
Abstract
Laparoscopic instruments that are newly inserted into trocars are initially outside the surgeon’s endoscopic field of view. This can make it difficult to accurately position the instrument at the operative site and presents a potential risk to patients since the tip of the instrument could potentially perforate organs and blood vessels while it is advanced blindly. To solve this problem, I have designed a trocar that incorporates a laser pointer to guide laparoscopic instruments while they are outside the endoscopic field of view. The laser dot is projected along the long axis of the trocar. This allows the surgeon to instantly determine the direction and target of the introduced instrument. Furthermore, the projected laser dot serves as evidence of an unobstructed path from the trocar to the target. This modification improves safety in laparoscopic surgery.
Introduction
Laparoscopy was initially invented as a diagnostic modality. 1 Subsequently, the development of specialized instruments made operative laparoscopy feasible. 2 Laparoscopic instruments are introduced into the peritoneal cavity via trocars. When a laparoscopic instrument is introduced into a trocar it initially remains outside the surgeon’s endoscopic field of view. Therefore, it can be difficult to correctly position a newly introduced laparoscopic instrument in the surgical field. This also presents a potential risk to patients since the tip of the introduced instrument could potentially perforate visceral organs and blood vessels while it is advanced blindly outside the endoscopic field of view. Here, I describe a modified trocar that simplifies the guidance of laparoscopic instruments while they are outside the endoscopic field of view.
Description of the Instrument
The modified trocar incorporates a laser diode, which projects a laser beam along the long axis of the trocar (Figure 1). The laser beam travels in a channel that is separate from the instrument port. This channel is enclosed by a glass cover and can be removed from the rest of the trocar for cleaning. The wavelength of the laser beam is 532 nm. This is within the green region of the visible optical spectrum. The power output of the laser diode is 5 mW. The laser diode is activated by a switch that is triggered when a laparoscopic instrument is introduced into the trocar and automatically deactivates 5 seconds later.
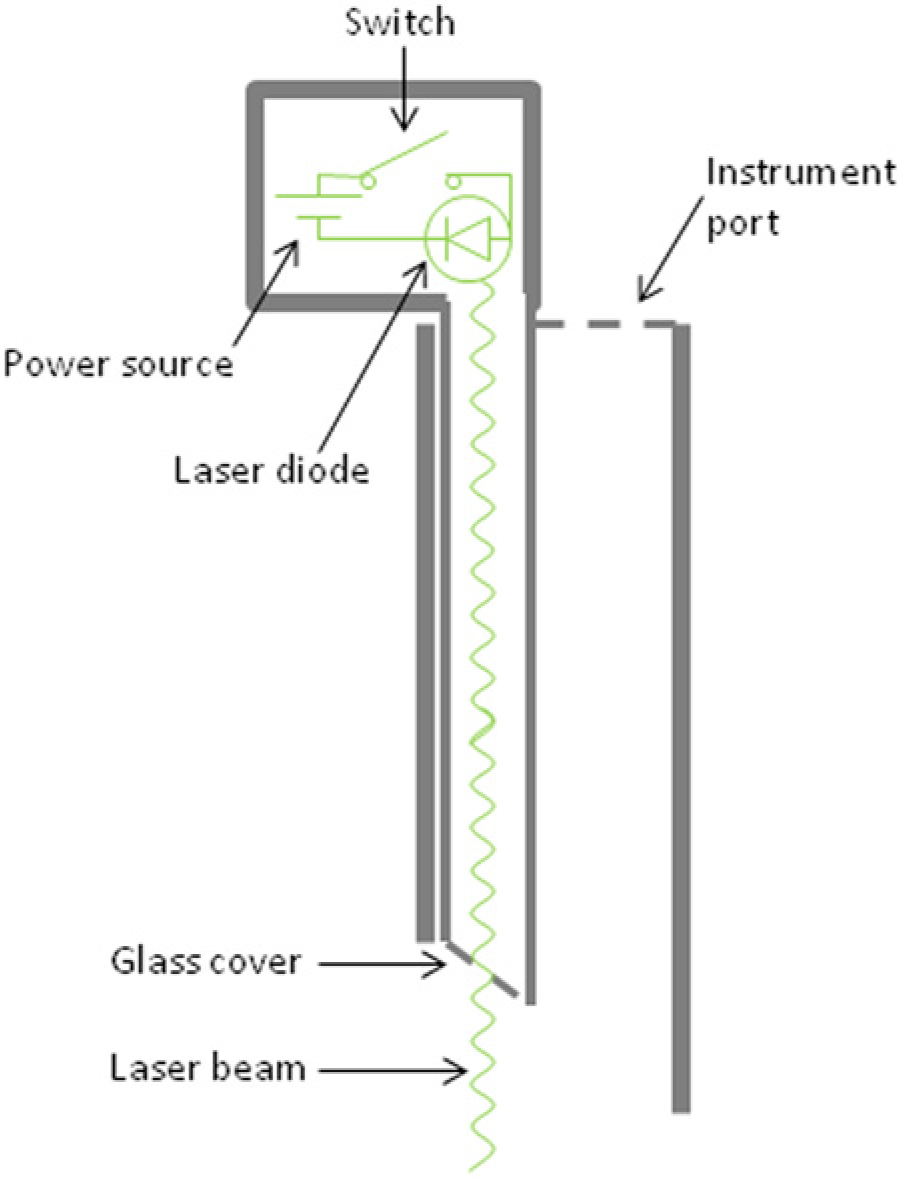
Construction diagram of the modified trocar. The laser diode is connected to a power source and projects a laser beam along a channel that is separate from the instrument port. This channel is enclosed by a glass cover and can be removed from the rest of the trocar for cleaning. The laser diode is activated by a switch when an instrument is introduced into the trocar and automatically deactivates 5 seconds later.
