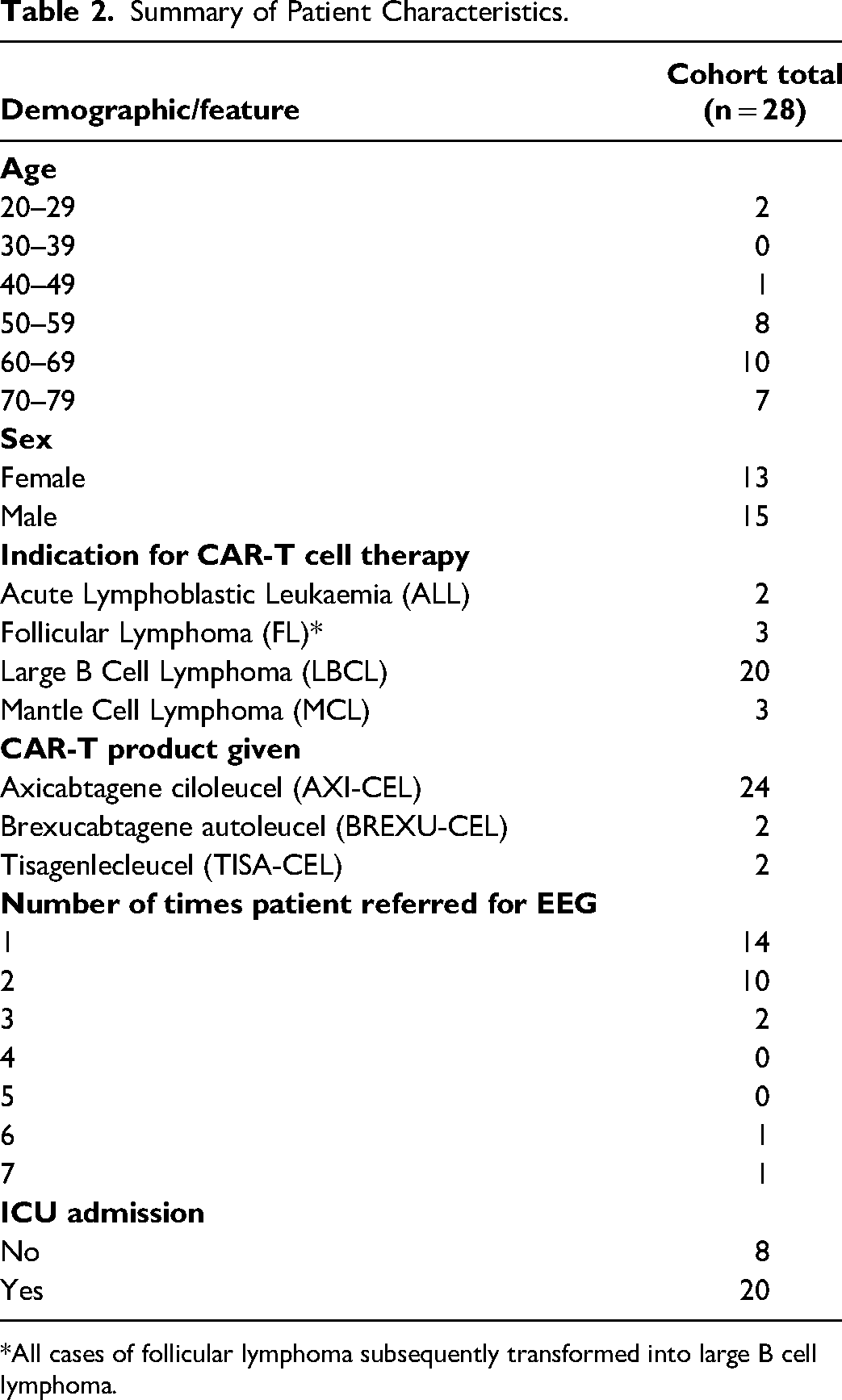
*All cases of follicular lymphoma subsequently transformed into large B cell lymphoma.
