
Abstract
Objective
This study evaluated whether quantitative electroencephalography (QEEG) guided neurofeedback (NF) improves intellectual functioning and attention in children with mild to severe intellectual disability (ID).
Methods
Sixty-five children (38 males, 27 females; mean age ≈11 years) with DSM-5 diagnoses of mild-to-severe ID (IQ 28-68) and histories of unsuccessful standard treatments were enrolled. Baseline assessments included 19-channel QEEG referenced to FDA-approved Nx-Link™, BrainDx™, and NeuroGuide™ databases, Wechsler Intelligence Scale for Children (WISC-R or WISC-IV),and the Test of Variables of Attention (TOVA). Participants underwent 80-120 QEEG-guided NF sessions. Training protocols targeted deviant z-scores, with hypercoherence addressed prior to amplitude abnormalities. IQ and attention were reassessed 6–12 months post-treatment. Outcomes were analyzed using paired t-tests, correlation analyses, and generalized linear models.
Results
Mean full-scale IQ increased by approximately 10 points (≈53 to ≈63; +18.6%, p < 0.001). Significant gains were observed in both WISC-IV (+≈11 points) and WISC-R (+≈10 points), with improvements across verbal, perceptual, working memory, processing speed, and performance domains (all p < 0.001). Two thirds of participants' IQ increased by ≥6 points. TOVA scores improved but were not correlated with IQ changes. QEEG analyses showed normalization of resting-state networks, including increased alpha power in default mode network hubs and reduced coherence and phase lag; reductions in slow-wave coherence predicted IQ improvement.
Conclusion
QEEG-guided NF was associated with clinically meaningful improvements in intellectual functioning and attention in children with ID, exceeding gains expected from environmental enrichment. Findings support NF as a promising nonpharmacologic intervention warranting randomized controlled trials.
Introduction
Intellectual disability is a developmental condition characterized by significant limitations in reasoning, learning, and problem-solving. 1 The Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5) defines ID as performance approximately two standard deviations below the population mean (intelligence quotient [IQ] ≤ 70) coupled with impairments in adaptive functioning across domains such as communication, self-care, social skills, and community use. 1 Abnormal electroencephalographic (EEG) patterns are common in ID; children with mild ID display delayed alpha development and predominant low-frequency activity, 2 while resting EEG often shows maturational lag in delta, theta, and beta bands and reduced antero-posterior differentiation. 2
Intelligence test scores measure reasoning, working memory, processing speed, and verbal abilities. 3 Neuroimaging studies link these cognitive abilities to specific neural characteristics, including increased white matter integrity and myelination 4 and enhanced metabolic activity in fronto-parietal networks, 5 suggesting that intelligence relates to neural tissue quality rather than mere quantity.6 The parieto-frontal integration theory posits that connections among the dorsolateral prefrontal cortex, anterior cingulate, and parietal lobes underlie individual differences in intelligence. 7 These neural networks are malleable; synaptic strengthening, dendritic branching, and increases in gray matter volume are mechanisms of neuroplasticity linked to cognitive gains.8,9
The default mode network represents a particularly dense neural architecture implicated in these cognitive processes, comprising the cingulate gyrus, hippocampus, medial frontal, temporal, and parietal regions with approximately five times more synaptic connections than other cortical networks.10,11 Active during rest and self-referential processing, DMN connectivity dynamics correlate with intelligence measures, with phase synchronization patterns showing systematic relationships to IQ scores. 12 During neurodevelopment, the DMN facilitates integration of sensory and cognitive information, supporting autobiographical memory, self-reflection, and emotion regulation 13 ; functions often compromised in intellectual disability.
Approaches to Enhance IQ
Environmental enrichment and cognitive training can modestly enhance IQ. 14 Meta-analysis evidence indicates that cognitively enriched environments yield long-term IQ increases of 1–5 points, 8 and working memory training can temporarily improve fluid intelligence.9,15,16
A study by Jaeggi et al 17 reported evidence that training on a challenging working memory task can improve fluid intelligence (Gf), even when the training task is completely different from the intelligence test used to measure it. The improvements in Gf increase with more training, demonstrating a dose-dependent effect and suggesting that Gf can be enhanced without direct practice on intelligence tests.
Non-invasive brain stimulation techniques such as transcranial direct current stimulation (tDCS), transcranial random noise stimulation (tRNS), transcranial alternating current stimulation (tACS), and repetitive transcranial magnetic stimulation (rTMS) have been explored. Although multi-session tRNS over the left dorsolateral prefrontal cortex (DLPFC) enhances mathematical reasoning and fluid IQ,18 single-session effects are weak and individualized protocols are needed. 19
During math training, tRNS accelerates learning and transfers to untrained IQ tests but shows no benefit when combined with working memory training.18 Theta–gamma tACS over left parietal cortex can enhance fluid IQ on challenging tasks, 20 and rTMS over left DLPFC transiently improves problem-solving. 21
Meta-analytic review showed combined neuromodulation and cognitive training may boost working memory and attention. 22 Neurofeedback paired with executive function coaching has shown gains in verbal and full-scale IQ in adolescents with learning difficulties. 23
Despite these advances, several limitations remain. IQ test performance is susceptible to various noncognitive influences such as attention, motivation, arousal, and anxiety,24,25 which can produce systematic underestimates of true ability. Given that test scores reflect not only latent intelligence but also these confounding factors, 26 improvements in attention following interventions may enhance performance without necessarily indicating genuine changes in underlying cognitive capacity.
Moreover, many studies report improvements on specific subcomponents (eg, working memory) rather than full-scale IQ, and small sample sizes and protocol variability limit replicability.17,27,28
Longitudinal studies show that IQ in ID is generally stable or declines slightly.29–31 Spitz 32 reviewed the history of attempts to raise IQ in developmentally delayed and/or culturally disadvantaged children. Efforts included early intervention and compensatory education programs such as Head Start, behavior modification, medical and dietary interventions, and various sensory and motor therapies. Spitz concluded that none has shown any significant effect in raising intelligence scores.
These challenges justify exploring alternative interventions, such as QEEG guided NF, that directly target brain network dynamics.
