
Abstract
Introduction. Appendectomy is performed on almost 700 000 patients per year in the European Community, rendering it the most common acute surgical procedure. Since the introduction of laparoscopic surgery, there has been increased interest in carrying out procedures with fewer incisions and less ports. Materials and methods. After the inception of single-port access, it is possible to insert into the abdominal cavity multiple instruments through a single device. A total of 15 patients—mean age 22 years and mean body mass index 27 kg/m2—with acute appendicitis were included in this study. Results. Mean operative time was 35 minutes with no conversions. Local suction drain was needed in 2 patients. Mean hospital stay was less than 24 hours with no complications. Conclusion. Single-port suprapubic appendectomy is feasible and safe, and can allow a more direct vision of the operating field depending on the position of the appendix and presents good cosmetic and postoperative outcomes.
Keywords
Introduction
The first recorded appendectomy dates back to 1736. The surgical technique of open appendectomy had experimented few modifications since its first description by McBurney in 1884, until 1997, when de Kok reported successful laparoscopic appendectomy. 1 Single-port access (SPA) surgery, also known as single-incision laparoscopic surgery or one-port umbilical surgery, among others, is an advanced, minimally invasive surgical procedure in which the surgeon operates exclusively through a single access port—typically, through the navel. 2 Since the whole procedure is performed through the umbilicus, it does not leave any visible scar, unlike traditional laparoscopic surgery. Patients should benefit from less postoperative pain, less blood loss, faster recovery time, fewer complications, and better cosmetic results.3,4 As in other laparoscopic procedures, SPA surgery is performed under general anesthesia after insufflation of the peritoneal cavity. This technique has been used to carry out various surgical procedures—most of them belong to urologic and pediatric surgery—but it has also been applied to gastrointestinal 5 and gynecologic procedures. SPA surgery for the treatment of appendicitis was first performed at Dokuz Eylul Medical School, Izmir, Turkey, and first presented at the Annual Congress of Turkish Association of Pediatric Surgeons in October 2005.
We report a series of 15 single-port laparoscopic appendectomies performed using one suprapubic incision, in the pubic hairline limit, without any scars.
Surgical Technique
A total of 15 patients (9 women and 6 men), aged between 18 and 30 years (mean = 22 years), mean body mass index 27 kg/m2 (range = 19-33 kg/m2), were included in this study (Table 1). Physical examination, blood tests, and ultrasound studies were performed in all the patients prior to the surgery. The patients were placed in supine position, with the right side tilted to facilitate mobilization of the cecum.
Patient Characteristics and Operative Data. a
All values are median (range) unless stated otherwise.
After an urinary catheter was inserted, a suprapubic transverse Pfannenstiel incision measuring 1.5 cm was made and 1 R-Port (Advanced Surgical Concepts, Wicklow, Ireland) was introduced into the abdominal cavity using an open technique, thus allowing several instruments to be inserted through different cannulae of a single port (Figure 1).
The R-Port is introduced through the suprapubic incision.
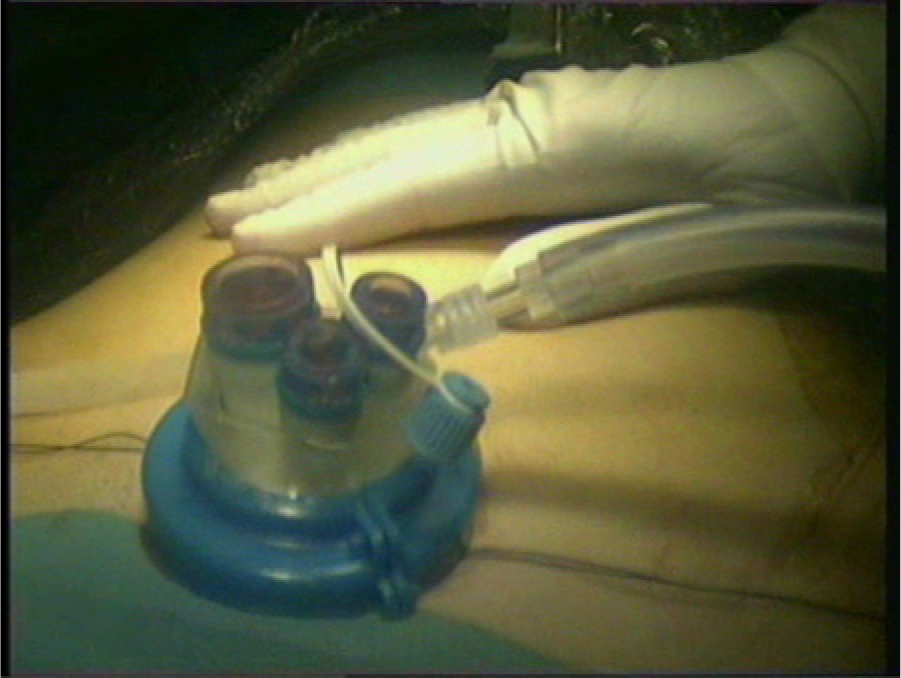
The R-Port consists of an external disc having 3 valves with a gel interface, which fits onto a double-layered plastic cylinder that can be used as the common channel or a single port.6,7 The plastic cylinder, when deployed, stays flush with the internal abdominal wall by an inner ring very much like a miniature hand port. Three separate valves allow insertion of one 12-mm, two 5-mm, or three 5-mm instruments simultaneously. A 5-mm 30° videolaparoscope was used, combined with 5-mm laparoscopic nonarticulated graspers and shears. After pneumoperitoneum was established, the patients were placed in Trendelenburg position (20°) to displace the small bowel away from the small pelvis. Additionally, the patients were tilted toward the left. With this additional maneuver, the small bowel lays apart from the operative field, the cecum hangs from its peritoneal attachments, and the base of the appendix appears just in front of the camera (Figure 2).