Indications
Iatrogenic injury of visceral organs or blood vessels is a serious complication of laparoscopic surgery. 3 This frequently occurs outside the surgeon’s endoscopic field of view.4,5 Surgical instruments that are newly introduced into trocars are initially located outside the endoscopic view. Therefore this represents a dangerous step in laparoscopy. Once inside the peritoneal cavity, surgical instruments are also occasionally maneuvered outside the endoscopic view. This also presents a risk for iatrogenic injury to organs and blood vessels, especially if the anatomy of the operative field is challenging and in the presence of peritoneal adhesions. To improve safety in laparoscopic surgery I have designed a trocar that incorporates a laser diode to guide laparoscopic instruments while they are outside the endoscopic view.
Laser Properties
Laser diodes are semiconductors that emit a low-powered laser beam. The color of the projected laser dot depends on the emitted wavelength and the brightness of the projected laser dot depends on the power output. Commercially available laser diodes emit light in the red, green, or blue regions of the visible optical spectrum. Our trocar employs a green diode with 532 nm wavelength. The wavelength of 532 nm was chosen based on a human factor study. Five surgeons were presented with a questionnaire to evaluate the optimal parameters for the laser diode. Each surgeon was asked to rank blue (445 nm), green (532 nm), and red (635 nm). All 5 surgeons ranked the red color as least favorable. Four surgeons ranked green as most favorable and 1 surgeon ranked blue as most favorable. The green color provides optimal contrast with intraperitoneal structures, including red blood and bluish veins.
The power output of visible lasers are classified by the American National Standards Institute as class 2 if the output is <1 mW, class 3A if the output is 1 to 5 mW, class 3B if the output is 5 to 500 mW, and class 4 if the output is >500 mW. The Food and Drug Administration stipulates that the maximum output for a demonstration laser product should fall in class 3A. The power output of the laser diode used for the described modified trocar is 5 mW, which corresponds to class 3A. This power output was also chosen based on a human factor study. Five surgeons were presented with a questionnaire to determine if they preferred a power output of 1 mW versus 5 mW. All 5 surgeons ranked a power output of 5 mW as superior. The higher power ensures that the projected laser dot is easily visible in the bright laparoscopic field. Furthermore, a power output of 5 mW is considered safe for sale to the general public without restriction in the United States.
Application
A switch activates the laser diode when a laparoscopic instrument is introduced into the trocar. The laser diode is automatically deactivated 5 seconds later to minimize unwanted distraction of the surgeon. Since the modified trocar is not yet approved for use by the Food and Drug Administration, we have extensively tested this instrument in a preclinical model. The projected laser dot is clearly visible on the laparoscopic screen. Surgeons may use the modified trocar just like a conventional trocar. In comparison with conventional trocars, the modified trocar has 2 major advantages. First, the projected laser dot serves as evidence of an unobstructed path from the trocar to the target. This improves the safety of introduction of new instruments into the peritoneal cavity since these instruments are potentially at risk of perforating visceral organs and blood vessels while they are advanced outside the endoscopic field of view. Second, the projected laser dot instantly indicates the target of an introduced instrument. This reliably guides the instruments while they are outside the endoscopic view and makes it easier to position new instruments in the surgical field.
However, our testing also revealed several potential disadvantages of the modified trocar. First, the projected laser dot can create distracting glare when the beam is scattered at an angle that reflects light rays directly back into the laparoscopic camera. Scattering can occur on other instruments or on the shiny surface of the peritoneum. I found that this problem is easily dealt with by slightly adjusting the angle of the trocar to move the position of the projected laser dot. Moreover, distraction to the surgeon is minimized by automatic deactivation of the laser diode 5 seconds after introduction of a new instrument. Second, the use of a laser diode increases the complexity of the trocar. Although the cost for the additional components is less than US$25, manufacturing the trocar requires changes in production lines. Furthermore, trocars incorporating a power source and a laser diode cannot be sterilized in a standard autoclave. Therefore, this trocar is a single-use instrument. All these factors result in higher cost than a conventional trocar. Consequently, this modified trocar might best be used selectively when difficult operative anatomy is expected, or to improve safety when teaching resident surgeons. Third, shining the laser dot directly into the eyes is potentially harmful. However, this is will not occur if the trocar is used correctly since the diode is only activated intraperitoneally. In any case, permanent retinal injury from a class 3A laser product is unlikely even after 15 minutes of direct retinal exposure. 6
Future Directions
Laser diodes are routinely used for nonsurgical applications outside the operating room. One of the most frequent applications of laser diodes outside the operating room is to guide the attention of other persons. The modified trocar could similarly be used to guide the attention of the members of the surgical team in the operating room. For example, the laser pointer could be used to identify anatomic structures to local or remote users. For this application, an additional switch would need to be incorporated that allows manual activation of the laser diode during the case.
Plans for the further development of the trocar also include an adjustable power output to regulate brightness. This would further serve to minimize distraction from glare.
Conclusion
The described laparoscopic trocar incorporates a laser diode to aid guidance of instruments while they are outside the laparoscopic field of view. This modification is intended to decrease the incidence of iatrogenic injury of visceral organs and blood vessels during laparoscopic surgery.
Footnotes
Acknowledgements
I gratefully acknowledge the suggestion of an automatic switch deactivating the laser diode after 5 seconds to minimize distraction by Dr Ali Tavakkoli. I also gratefully acknowledge the suggestion of a manual switch allowing the trocar to be used as a pointer during the case by an anonymous reviewer of Surgical Innovation. Finally I gratefully acknowledge the help from staff of the Neil and Elise Wallace STRATUS Center at Brigham and Women’s Hospital with preclinical testing of the device.
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.