Neurofeedback and QEEG Rationale
Neurofeedback trains individuals to self-regulate cortical oscillations by providing real-time feedback on specific EEG parameters.33,34 QEEG-guided NF uses normative databases to identify abnormal spectral power (the amplitude of specific frequency bands), coherence (the consistency of phase relationships between brain regions), or phase patterns (the timing of oscillatory activity) and offers insights into how the clinician should tailor NF protocols accordingly.35,36
Evidence suggests that NF can normalize EEG patterns and improve cognition in attention-deficit/hyperactivity disorder, learning disabilities, epilepsy, and intellectual disability,37,38 Fernández et al, 2007;.39–42 In a small case series, QEEG-guided NF improved Wechsler Intelligence Scale for Children Revised (WISC-R) IQ scores by > 6 points in 19 of 23 children with intellectual disability (severity of degree: from moderate to mild). 39 These findings led to the hypothesis that normalizing brain electrical activity via QEEG-guided NF could improve intellectual functioning and brain coordination in children with ID. 39
Methods
Participants
The study recruited 65 children with ID (38 males, 27 females) aged 6–16 years (mean ≈ 11 years). Participants were categorized into WISC-R (n = 48; mean age 11.19 ± 2.47 years) and WISC-IV (n = 17; mean age 11.00 ± 2.89 years) cohorts according to the IQ test administered. In the DSM-5, intellectual disability is characterized by general IQ ranges that serve as rough guides rather than strict cutoffs, with an IQ of approximately 70 or below typically raising concern for ID. 1 Severity is conventionally stratified into mild (≈50-55 to 70), moderate (≈35-40 to 50-55), severe (≈20-25 to 35-40), and profound (below ≈20-25). Consistent with this framework, severity at baseline was classified using pre-treatment full scale IQ: Severe (IQ 28-39; 4 cases), Moderate (IQ 40-54; 30 cases), and Mild (IQ 55-69; 31 cases).
All participants carried a prior diagnosis of intellectual disability, which was reviewed and verified at the clinic by a multidisciplinary team comprising a psychiatrist and a clinical psychologist, in accordance with DSM-5 criteria. Brain MRI scans were requested from external centers for participants who did not have prior imaging. In all cases, neuroimaging findings were negative for organic brain pathology.
Inclusion and Exclusion Criteria
Materials and Assessment Instruments
QEEG Acquisition
Resting EEG data were recorded from 19 scalp locations according to the international 10–20 system (Fp1, Fp2, F7, F3, Fz, F4, F8, T3, C3, Cz, C4, T4, T5, P3, Pz, P4, T6, O1, O2). Signals were analyzed using FDA-approved quantitative QEEG databases (Nx Link™, BrainDx™, and NeuroGuide™) to compute Z-scores for multiple metrics. Z-scores represent standardized measures indicating how many standard deviations each participant's values deviated from age-matched normative means. Three primary QEEG metrics were assessed: Coherence (the consistency of phase relationships between brain regions), Phase lag (timing differences in oscillatory activity between regions), and Absolute/Relative power (the amplitude of specific frequency bands). 46 Z-scores of ≥1.95 or ≤ −1.95 indicated clinically significant deviations from normal, while pre-treatment to post-treatment changes approaching zero reflected normalization toward age-expected values.36,47
IQ Testing
Intellectual functioning was assessed with either the Wechsler Intelligence Scale for Children - Revised (WISC-R 48 ; or the Fourth Edition (WISC-IV;. 3 WISC-R yields verbal and performance IQ, while WISC-IV provides indices of verbal comprehension, perceptual reasoning, working memory, and processing speed. 3 Baseline testing occurred before NF treatment. WISC-R outcomes were reassessed 6 months after treatment completion and WISC-IV outcomes at 12 months. Clinical psychologists blinded to treatment status administered all tests. As this is a retrospective study, each group was assessed using the version of the WISC that was in use at the time. Since the WISC-IV was introduced later, we analyzed and presented the results for the two groups separately.
Attention Measurement
Sustained attention and inhibitory control were measured with the Test of Variables of Attention (TOVA 49 ; in both visual and auditory modalities. Variables included response time (RT), response time variability (RTV), omission errors, and commission errors.
Laboratory Measures
Routine blood tests (eg, complete blood count, vitamin B12, folate, vitamin D, thyroid-stimulating hormone) were collected to monitor general health. Laboratory values were not used as exclusion criteria, as they were not significant.
Neurofeedback Intervention
Treatment Structure and Dosage
Each participant completed 80–120 sessions (mean = 100 ± 11.5) over 3–3.5 months, with sessions scheduled daily except weekends. This dosage was determined based on clinical experience with intellectual disability populations, with treatment continuing until observable improvement occurred. Two types of sessions were employed: standardized weighted low-resolution electromagnetic tomography Z-score neurofeedback (swLZNFB) sessions lasting 40 min, and amplitude training sessions lasting 30 min. Training was conducted using Lexicor™ Biolex, Thought Technology™ ProComp2, Mitsar™, and NeuroGuide™ software.
Protocol Individualization
All treatment protocols were individualized based on each participant's QEEG profile. Electrode sites and training parameters were selected according to deviant Z-scores identified in the baseline QEEG assessment, with protocols guided by clinician experience and supporting validation data. 50
Targeting Hierarchy
QEEG analysis revealed that hypercoherence (excessive synchronization between brain regions) was commonly present in this population. As hypercoherence disrupts neural connectivity, it was prioritized as the primary treatment target when present. Following hypercoherence normalization, protocols then addressed relative power abnormalities in specific frequency bands.
Specific Training Protocols
Coherence and Power Protocols
Bipolar training at homologous sites (Fp1–Fp2, F3–F4, C3–C4, P3–P4, T3–T4, O1–O2) was used to inhibit excessive alpha or beta coherence and amplitude while reducing delta and theta activity. These bilateral montages were the most frequently employed protocols in this patient population.
Attention and Motivation Protocols
Frontal montages (Fp1–Fp2, Fp1–F3) targeted improvements in sustained attention and motivational engagement.
Sensorimotor and Sleep Protocols
Cz–C4 bipolar montages trained sensorimotor rhythms (SMR) to support motor regulation and sleep quality.
Additional Symptom-Specific Protocols
SwLZNFB protocols also addressed anxiety, impulsivity, executive function deficits, DMN dysregulation, and academic skill difficulties as indicated by individual clinical presentations.
Network-Level Analysis
To examine treatment effects on large-scale brain networks, we assessed functional connectivity within the DMN using exact Low Resolution Electromagnetic Tomography (LORETA 51 ; based analysis implemented in BrainDx™ software. We analyzed eight key DMN hubs comprising cortical midline structures (anterior cingulate cortex (ACC), cingulate gyrus, posterior cingulate cortex (PCC), precuneus, subcallosal gyrus, parietal regions (angular gyrus, supramarginal gyrus), and the insular lobe; regions known to support self-referential processing and executive function.
Procedure and Statistical Analysis
Baseline assessments (QEEG, WISC-R/WISC-IV, TOVA, and Developmental Behavioral Checklist, Parent reports, family history) were conducted prior to NF. Post-treatment assessments (QEEG and WISC) occurred at 6 months for the WISC-R group or 12 months for the WISC-IV group, and TOVA assessment was completed immediately after NF treatment completion. Statistical analyses employed paired t-tests to compare pre-treatment and post-treatment scores, correlation analyses to examine relationships among IQ, attention, and electrophysiological changes, and generalized linear models to evaluate predictors of cognitive change. The study corrected for possible confounding effects of attention on IQ by examining correlations between TOVA changes and IQ change.