EEG Referrals
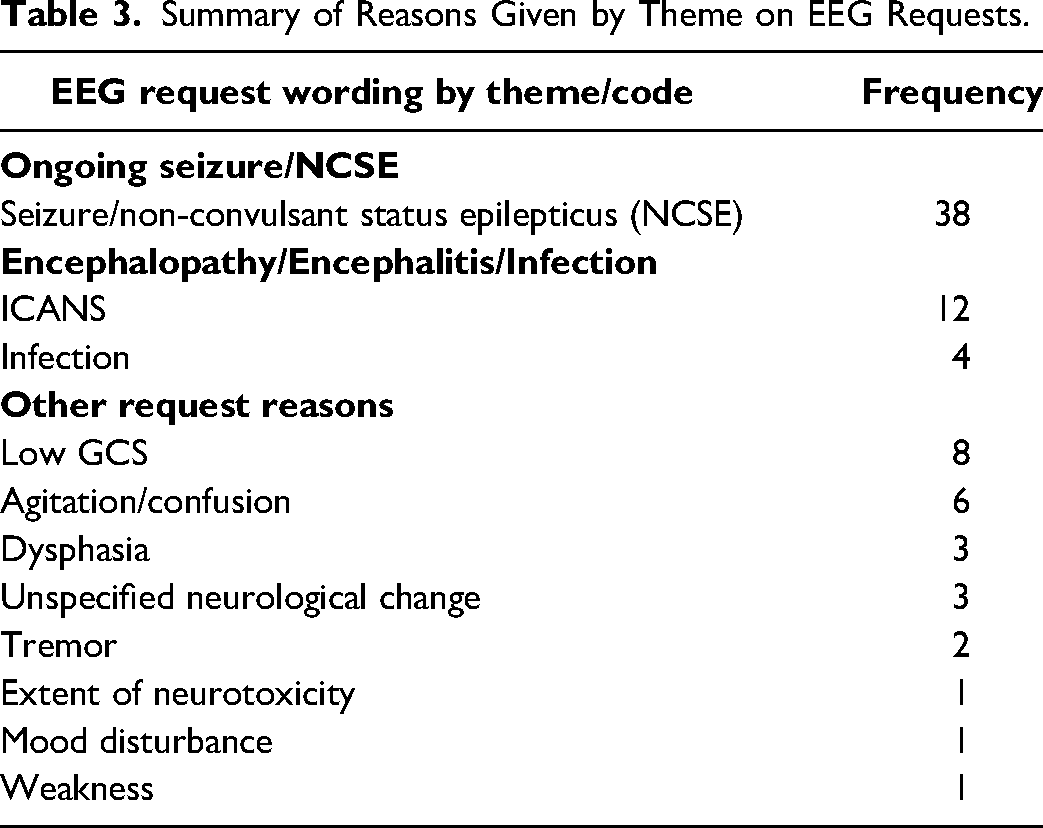
There was variation and overlap in the reasons given for EEG requests across the 53 referrals made for these 28 patients. Primarily, the single most common indication for EEG was the diagnosis and classification of possible seizure or non-convulsive status epilepticus (n = 38). Secondly, clinicians wanted to assess the presence of encephalopathy/encephalitis or cerebral infection (n = 16). Requests also described a range of neurological symptoms, for example low GCS (n = 8), and asked whether EEG could offer insights as to the cause of these, without suggesting any specific diagnosis for inclusion or exclusion. In a single case, there was a request for assessment of the ‘extent of neurotoxicity’ in a patient with known ICANS, and the absence of such an objective EEG grading scale for CAR-T in part prompted this study. The frequencies of these themes are summarised in Table 3.
Summary of Reasons Given by Theme on EEG Requests.
Diagnostic Value of EEG
Electrographic evidence of focal seizure was observed on four occasions in three EEGs (3/53; 5.7%) for two different patients, both of whom died. No cases of generalised seizure or NCSE were detected. There was no specific EEG evidence of infection. Most EEGs (47/53; 88.7%) showed some degree of encephalopathy.
The Relationship Between QEEG and ICANS Grade
Quantitative EEG severity of encephalopathy was graded as described in the methods section. QEEG grades were correlated with the highest ICANS value for each patient during inpatient stay around the time of EEG. The Pearson correlation coefficient between QEEG grade and ICANS grade was r = + 0.41 (p = .030).