The base of the appendix is located in front of the camera.
The clearly inflamed appendixes were identified and loosened from surrounding tissues. The mesoappendixes were dissected after retraction of the appendix and divided using electrocautery and clips. The appendixes were then occluded and transected by a 30-mm stapling device (2.5 mm staples Endo GIA, Covidien, Mansfield, MA), as is the current technique at our institution.
Before appendix removal, hemostasia of the operative field was ensured. Placement of a suction drain through a different incision was necessary in 2 patients. Fascia was closed with nonabsorbable interrupted suture and skin with intradermic continuous suture.
Results
There were no intraoperative complications, neither additional transabdominal sutures nor suture traction through optional accesses were necessary in these procedures. Mean operative time was 35 minutes (range = 15-60), and the patients were discharged less than 24 hours after surgery without specific analgesia requirements (only on-request conventional analgesia). Cosmetic appearance of the incisions was very satisfactory (Figure 3).

The scar is practically invisible.
Discussion
Surgery through a single incision is an alternative to conventional laparoscopy and natural orifice transluminal endoscopic surgery. Various nomenclature and terminology have been used to describe similar surgical methods, such as SPA (single-port access), SPLS (single-port laparoscopic surgery), OPUS (one-port umbilical surgery) and, recently, LESS (laparoendoscopic single-site surgery).2,4 The LESS technique has been used to perform various surgeries such as appendectomy, cholecystectomy, hernias, nephrectomy, hysterectomy, adrenalectomy, colon resection, and others.5-7 Since the whole procedure is performed through the navel, it does not leave any visible scar, unlike conventional laparoscopy. Lack of space makes triangulation difficult, since surgical instruments remain nearly parallel during the process. 4 Because of its main role in laparoscopy, articulated or bent instruments would prevent the necessity to separate ports, allowing the creation of a small and solitary entry port into the abdominal cavity. Coordination between the surgeon and the camera assistant is absolutely essential.
Although initial publications of this technique appear in the early 1990s, its true clinical application has been accomplished only in the past 3 years. 3 Devices that allow the introduction of various instruments through them have been used in several surgical specialties. In gastrointestinal surgery, the first appendectomies were performed with assisted transumbilical technique,8,9 which means completing appendectomy in an extracorporeal way, thus taking advantage of the cecum as a static point of traction.
In 1997, Navarra et al 10 published the first laparoscopic cholecystectomy using a single umbilical port. Two years later, Piskun and Rajpal 11 described a similar technique using transabdominal sutures, and Besadrola et al 12 found less postoperative pain and less analgesia requirements in the first 24 hours after transumbilical cholecystectomy. Despite the fact that no studies have yet demonstrated it, those conclusions may be applied to LESS appendectomies too.
First cholecystectomies using devices such as Tri-Port were reported by Rao et al 7 in 2008. Although there are no data of its advantages against conventional laparoscopy, less incision and less morbidity may also be applied to LESS. 4 Cosmetic results are evident.
With the approach through a small Pfannenstiel incision and left tilt that we propose, a direct exposition of the appendix and its meso is probably guaranteed in most of the cases, avoiding the necessity to use a surgical instrument to move the small bowel. This is because both the appendix and the surgical instruments are in the same straight line.
In conventional laparoscopic approach, 3 ports are used without direct vision of the appendix, which has to be searched and grasped toward the ports. When LESS technique is used, through a single transumbilical incision, the problem is similar, as both the appendix and its meso are usually hidden by the interposed small bowel. This approach permits a direct view of the appendix, avoiding the problems described.
In addition, suprapubic approach allows immediate and easy visualization of the internal genital organs and Douglas pouch, avoiding small bowel mobilization required in conventional laparoscopy or transumbilical LESS.
Conclusions
This access to the abdominal cavity allows a different, direct and perhaps better surgical field, which facilitates the dissection and appendectomy procedure.
Cosmetic results are better,13-15 considering the fact that pubic hairline makes it a scarless surgery. We consider this surgery feasible and safe. Further studies must be developed to establish possible benefits for all patients.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.