Throughout treatment, participants and parents were recorded via webcam every 20 sessions to monitor behavioral changes and to provide documentation for retrospective evaluation of treatment functionality and clear observation of baseline status and progress.
Results
Overview of Cognitive Outcomes
Neurofeedback intervention resulted in statistically significant improvements in overall intellectual functioning. Mean full-scale IQ increased from baseline (M = 52.98, SD = 9.77) to post-treatment (M = 62.83, SD = 12.74), representing a mean gain of 9.85 IQ points, t (66) = 10.43, P < .001, d = 0.89, indicating a large effect size. Improvements were observed across both WISC-R and WISC-IVsubgroups (Figure 1).
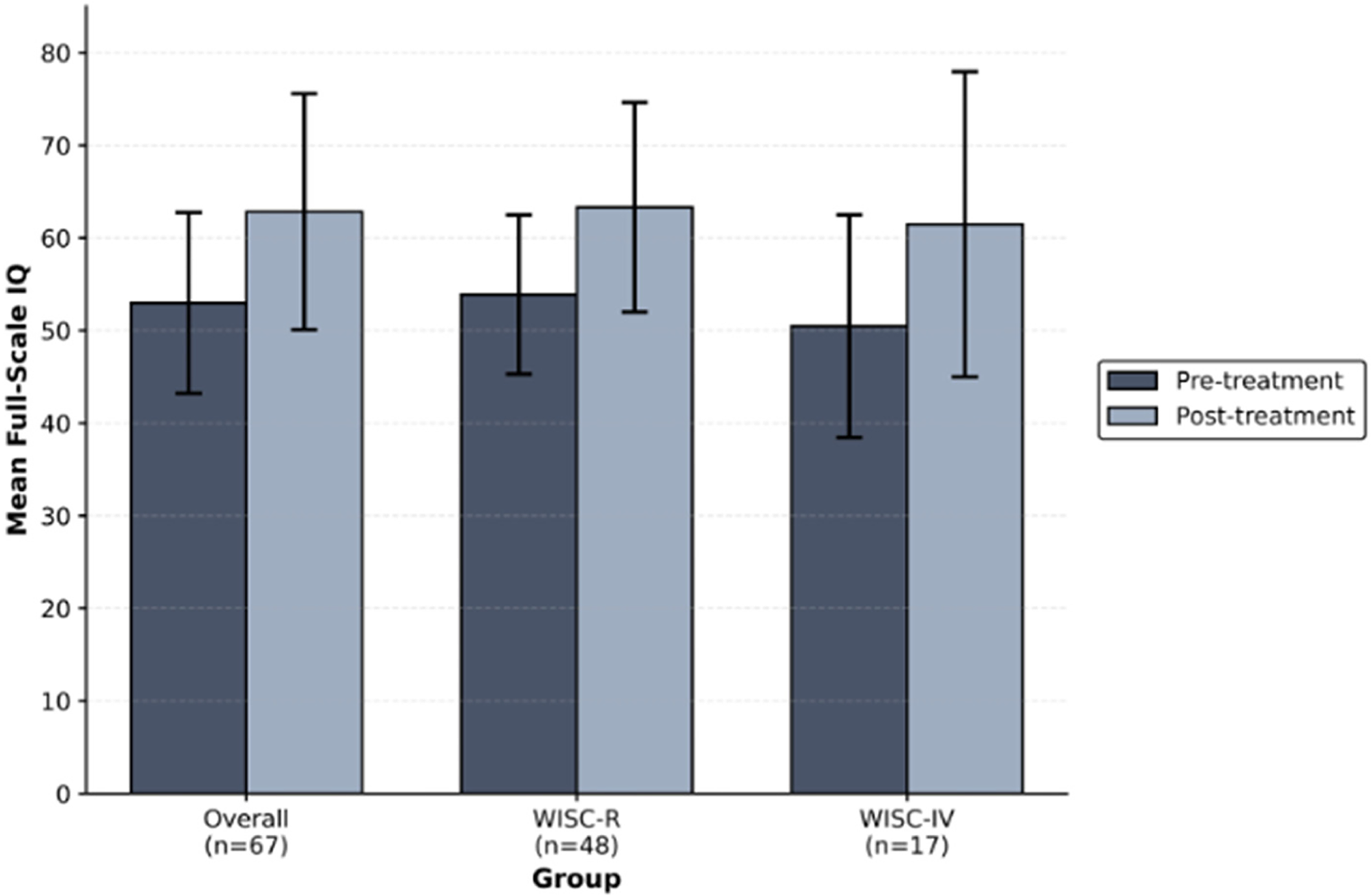
Mean full-scale IQ scores at baseline and post-treatment for overall sample and assessment subgroups. Note. Error bars represent ± 1 SD. WISC-R n = 48; WISC-IV n = 17. All groups showed significant improvements (P < .001).
WISC-R Outcomes
Participants assessed with the WISC-R (n = 48) demonstrated significant improvements from baseline to post-treatment. Mean full-scale IQ increased from M = 53.88 (SD = 8.60) to M = 63.31 (SD = 11.32), t(47) = 8.92, P < .001, d = 0.94. Both Verbal IQ, t(47) = 7.84, P < .001, and Performance IQ, t(47) = 8.21, P < .001, showed significant improvements. Clinically meaningful gains (≥ 6 IQ points, equivalent to 0.4 standard deviations 52 ; were achieved by 73% of participants in this subgroup (Figure 2).