Admission to ICU and Inpatient Stay Duration Outcomes
Twenty patients (20/28; 71.4%) were admitted to ICU. The reasons for ICU admission were given as: ICANS (7/20; 35.0%); ICANS and/or cytokine release syndrome (CRS) (4/20; 20.0%); CRS (3/20; 15.0%); persistent hypotension (3/20; 15.0%); ICANS and/or sepsis (2/20; 10.0%); CRS and/or sepsis (1/20; 5.0%).
The performance of ICANS grade and QEEG grade were assessed for their ability to predict ICU admission. AUROC analysis showed predictive ability of ICANS grade area under curve (AUC) = 0.250, and QEEG grade had AUC = 0.444.
The average duration of inpatient stay (in days) of the patients surviving to discharge (23/28; 82.1%) was 18 days. The correlation between QEEG grade and the length of stay (in days) as an inpatient had Pearson correlation r = + 0.08 (p = .723).
Survival and Functional Performance status Outcomes
Twenty-seven patients (27/28; 96.4%) survived to 1 month post CAR-T. Twenty-one patients (21/28; 75.0%) survived to 3 months. Seventeen patients (17/28; 60.7%) survived to 6 months. The performance of QEEG grade at predicting survival was assessed using AUROC analysis. At 3 months, AUC = 0.673. At 6 months, AUC = 0.578. With only a single death by 1 month post CAR-T, statistical analysis was not appropriate for this timepoint.
The QEEG severity grade was assessed for its ability to predict performance status change and recovery (ECOG values). Each patient's QEEG grade was correlated with their respective ECOG value change from baseline at 1 month and 3 months. We also assessed the correlation between QEEG grade and the time taken to return to baseline ECOG values in months.
At 1 month, the Pearson correlation coefficient was r = + 0.40 (p = .080). At 3 months, the correlation was r = + 0.19 (p = .439). Seven patients died before returning to baseline ECOG values. All patients that survived to 6 months had ECOG values that returned to baseline. The correlation between QEEG grade and time taken to return to baseline (in months) was r = + 0.32 (p = .156).
QEEG and Age
There was no correlation between EEG grade and age; Pearson r = -0.26 (p = .189). There was no significant difference in age between EEG grade groups using Student's 2 tailed t-test analysis. All inter-group values had p > .05.
Discussion and Conclusions
Background and Context
A recent literature review suggests there may be a role for EEG in the monitoring, prognosis, and exclusion of certain pathologies in a number of causes of encephalopathy and encephalitis. 14 The American Society for Transplantation and Cellular Therapy suggests that EEG may have a specific role in cancer immunotherapy related encephalopathy; to exclude focal seizures or non-convulsive status epilepticus (NCSE). 11
In this study, our findings on the use of portable routine EEG following CAR-T cell therapy induced encephalopathy/neurotoxicity are reported from a single regional centre in the UK. We describe real world data reflecting the use of EEG in this clinical context. It is timely to report these findings, since in 2023 CAR-T cell therapy was approved for routine use as a third line therapy for large B-cell lymphomas (LBCL) in the UK. 15 This was the most common indication for CAR-T in our patient population (20/28; 71.4%). As a result, neurophysiology departments are likely to see an increase in the number of EEG referrals for patients like those described in our cohort.
Our local guidelines recommend that all patients diagnosed with ICANS grade ≥2 following CAR-T are referred for EEG. Some patients developing ICANS will have been below this threshold, hence not referred.
Anecdotally, the referring haematologists advised us that referrals are often not made over the weekend and are cancelled if symptoms self-resolve, which may further explain why only 28 out of 50 patients with apparent neurotoxicity had EEG recordings.
It is also possible that rather than following local guidelines, some referring clinicians preferentially used other national/international guidelines that recommend use of EEG in the workup of all CAR-T patients developing neurotoxicity. This may explain why some patients with ICANS grade lower than 2 were referred for EEG.
