
Abstract
Background
Isolated paroxysmal eye deviation in children is often considered a benign nonepileptic phenomenon. When epileptic in origin, gaze deviation is usually accompanied by visual symptoms, autonomic features, impaired awareness, or additional motor manifestations.
Case
We report a 6-year-old boy with frequent daily episodes of brief right upward eye deviation without impaired awareness, visual symptoms, head version, or other ictal features. Neurological and ophthalmological examinations, routine laboratory investigations, and brain magnetic resonance imaging were unremarkable. Video-electroencephalography demonstrated repetitive spike-wave discharges over the left occipital region, supporting an epileptic origin.
Results
Carbamazepine treatment markedly reduced episode frequency, and the spells resolved completely after dose adjustment during follow-up. Next-generation sequencing analysis of calcium channelopathy-related genes revealed no pathogenic variants.
Conclusions
This case highlights that isolated paroxysmal right upward eye deviation, even in the absence of other ictal features, may represent a focal preserved consciousness seizure rather than a benign ocular phenomenon. Early electroencephalographic evaluation is essential in children with frequent or atypical paroxysmal eye movements to avoid misdiagnosis and delayed treatment.
Introduction
Paroxysmal gaze deviation in childhood is often attributed to benign nonepileptic conditions, including paroxysmal tonic upgaze, tic disorders, opsoclonus-myoclonus syndrome, oculomotor apraxia, and CACNA1A-related disorders.1–4 Distinguishing epileptic from nonepileptic ocular events may be particularly challenging when eye deviation is the sole clinical feature. Video-electroencephalography (vEEG) is therefore critical in the evaluation of frequent or atypical paroxysmal eye movements. When gaze deviation is epileptic in origin, it is usually associated with the ipsilateral temporal, parietal, or occipital regions in seizures with impaired awareness, and with the contralateral frontal lobe in seizures with preserved awareness. 5 Bilateral frontal eye field activation may account for tonic upward gaze during generalized tonic-clonic seizures. 5 In childhood occipital epilepsy, gaze deviation may occur, but it is typically accompanied by visual symptoms or other ictal manifestations. 6
Here, we report a child with occipital lobe epilepsy in whom the only ictal semiology was brief recurrent right upward eye deviation associated with left occipital epileptiform discharges on vEEG. The case highlights an unusual electroclinical presentation of childhood occipital epilepsy that could easily be mistaken for a benign ocular phenomenon.
Case Presentation
A 6-year-old boy was referred for daily brief episodes of right-upward eye deviation (Figure 1). Awareness and responsiveness were preserved during the episodes, and the spells were not associated with visual symptoms, head version, autonomic features, or other observable motor manifestations. Pregnancy, birth history, and neurodevelopment were unremarkable. Neurological and ophthalmological examinations were normal between episodes. Routine laboratory and biochemical studies and brain magnetic resonance imaging were unremarkable. Interictal vEEG demonstrated repetitive spike-wave discharges over the left occipital region (Figure 2), supporting an epileptic origin. Carbamazepine treatment resulted in marked reduction in episode frequency, and the spells resolved completely after dose adjustment during follow-up. Next-generation sequencing analysis of calcium channelopathy-related genes revealed no pathogenic variants.

Still image captured during a paroxysmal episode showing brief right-upward gaze deviation without loss of awareness*.
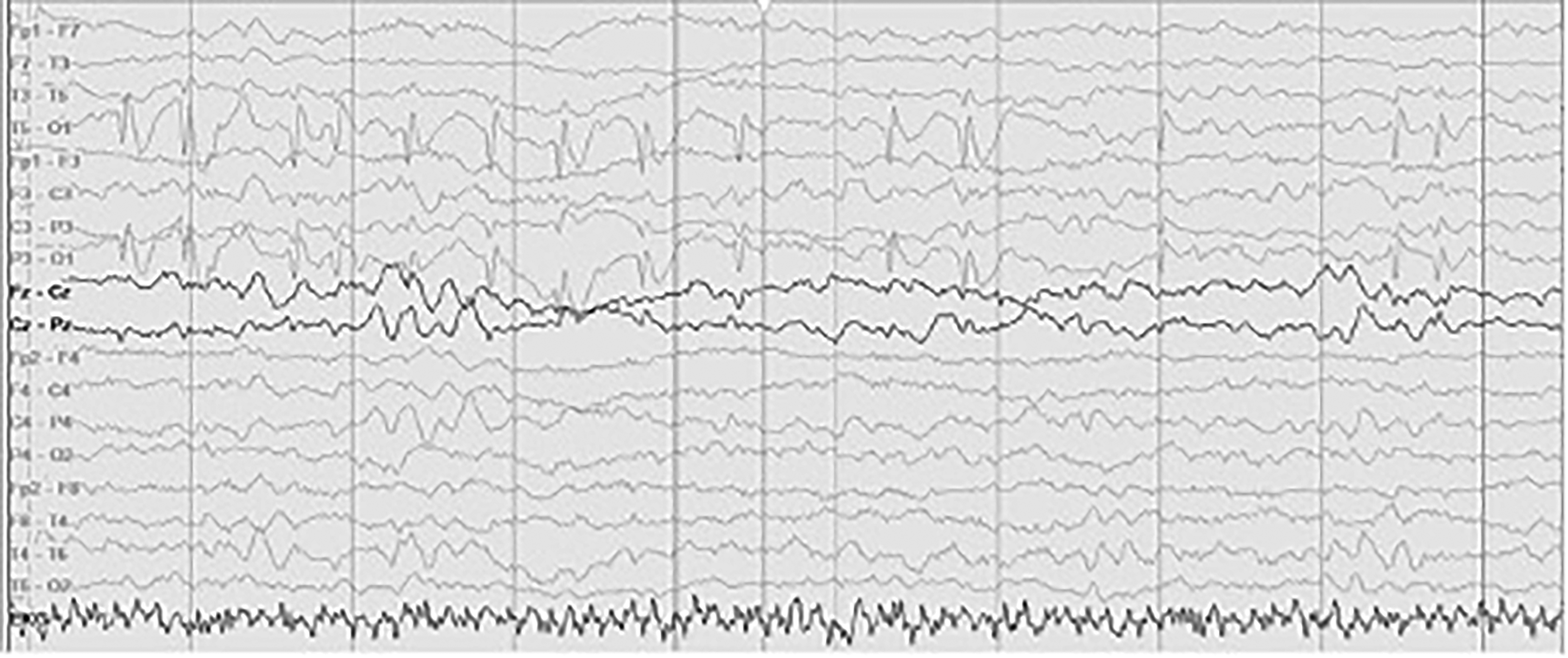
Interictal electroencephalogram demonstrating repetitive spike-wave discharges over the left occipital (O1) region, providing an electroclinical correlate for the episodes.