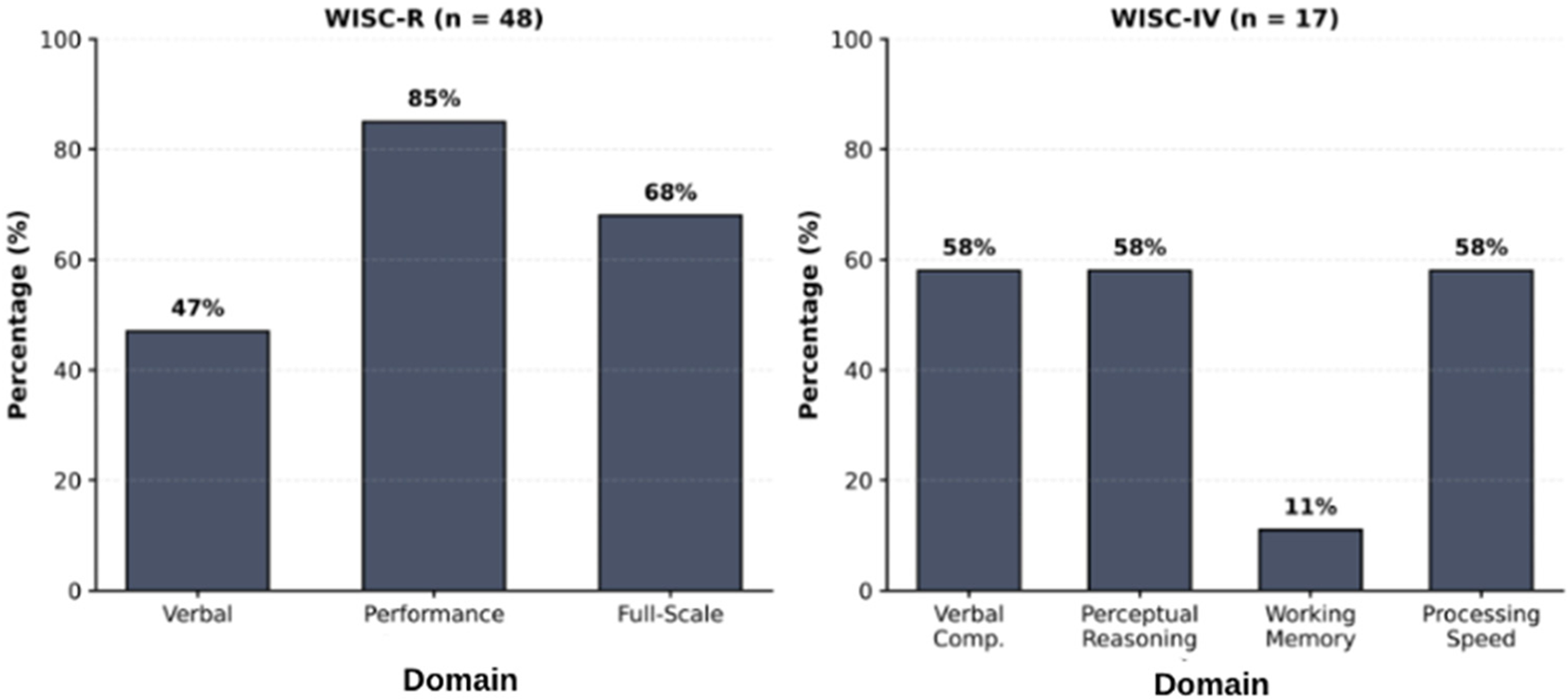
Proportion of participants achieving clinically meaningful IQ improvements (≥6 points) by assessment type and domain. Note. WISC-R n = 48; WISC-IV n = 17. Six-point threshold represents 0.4 SD, indicating clinically significant change. 52
WISC-IV Subscale Outcomes
Within the WISC-IV subgroup (n = 17), significant increases were observed across three of four cognitive indices (Table 1). Mean scores improved by 8–11 points across Verbal Comprehension, t(16) = 3.25, P = .005, d = 0.79; Perceptual Reasoning, t(16) = 2.97, P = .009, d = 0.72; and Processing Speed, t(16) = 3.23, P = .005, d = 0.78.
WISC-IV index Scores Before and After Neurofeedback.

Classification Changes by Severity Level
Neurofeedback shifted a substantial proportion of participants to higher intellectual functioning categories (Table 2). Among children with mild intellectual disability (IQ 55-69, n = 24), 70.8% achieved clinically meaningful change (≥ 6 IQ points), with 17 of 24 progressing to borderline intellectual functioning. This subgroup's mean IQ increased from M = 61.33 (SD = 5.87) to M = 72.58 (SD = 8.45), t(23) = 3.47, P = .002, d = 1.47, with corresponding improvements in Verbal (M = 59.87 to M = 68.45) and Performance (M = 67.54 to M = 81.70) domains.
Outcomes by Initial Severity Level.

Among those with moderate intellectual disability (IQ 40-54, n = 24), 41.7% showed clinically meaningful change, with 10 of 24 advancing to mild intellectual disability classification. This subgroup demonstrated a mean IQ increase from M = 46.00 (SD = 4.85) to M = 54.00 (SD = 7.21), t(23) = 2.48, P = .021, d = 1.23, with improvements in both Verbal (M = 46.54 to M = 51.25) and Performance (M = 52.33 to M = 63.00) scores.
Attention Performance Outcomes
Across both visual and auditory TOVA modalities, neurofeedback enhanced sustained attention and inhibitory control. Reaction times and variability decreased and commission and omission errors declined significantly (Figure 3).
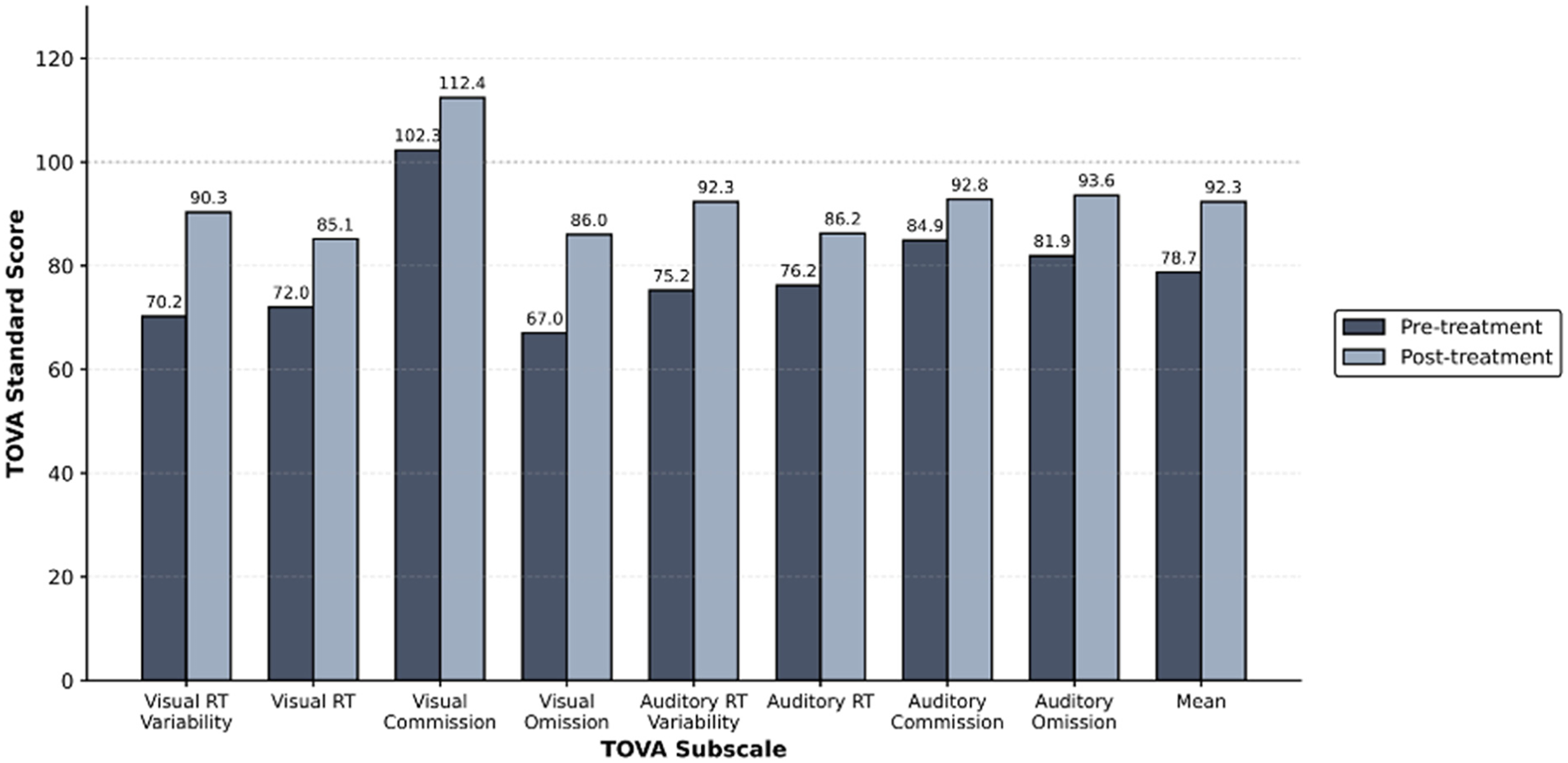
Pre-treatment and post-treatment TOVA performance across all measured parameters. Note. n = 67. TOVA uses age-normed standard scores (M = 100, SD = 15), where higher scores indicate better performance. All parameters showed significant improvements (P < .001). Overall mean TOVA performance increased from M = 78.73 to M = 92.33, approaching normative performance levels (≥85).