Interpretation of Results
Most of the themes stated in EEG referrals are unlikely to surprise electroencephalographers. Seizures and non-convulsive status epilepticus are the single most common indication for an EEG (n = 38 referrals here). Although any seizure type was only confirmed on 4 occasions on 3/53 (5.7%) EEGs, this does conform to the known seizure risk in CAR-T. All 4 episodes of seizure activity recorded were focal seizures. No electrographic evidence of generalised seizure was found. The relatively low rate of electrographic seizure detection is most likely a by-product of the limited sampling by intermittent short duration EEG recordings. While continuous EEG (cEEG) monitoring may be more desirable for this purpose, it does not reflect routine practice in most NHS hospitals in the UK,9,14,16 and therefore may have limited practical application outside of high income countries or the research environment.
Half of the patients (14/28; 50.0%) had only a single EEG recording, with 10/28 (35.7%) receiving 2 recordings, and the remaining 4 patients receiving 3-7 EEGs. The reasons for repeat EEG were variable across the 14 patients receiving 2 or more recordings. Sometimes, the referring clinician would refer a patient for repeat EEG with essentially the same request as the original. For example, the patient that had 7 EEG recordings was referred for possible NCSE/subclinical seizure on all 7 occasions. This patient was started on multiple anti-seizure medicines, steroids, and other medication regardless of the EEG outcome. In addition, while treating clinicians may believe that EEG could be used to monitor improvements in the patient's encephalopathic state using EEG, this contradicts our data which suggests there is limited prognostic ability. These factors suggest that repeat EEG offers little useful additional information for repeated monitoring with the same referral reason.
For other patients, repeat EEG was requested for different reasons when compared to their initial request. For example, in one case, an initial request for EEG to investigate a patient who was not waking up as expected was made. The subsequent EEG requested for this patient was to investigate possible focal seizure, but only after they had regained consciousness. Given the change in the patient's condition, these requests both had the potential to offer new information for the clinicians. We would recommend only routinely seeking repeat EEG if there has been a change in the patient's symptoms or condition, and there is a different possible differential diagnosis. Repeat EEG for the same reason appears to add little value in this group of patients.
Given the immunosuppressed state of CAR-T patients, referrals enquiring about superimposed infection are understandable, but perhaps of questionable value, as EEG may show disease specific patterns in only a very few cerebral infections, such as herpes simplex encephalitis. 17 Given there are many potential cerebral infections which may not even be confirmed electrographically, this is perhaps a relatively limited use of EEG in this setting.
In a single case, the referral asked for the ‘extent of neurotoxicity’. This may reflect a belief by treating clinicians that EEG is an established objective method of measuring neurotoxicity/encephalopathy. The degree of background EEG slowing has been observed to correlate with the severity of neurotoxicity in 2 large case series,18,19 although the pathophysiological mechanism is not yet fully understood. 19 There is also limited evidence for the application of objective QEEG for this purpose. We found that there was a moderately positive Pearson correlation (r = + 0.41) between QEEG grade and ICANS grade, which is broadly similar to previous reports with Pearson correlation r = + 0.58, 18 and Spearman correlation ρ = + 0.50. 19 There is currently no reason to suggest that EEG could replace bedside scales such as ICANS, but it does potentially offer an adjunct condition-specific objective biomarker, as suggested by Jones et al (2022). 18
The QEEG grade and ICANS grade of patients were unable to predict admission to ICU based on AUROC analyses. QEEG grade was not proportional to the length of inpatient stay (in days) according to Pearson correlation. The QEEG grade was not able to reliably predict survival in our cohort at 3 or 6 months based on AUROC analyses. Insufficient data was available to perform statistical analysis for 1 month survival. QEEG was not able to predict functional status change/improvement of this patient group at 1 or 3 months. It was also not able to predict the time to return to baseline functional levels. Overall, QEEG showed no significant ability to prognosticate for these health outcomes, which may reflect the complexity of these patients. This is important information for clinicians in this field, because EEG reportedly has some neuroprognostic role in other situations, such as viral encephalitis, 20 hepatic encephalopathy, 21 and hypoxic ischaemic encephalopathy. 22
Patients were treated with several medications as soon as they were diagnosed with ICANS. In 15/28 (53.6%) patients, clinical seizure was reported, and therefore anti-seizure medication could be considered treatment. In the other 13/28 (46.4%) patients, anti-seizure medication could be considered prophylactic or precautionary. In all cases, levetiracetam was given (and continued over EEG recording period), alongside other medicines including steroids and monoclonal antibodies (see supplementary information).