Written informed consent for publication of the clinical details and images was obtained from the patient's parents. Clinical images were de-identified using AI-based facial transformation software to protect privacy while preserving the relevant ocular findings.
Discussion
This case illustrates an unusual electroclinical presentation of childhood occipital epilepsy in which the sole ictal manifestation was recurrent brief right upward eye deviation with preserved consciousness. To our knowledge, only one previous report has described isolated paroxysmal eye deviation as the only manifestation of occipital lobe epilepsy, and that case involved horizontal deviation rather than upgaze. 7 The present case therefore expands the recognized spectrum of isolated ocular semiology in focal epilepsy.
Isolated paroxysmal eye deviation without additional symptoms is often considered a benign nonepileptic phenomenon in childhood.2–4 However, in the present case, the relatively late onset, high daily frequency, and absence of a typical benign paroxysmal tonic upgaze pattern prompted electroencephalographic evaluation. The recording demonstrated frequent left occipital spike-wave discharges, providing a clear electrophysiologic correlate for the clinical events. This was diagnostically important because the episodes lacked the visual phenomena, autonomic symptoms, or head version more commonly associated with occipital seizures.5,6
The neuroanatomical mechanism of tonic upward eye deviation in occipital epilepsy is likely network-based rather than purely local. Epileptic gaze deviation has been linked to cortical excitation of the frontal eye fields, temporal cortex, and parieto-occipital cortex, regions involved in saccadic control and connected through cortico-collicular projections to the brainstem oculomotor system. 8 This concept is further supported by recent structural network evidence showing that occipital lobe epilepsy is associated with altered global network organization and local network abnormalities extending beyond the occipital cortex to parietal, temporal, frontal, insular, cingulate, and perirolandic regions. 9 Therefore, the right-upward eye deviation in our patient is best interpreted as a network-mediated manifestation of a left occipital epileptic discharge, possibly involving propagation to posterior visual–oculomotor and parieto-occipital/frontal gaze networks, followed by recruitment of cortico-collicular and rostral midbrain supranuclear vertical gaze pathways.8–10 This interpretation also helps distinguish the episodes from benign paroxysmal tonic upgaze, in which prolonged or intermittent upgaze occurs without a consistent ictal occipital electroclinical correlate.
Current International League Against Epilepsy (ILAE) terminology emphasizes visual symptoms as a core feature of self-limited childhood occipital epilepsies. 6 In contrast, our patient had no visual complaints, autonomic symptoms, or other observable ictal features despite clear occipital epileptiform activity. According to the updated ILAE seizure classification, the episodes are best classified as focal preserved consciousness seizures with observable manifestations, with right upward eye deviation as the ictal semiology descriptor. 11 This makes the case diagnostically important, as the absence of visual symptoms could easily lead to misclassification as a nonepileptic ocular disorder. To date, only one case report has described paroxysmal gaze deviation as the sole manifestation of occipital lobe epilepsy, involving tonic leftward eye deviation with right occipital spike-wave discharges on vEEG. 7 In addition, paroxysmal tonic upgaze has been reported incidentally in a child with absence epilepsy.1
This case highlights that isolated paroxysmal upgaze may represent a focal epileptic phenomenon rather than a benign ocular event. In children with frequent or atypical paroxysmal eye deviations, early electroencephalographic evaluation is essential to avoid misdiagnosis and delayed treatment.
Footnotes
Acknowledgments
Not applicable.
Ethical Considerations
Ethical approval was not required for this single case report according to institutional policy.
Informed Consent
Written informed consent for publication of the case details and clinical photographs was obtained from the patient's parents. A copy of the consent is available upon request. The photographs and video frames were further anonymized using AI-based facial transformation software to ensure privacy while preserving clinically relevant eye movements.
Author Contributions
G.B. contributed to study conception, clinical data acquisition, EEG interpretation, and drafting of the manuscript. R.A. contributed to study design, interpretation and analysis of the clinical and electroencephalographic findings and critical revision of the manuscript. Both authors approved the final version of the manuscript and agree to be accountable for all aspects of the work.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability
Not applicable.