Default Mode Network Connectivity Changes
LORETA source localization analyses demonstrated significantly increased alpha-band (8–12 Hz) connectivity within the DMN following treatment, particularly in hubs of the posterior cingulate cortex, angular gyrus, and precuneus (Table 3). Left hemisphere regions showed the strongest effects.
Regions Showed Statistically Significant Increases in Alpha Band Connectivity. Left Hemisphere Activation Showed Consistently Stronger Effects Than Bilateral Measures.

QEEG Normalization Patterns
Coherence Changes
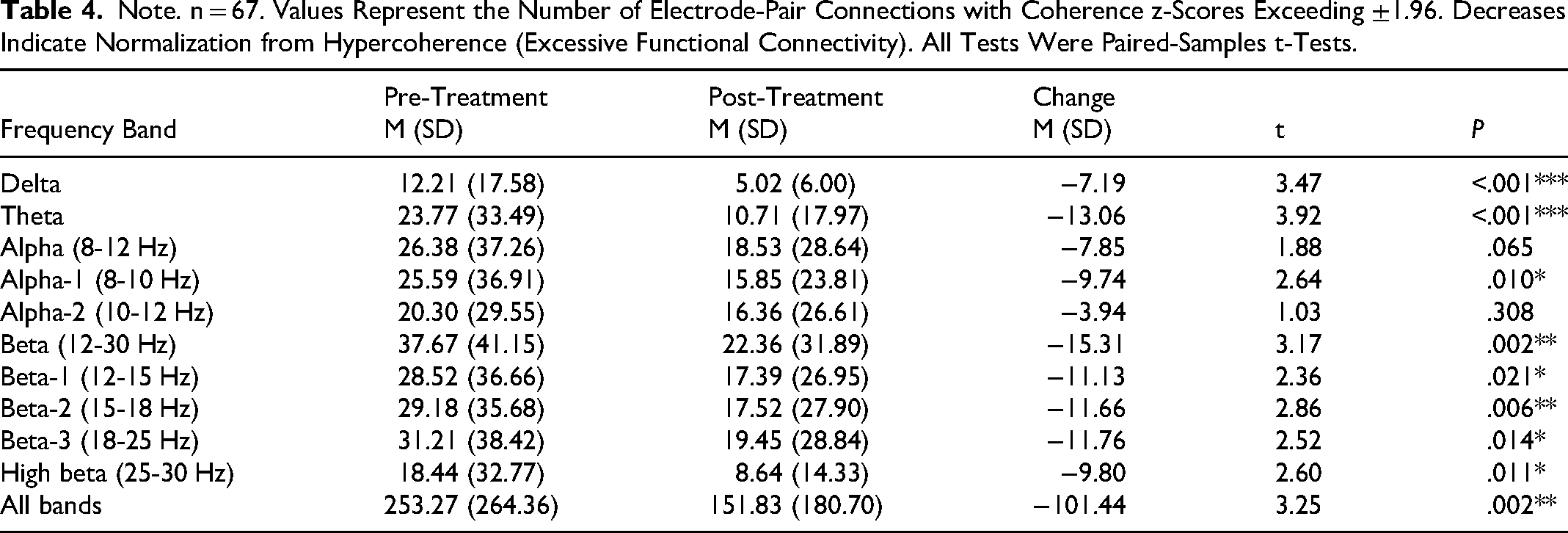
QEEG coherence analyses revealed significant reductions in hypercoherence across multiple frequency bands, indicating improved functional differentiation within neural networks (Table 4). Coherence represents the degree of phase synchronization between electrode pairs; higher z-scores indicate abnormal phase synchronization relative to normative databases. Reductions indicate improved temporal coordination of neural activity.
Note. n = 67. Values Represent the Number of Electrode-Pair Connections with Coherence z-Scores Exceeding ±1.96. Decreases Indicate Normalization from Hypercoherence (Excessive Functional Connectivity). All Tests Were Paired-Samples t-Tests.