Treatment change was observed on no occasion following review of EEG. In addition, while radiological imaging such as magnetic resonance imaging (MRI) and computed tomography – positron emission tomography (CT-PET) results fall outside the remit of this study, we note that these imaging modalities were often requested during inpatient stay. None of these tests appeared to directly follow EEG review. The use of EEG in this patient group did not lead to any apparent change in patient management.
Given the lack of changes in patient management following EEG observed in this cohort, it would be difficult to justify the use of EEG in routine workup of CAR-T patients. EEG would be best used where there are specific clinical questions which EEG may help answer.
The relevance of this study is that it reflects real world use of routine EEG in standard clinical practice, using real-time commercially available EEG analytical tools. Overall, patients were generally young and healthy, with relatively few comorbidities (including no neurological co-morbidities likely to affect EEGs) alongside their haematological diagnosis, so co-existing health problems were unlikely to impact on their background EEG patterns.
All patients developed CRS to some extent, encompassing all grades. 9/28 (32.1%) developed grade 1, 13/28 (46.4%) grade 2, 5/28 (17.9%) grade 3, and 1/28 (3.6%) grade 4. CRS is a significant risk factor for development of ICANS, and our trust also has specific local guidelines to help manage CRS. Management in our cohort included use of steroids (28/28; 100%), tocilizumab (27/28; 96.4% received at least one dose), anakinra (8/28; 28.6%), and siltuximab (2/28; 7.1%). There was no correlation found between CRS grade and ICANS grade in our cohort, r = + 0.07 (p = .727).
Treatment Indication, CAR-T Product Mechanisms, and Rates of Neurotoxicity
Use of costimulatory intracellular signalling is key to effective functioning of CAR-T therapies.23,24 Our study reports on the use of 3 different CAR-T products utilising 2 different costimulatory signalling domains; CD28 and 4-1BB (CD137). Twenty-four out of twenty-eight (24/28; 85.7%) patients received Axicabtagene ciloleucel (AXI-CEL) which uses CD28 costimulatory molecules, 2/28 (7.1%) received Brexucabtagene autoleucel (BREXU-CEL) which also uses CD28 costimulatory molecules, and 2/28 (7.1%) received Tisagenlecleucel (TISA-CEL) which uses 4-1BB (CD137) costimulatory molecules.
The 2 patients that received TISA-CEL with 4-1BB costimulatory molecules both had QEEG grade 3 encephalopathy. Both of these patients were treated for ALL. The 2 patients treated with BREXU-CEL with CD28 costimulatory molecules had grades 1 and 3 QEEG encephalopathy scores. Both of these patients were treated for MCL. The remaining 24 patients treated with AXI-CEL with CD28 costimulatory molecules had grades 0-3 of encephalopathy from QEEG. They were treated for follicular lymphoma (FL), LBCL, and MCL.
There is not enough data to elicit a correlation between co-stimulatory molecules and QEEG grade, since only 2/28 (7.1%) patients received the TISA-CEL with 4-1BB compared to 26/28 (92.9%) receiving AXI-CEL or BREXU-CEL with CD28. It is still interesting to note that both TISA-CEL 4-1BB patients had grade 3 encephalopathy (the worst level of encephalopathy on QEEG), however the literature reports no significant difference in rates of neurotoxicity or safety profile between these 2 costimulatory molecules.23,24
The 2 patients receiving TISA-CEL were young (both in their 20s) and both were being treated for ALL, either of which could be an as yet unknown reason for greater extent of encephalopathy, although there is no reason or evidence to support this.
The number of patients receiving CAR-T for the different indications, ALL (2/28; 7.1%), FL (3/28; 10.7%), MCL (3/28; 10.7%), and LBCL (20/28; 71.4%), were too low to offer any useful statistical inter-group differences.