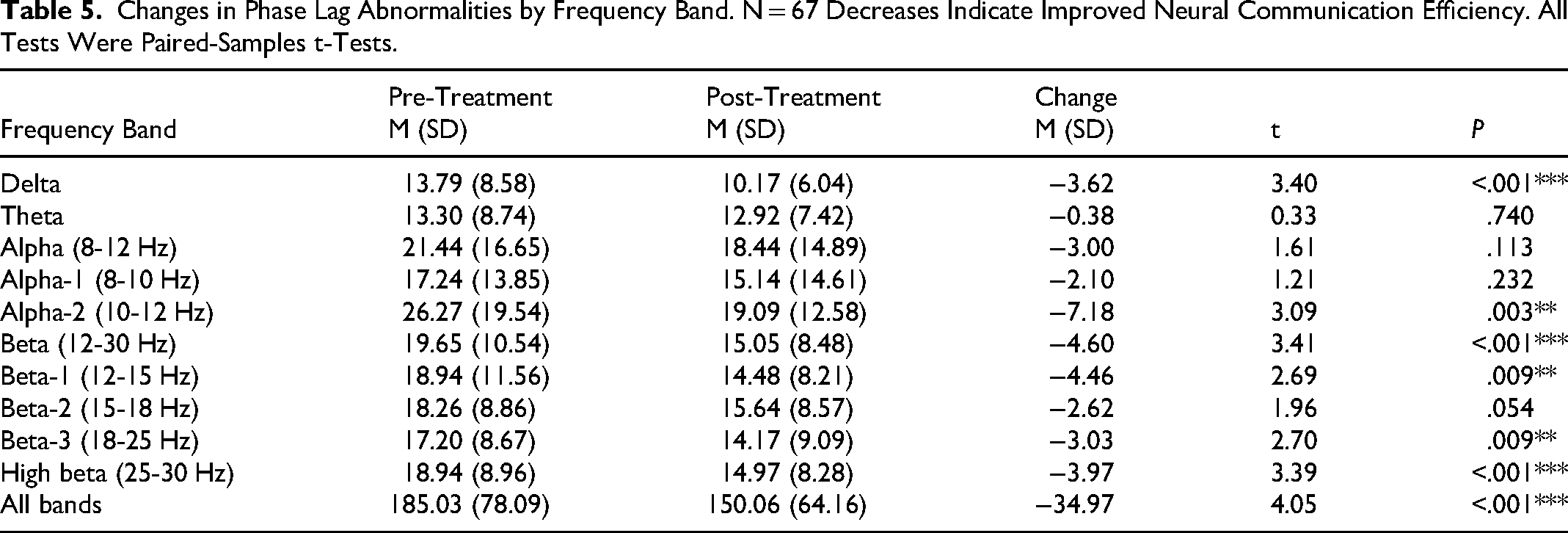
Phase lag Changes
Neurofeedback improved the timing of information transfer between brain regions, as reflected by reductions in abnormal phase lag across several frequencies (Table 5). Phase lag represents the temporal delay in neural communication between electrode pairs; abnormal values (z-scores exceeding ±1.96) indicate disrupted neural communication efficiency.
Changes in Phase Lag Abnormalities by Frequency Band. N = 67 Decreases Indicate Improved Neural Communication Efficiency. All Tests Were Paired-Samples t-Tests.
Absolute and Relative Power Changes
Neurofeedback normalized cortical activation by reducing excessive alpha power (Table 6). For alpha power metrics, positive z-scores indicate excess cortical activation relative to age-matched normative expectations. Other frequency bands did not exhibit significant changes.
Values Represent Mean z-Scores ± SD. Note. n = 67. All Tests Were Paired-Samples t-Tests.

Correlation Analyses
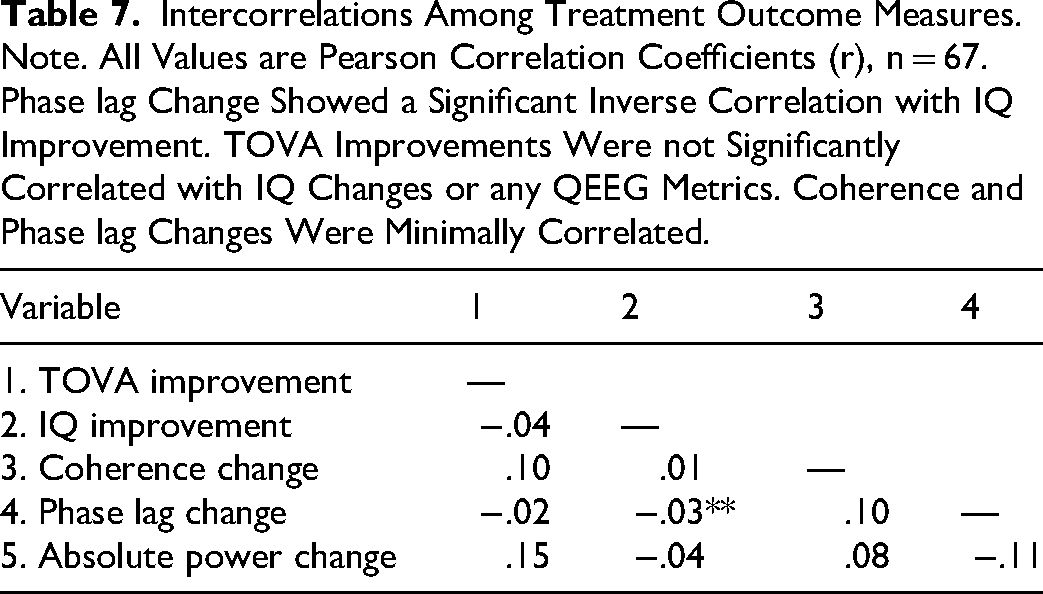
Reductions in phase lag abnormalities were significantly correlated with IQ improvement (r = −.033, P = .007), indicating that greater normalization of neural communication timing predicted larger cognitive gains. No significant correlations were observed between TOVA improvements and any QEEG metrics. Coherence and phase lag changes were minimally correlated (r = .10, P = .421), suggesting distinct mechanisms (Table 7).
Intercorrelations Among Treatment Outcome Measures. Note. All Values are Pearson Correlation Coefficients (r), n = 67. Phase lag Change Showed a Significant Inverse Correlation with IQ Improvement. TOVA Improvements Were not Significantly Correlated with IQ Changes or any QEEG Metrics. Coherence and Phase lag Changes Were Minimally Correlated.
Regression Analyses
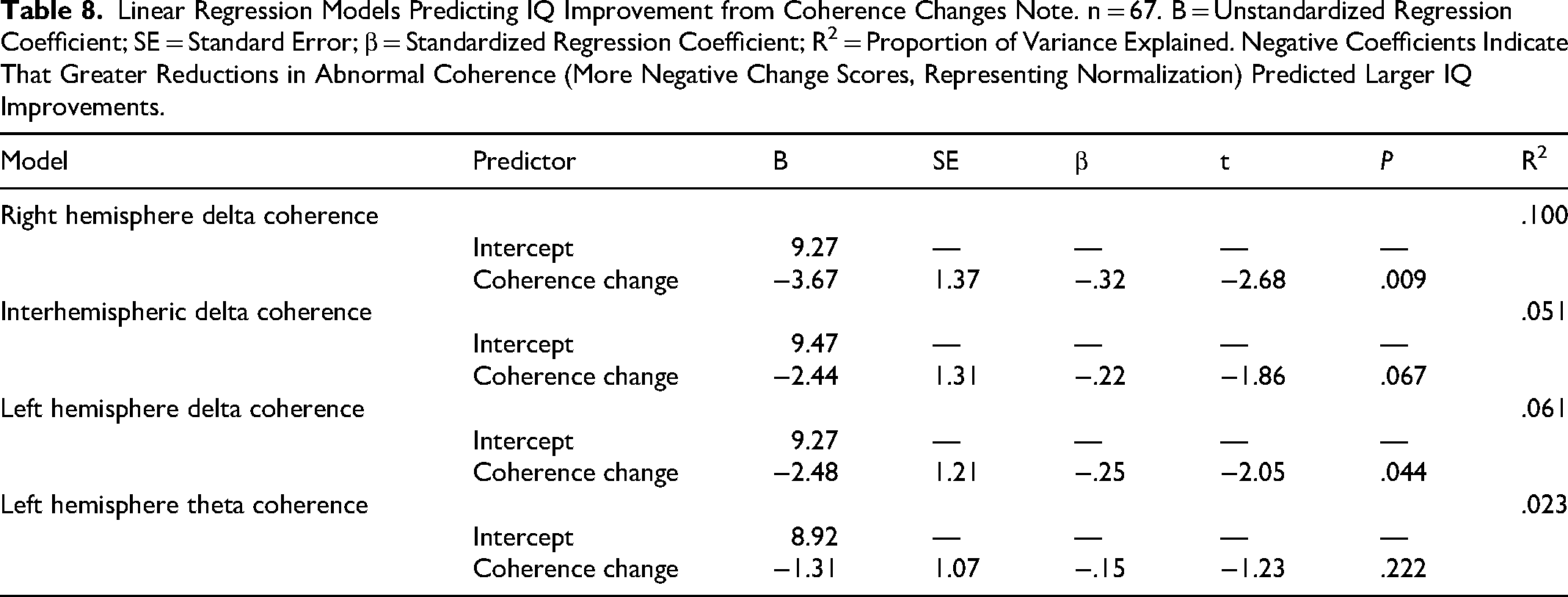
Multiple regression analyses indicated that decreases in right hemisphere delta coherence significantly predicted IQ improvement (R2 = .10, P = .009), with each unit decrease in abnormal coherence associated with a 3.67 point IQ gain (Table 8). In 86% of participants (n = 56), IQ gains met or exceeded the model's predicted improvement of 3.67 points, and three additional participants showed gains of 3 points. Left hemisphere delta coherence was also a significant predictor (R2 = .06, P = .044), while interhemispheric delta coherence showed a trend toward significance (P = .067). Overall, these models accounted for 6%–10% of the variance in IQ improvement.
Linear Regression Models Predicting IQ Improvement from Coherence Changes Note. n = 67. B = Unstandardized Regression Coefficient; SE = Standard Error; β = Standardized Regression Coefficient; R2 = Proportion of Variance Explained. Negative Coefficients Indicate That Greater Reductions in Abnormal Coherence (More Negative Change Scores, Representing Normalization) Predicted Larger IQ Improvements.
Group Comparisons
WISC-IV and WISC-R groups did not differ significantly in the magnitude of IQ change, TOVA change, or coherence change (Table 9), suggesting that improvements were robust across test versions.
Comparison of Treatment Outcomes Between WISC-R and WISC-IV Groups Improvement Scores Represent post-Treatment minus pre-Treatment Values. Independent Samples t-Tests Were Conducted to Compare Groups.

Discussion
Interpretation of Findings
This clinical case series demonstrates that QEEG guided neurofeedback can produce significant and clinically meaningful improvements in intellectual functioning for children and adolescents with ID. Mean IQ gains of approximately 10–11 points are substantially larger than the 1–5 point increases observed following cognitive enrichment 8 and counter the tendency for IQ to remain stable or decline over time in ID.29–31
In the present study, two-thirds of participants with intellectual disability showed an increase of at least six IQ points, a threshold considered clinically meaningful. This finding is consistent with earlier results reported by Sürmeli and Ertem, 39 in which 19 of 23 patients demonstrated IQ gains of six points or more.
Beyond the psychometric threshold, the clinical relevance of these gains is reinforced by parent-reported improvements in daily life functioning across multiple domains. In the area of speech and language, families described more coherent and logical sentence construction, meaningful question-asking, emerging signs of perspective-taking and empathy toward others, increased use of novel vocabulary, the cessation of repetitive questioning and repetitive speech, and the emergence of imaginative thinking and the capacity to daydream. Sleep regulation improved, with the establishment of regular sleep–wake schedules and the resolution of both nocturnal enuresis and bruxism. In the domain of behavior and aggression, caregivers reported marked reductions in aggressive behavior, decreases or full resolution of oppositional behavior, stubbornness, and tantrums, reduced or absent lying, improved rule-following, and the cessation of resistance to limits on screen time. Emotional regulation was characterized by reduced stress levels and a reduction in obsessive and compulsive features. Academic functioning improved through faster writing, reduced forgetfulness, the practice of bringing homework home and assuming responsibility for assignments, an increased awareness of school context (eg, the purpose of attending school and current grade level), improved comprehension of everyday events, and reduced restlessness in the classroom and at home, accompanied by decreased impulsivity. Social communication gains included increased self-esteem, awareness, and orientation; greater interaction with peers; remembering classmates’ names and beginning to identify them as “friends”; appropriate behavior in group settings (eg, adherence to communication and social-context norms); the assumption of household responsibilities; and the cessation of unprompted, context-inappropriate laughter. In the motor and self-care domain, caregivers reported improvements in fine and gross motor skills, the initiation of independent bathing, and advances in toileting skills. Changes in appetite and eating were also observed, including earlier satiety and a reduction in continuous eating, spontaneous refusal of sugary, starchy, or carbonated items even when offered by the family, and broader food acceptance beyond previously preferred sweet or starchy foods. Finally, somatic complaints such as constipation and headaches were reported to have resolved in some children. The convergence between the a priori IQ-based threshold and these observable, real-world changes across nine functional domains supports the interpretation that the cognitive gains were not artifacts of measurement but reflected functionally meaningful improvements in the children's everyday lives. Taken together, the magnitude of IQ gains, the proportion of participants exceeding the reliable change threshold, and the breadth of parent-reported functional improvements converge to support the conclusion that QEEG-guided neurofeedback produced changes that were not only statistically significant but also clinically meaningful in this sample.
Gains were observed across verbal, performance, and processing indices, suggesting broad cognitive benefits rather than narrow improvements on working memory tasks. The shift of many participants from moderate to mild ID underscores the potential functional impact of NF. Attention improvements were also robust; however, the lack of correlation between TOVA and IQ changes indicates that NF targets distinct cognitive systems. As attention improved independently of IQ, it is unlikely that improved attention alone explains the IQ gains. Instead, NF may enhance underlying neural efficiency.
Coherence and phase analyses support this interpretation; reductions in slow-wave coherence and phase lag imply more differentiated and efficient communication between brain regions. Increased alpha power within DMN hubs mirrors the developmental trajectory seen in typically developing children.53,54 These electrophysiological changes may reflect synaptic pruning, myelination, and strengthening of long-range connections which are mechanisms that are central to the parieto-frontal integration theory of intelligence. 7 Similarly, orbital and medial prefrontal regions and posterior cingulate have been found to correlate with alpha band activity and DMN connectivity in healthy adults. 55
Regression analyses suggest that decreases in slow-wave coherence predict IQ gains, with medium effect sizes in the right hemisphere (R2 = .10, P = .009) and left hemisphere (R2 = .06, P = .044). This aligns with the notion that excessive coherence (hypersynchrony) reflects poor differentiation and cognitive inflexibility56,57; reducing hypercoherence may enable more efficient information processing. Decreased delta power has also been positively correlated with IQ in other studies.12,58–60
Neuroplasticity and Intelligence
While the brain demonstrates clear neuroplastic capacity across the lifespan, this plasticity does not necessarily translate into durable increases in general intelligence as measured by full-scale IQ. Structural and functional brain changes can be induced through training, learning, or intervention—such as region specific gray matter alterations associated with skill acquisition 9 —yet these changes are typically task or domain-specific.