Limitations
Limitations of this single centre retrospective observational study include availability of some of the ECOG values at 1 and 3 months. Also, the ICANS score was not always available at the exact moment of the EEG recording, and therefore the values may not be contemporaneous. We note that the use of maximum ICANS grade is still likely to have been reflective of the patient state at time of the EEG, since requests for EEG are routinely cancelled when patients improve. Furthermore, intermittent short duration EEG recordings have recognised limited sampling of both seizures and possibly natural fluctuations in encephalopathy severity; which may account for the enhanced correlation achieved by long-term cEEG recordings.18,19 EEGs were typically performed on the same day as the request, where these were made during service hours. These EEGs were also typically reported on the same day they were recorded. There were very limited records stating exact dates of ICANS onset, which means it is not possible to determine the delay between onset of ICANS and EEG reporting with any accuracy.
We could only include patients that had EEGs performed in our analysis. EEGs were more likely to be performed in those with higher ICANS scores. It should be noted that if EEGs were performed on all 50 patients who developed ICANS, the results may be different. A prospective EEG study including all patients diagnosed with ICANS may provide stronger evidence for the basis of these conclusions, in particular the prognostic associations reported.
Patients that died may have had different ECOG grades than those who survived, thus creating the possibility of survivorship bias. ECOG values could naturally get worse as malignancy progressed. In a single case, the patient's ECOG score improved after recovering from ICANS (see supplementary information).
EEGs taken and analysed could not be compared to baseline since baseline EEGs are not performed in clinical practice. Prior to commencing CAR-T treatment, no patient had any disease associated with encephalopathy or could otherwise induce slowing of dominant frequencies. Nor were any patients on any medication that would have adversely affected an EEG prior to treatment. There is no reason to believe that any patients would have been graded as anything other than 0 before the start of treatment.
Typically, the dominant rhythm observed on EEG may slow by 1 Hz or more over a lifetime. 25 Although this slowing effect was not accounted for during QEEG analysis, the distribution and statistical analysis of patients in our study suggested there was no evidence this slowing effect has influenced QEEG encephalopathy grading.
All patients were on multiple medications for infection prophylaxis as well as ICANS treatment, including steroids, other immunosuppressants, and antiseizure medications, which may potentially have affected EEG interpretation. For example, Levetiracetam was given to all patients as soon as treating clinicians were suspicious of ICANS, and patients remained on these during EEG recordings. This is, however, reflective of the clinical context of this patient population, and therefore remains relevant for real world decision making.
Our patient numbers were too small to consider subset analysis of other infrequent EEG graphoelements (eg interictal epileptiform and repetitive periodic discharges, or triphasic waves), although it was nearly always possible to quantitatively assess their background EEG.
Conclusions
QEEG can add some potential value as an objective biomarker in patients presenting with encephalopathy/neurotoxicity following CAR-T cell therapy. It is useful in seizure diagnosis, but not generally in the detection of encephalitis/infection. The use of post CAR-T EEG generated no tangible change in patient management. QEEG was unable to prognosticate on survival, ICU admission, duration of inpatient stay, or functional status in patients with CAR-T related neurotoxicity.
Supplemental Material
sj-xlsx-1-eeg-10.1177_15500594241312451 - Supplemental material for The Role of Electroencephalography Following CAR-T Cell Therapy in Clinical Practice
Supplemental material, sj-xlsx-1-eeg-10.1177_15500594241312451 for The Role of Electroencephalography Following CAR-T Cell Therapy in Clinical Practice by Alexander J Matthews, Fiona E Starkie, Lydia E Staniaszek and Nicholas M Kane in Clinical EEG and Neuroscience
Footnotes
Author Contributorship
This study was conceptualised by LS and NK. Data acquisition was performed by AM, FS, and LS. Objective QEEG grading was performed by NK. Statistical analysis was performed by AM. All authors contributed to analysis and interpretation of results. The manuscript was drafted by AM. All authors contributed to critical review and approval of the final manuscript.
Data Availability Statement
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval and Informed Consent Statement
Our institutional research and development department confirmed this study was not classed as clinical research under the UK policy framework for health and care research. It therefore did not require Health Research Authority (HRA) and/or National Health Service (NHS) research ethics approval. It did, however, conform to relevant information governance requirements for retrospective data analysis.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.