Consistent with this, intervention studies frequently report improvements in circumscribed cognitive subcomponents (eg, working memory, attention, or processing speed) rather than global IQ gains, and such effects are often constrained by small sample sizes and methodological heterogeneity, limiting replicability.31,32
Large-scale reviews of early intervention, compensatory education, behavioral, medical, and sensory-motor programs have repeatedly failed to demonstrate sustained increases in intelligence scores, particularly in populations with intellectual disability.32,61
Together, these findings suggest that while neuroplasticity supports functional adaptation and skill optimization, it should not be conflated with the capacity to meaningfully raise general intelligence, underscoring the importance of distinguishing neural change from psychometric change in the IQ–neuroplasticity debate.
Clinical Implications
The findings imply that QEEG guided NF is a promising non-pharmacologic intervention for ID. NF directly trains neural networks rather than relying on external stimulation, and it can be individualized based on each child's or adolescent's QEEG profile. Normalization of EEG patterns suggests that NF may facilitate neurodevelopmental maturation.
Improvements in IQ and attention may translate to better academic performance, self-care, and social functioning. The intervention is safe and well tolerated; participants did not receive concurrent psychotropic medications, and no adverse events were reported. Given the limited efficacy of existing interventions and the persistence of cognitive impairments in ID, NF offers a valuable addition to the therapeutic repertoire.
Limitations and Future Directions
Several limitations warrant caution when interpreting these findings.
Lack of Control Group: The study lacked a randomized or matched control group. Although it may be assumed that the observed improvements could be influenced by placebo effects, maturation, regression to the mean, or repeated exposure to testing procedures (TOVA and WISC), placebo effects generally subside within one week. Moreover, given that the WISC was re-administered at 6 and 12-month intervals, the improvements observed extend beyond these confounding factors and indicate a meaningful effect that merits serious consideration. Taken together, these findings warrant further investigation in a well-controlled study to establish causality and generalizability.
In our dataset, IQ scores measured at 6-month (WISC-R) and 12-month (WISC-IV) follow-up showed an increase rather than remaining stable or declining. This pattern is unlikely to be attributable to a placebo effect.
In contrast, our dataset demonstrates neither stability nor decline but rather a measurable increase in IQ scores across both assessments. These findings suggest that the commonly observed age-related limitation in cognitive trajectory may have been overcome in this cohort. Nevertheless, the magnitude of IQ gains and the normalization of EEG patterns observed here exceed those typically produced by practice alone.
62
Comparisons with previously published longitudinal IQ follow-up studies in individuals with ID suggest that the inclusion of a strict tau-control group may not be strictly necessary; nevertheless, we still recommend its inclusion for methodological rigor.
Sample Heterogeneity: The sample size was modest and clinically heterogeneous. Participants varied widely in etiological factors (eg, chromosomal anomalies, perinatal complications), severity of intellectual impairment, and baseline electrophysiological patterns. Such heterogeneity limits the generalizability of the results and makes it difficult to identify which training elements were most effective.
On the other hand, the fact that protocols were individualized supports the notion that using NF in this manner is most effective independent of etiology. Regardless of confounding factors that contribute to baseline variability in what is considered abnormal (eg, perinatal complications), the use of individually tailored z-score protocols centered on these variations is still associated with improvements in IQ. This finding strengthens the rationale for using NF, particularly in contexts where pharmacological treatments may be more strongly influenced by such factors.
Environmental and Educational Factors: Spitz
32
demonstrated that decades of efforts to increase IQ in developmentally delayed or culturally disadvantaged children—including early intervention programs (eg, Head Start), behavioral modification, medical and dietary approaches, and sensory-motor therapies—failed to produce meaningful or durable gains in intelligence. Against this historical backdrop, it is notable that, at the time of NF intervention, the children in the present context were not receiving special education services; this reduced the likelihood that observed cognitive changes could be attributed to concurrent compensatory education.
However, the absence of systematic monitoring of educational support, rehabilitation services, or changes in the home environment between assessments constitutes a methodological limitation, as these factors may act as unmeasured confounders. Nonetheless, given the extensive prior evidence that such interventions do not reliably elevate IQ, it is unlikely that nonspecific environmental or educational changes alone would account for substantial intelligence gains, underscoring the need for controlled studies to clarify the specific contribution of NF to observed outcomes.
Practice Effects: As long as testing was not repeated within 6 months, there is little chance of practice effect.
62
Moreover, in populations with intellectual disability, longitudinal data generally indicate that IQ scores remain stable or decline over 1 to 2 years, which makes the large gains reported here particularly unexpected.
61
Taken together, these considerations underscore the need for a controlled, long-term study to establish both the magnitude and durability of any treatment-related improvements.
Future research should address these limitations by employing randomized, controlled trial designs with sham neurofeedback or active comparator conditions (eg, cognitive training alone). Long-term follow-up, including assessments beyond 1 year, is necessary to determine the persistence of cognitive and neurophysiological changes.
Conclusion
QEEG guided neurofeedback produced significant improvements in IQ and attention among children with intellectual disability. The magnitude of cognitive gains and normalization of electrophysiological measures suggest that targeting brain network dynamics can meaningfully enhance intellectual functioning. These findings highlight NF as a promising adjunct to conventional therapies and support its further evaluation in controlled trials.
Footnotes
Ethical Considerations
This study is a retrospective clinical case series using de-identified data collected during routine clinical care. According to institutional policies, formal ethics committee approval was not required. The study was conducted in accordance with the principles of the Declaration of Helsinki. Informed consent for the use of clinical data for research and publication was obtained from all participants, and no identifiable patient information is disclosed.
Author Contributions
TS contributed to conception, contributed to acquisition and interpretation, drafted the manuscript, critically revised the manuscript, gave final approval, and agrees to be accountable for all aspects of work, ensuring integrity and accuracy. AE contributed to the interpretation of IQ test results. NCB contributed to data acquisition and statistical analysis. DC contributed to analysis and interpretation, drafted the manuscript, critically revised the manuscript, and agrees to be accountable for all aspects of work, ensuring integrity and accuracy. EE contributed to conception, contributed to analysis and interpretation, drafted the manuscript, critically revised the manuscript, and agrees to be accountable for all aspects of the work, ensuring integrity and accuracy. HJ contributed to the data analysis methods.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
De-identified data may be made available from the corresponding author upon reasonable request and subject to institutional review and applicable regulations.