
Abstract
Purpose. This study investigates the feasibility and potential utility of head-mounted displays for real-time wireless vital sign monitoring during surgical procedures. Methods. In this randomized controlled pilot study, surgery residents (n = 14) performed simulated bedside procedures with traditional vital sign monitors and were randomized to addition of vital sign streaming to Google Glass. Time to recognition of preprogrammed vital sign deterioration and frequency of traditional monitor use was recorded. User feedback was collected by electronic survey. Results. The experimental group spent 90% less time looking away from the procedural field to view traditional monitors during bronchoscopy (P = .003), and recognized critical desaturation 8.8 seconds earlier; the experimental group spent 71% (P = .01) less time looking away from the procedural field during thoracostomy, and recognized hypotension 10.5 seconds earlier. Trends toward earlier recognition of deterioration did not reach statistical significance. The majority of participants agreed that Google Glass increases situational awareness (64%), is helpful in monitoring vitals (86%), is easy to use (93%), and has potential to improve patient safety (85%). Conclusion. In this early feasibility study, use of streaming to Google Glass significantly decreased time looking away from procedural fields and resulted in a nonsignificant trend toward earlier recognition of vital sign deterioration. Vital sign streaming with Google Glass or similar platforms is feasible and may enhance procedural situational awareness.
Introduction
The Google Glass (Google, Mountain View, CA) head-mounted display platform allows users access to an array of digital media and functions, while performing a variety of daily tasks. 1 This is facilitated through a display in the peripheral vision of one visual field, similar to a rear view mirror, and a bone conduction audio system that provides single-user sound and voice recognition. The device is worn like a pair of glasses and includes voice activation, a high-definition camera, and wireless Internet connectivity. In the clinical setting, an interface between Google Glass and existing traditional patient monitoring devices holds the potential to provide clinical practitioners real-time access to resourceful data such as patient vital signs for improved situational awareness. However, prior studies published in the literature have not explored use of Google Glass for this function or demonstrated its feasibility.
Monitoring of patient vital signs is an essential element of every day in-hospital practice, and is central to the diagnosis and management of a spectrum of patient clinical conditions. 2 The assessment of temperature, heart rate, blood pressure, respiratory rate, and oxygen saturation level are among the most fundamental patient parameters that all medical personnel are trained to evaluate and review when initiating, adjusting, and/or concluding treatments. In the periprocedural setting, where conscious sedation may be utilized without the presence of an anesthesiologist (ie, angiograms, upper endoscopy, colonoscopy, bronchoscopy, or chest tube placement), the monitoring of vital signs becomes even more paramount to the safety of the patient. 3 Medications administered during conscious sedation can depress respiratory drive, decrease blood pressure, and potentially become life threatening if not appropriately monitored. Even when all vital parameters are merged onto one display system, this may be out of the operator’s direct visual field since the patient and operator are often confined to a fixed sterile area relative to the display devices and the operator is focused on specific steps of the procedure. Hence, to maintain a continuous view of these patient-specific monitoring parameters, the operator must frequently make a concerted effort to shift their attention away from the procedural field to monitor these variables.
Recent reports demonstrate that Google Glass technology can be applied to various medical applications, including facilitating hands-free communication, expediting workflow, and performing telemedicine in an emergency department setting. 4 Others have suggested Google Glass for use in pharmacies and for documentation during autopsies.5,6 One study investigated the use of the device in a pediatric surgery practice, with applications including hands-free documentation, billing code lookup, and Internet searches for unfamiliar medical terms. 7 Additionally, Google Glass has been proposed in a surgical setting to document airway assessment, to assist with ultrasound-guided central line placement, and to create a wearable surgical navigation system for image-guided cancer resection.8-10
In addition to already proposed uses in the literature, the ability of an electronic head-mounted wearable device like Google Glass to augment vital sign monitoring offers the potential to improve patient safety by preventing complications of conscious sedation during bedside procedures. However, feasibility and benefits to using this technology are yet to be demonstrated. In this early feasibility pilot study, we investigate the use of Google Glass to reliably facilitate real-time vital sign monitoring during procedures requiring conscious sedation in a standardized simulated surgical setting and explore the potential utility of this technology.
Material and Methods
Study Design
This study is a randomized controlled trial with crossover design completed at an academic medical center in April 2014. Study participants (n = 14) were postgraduate year (PGY)-1 to PGY-5 surgical residents in an Accreditation Council for Graduate Medical Education (ACGME)-accredited surgical training program. Subjects were recruited by email sent to all residents in a general surgery residency program and were eligible to participate if they were a categorical general surgery resident, a surgical subspecialty resident, or a preliminary general surgery resident. The study was conducted as part of a residency skills session held in the Goodman Surgical Education Center.
Each subject participated in 2 standardized preprogrammed simulation scenarios involving bedside surgical procedures on a high-fidelity computer controlled mannequin in the simulation center. Participants were randomized to either the control or experimental group for the first scenario. The control group relied on traditional monitoring of patient vital signs using a standard bedside digital monitor. The experimental group wore Google Glass with continuous wireless streaming of patient vital signs to the device in addition to the standard bedside vital sign monitor. Subjects in the control group for the first scenario then crossed over to the experimental group for the second scenario, and vice-versa. Therefore, subjects served as a control subject for one scenario and an experimental subject for the other scenario. Experimental subjects received training with Google Glass 5 minutes before starting their scenario. User feedback was collected from subjects by electronic survey immediately following completion of the scenarios. Institutional review board approval was obtained from Stanford University for use of these data for research purposes.
Wireless Vital Sign Streaming to Google Glass
The mannequin’s vital signs were streamed from a standard display monitor to the mobile, head-mounted Google Glass device using VitalVideo software (Vital Enterprises, Inc, San Francisco, CA). Using this system, the video output from the vital sign display monitor is digitally encoded and broadcast from a private wireless access point. Vital sign data streamed to Google Glass was a replicate miniaturized version of a traditional vital screen monitor, and included arterial line blood pressure, heart rate and rhythm, pulse oximetry, and respiratory rate. While wearing Google Glass, operators viewed in the upper right-hand corner of the visual field a reproduced image of the mannequin’s General Electric Patient Monitoring System vital sign monitor (Figure 1). Wireless streaming was near real-time with millisecond latency.

Wireless streaming of vital signs to Google Glass in a simulation setting.
Setting
The study was performed in a simulation suite consisting of a simulated patient care area with high-fidelity computer-operated mannequin (Laerdal SimMan 3G), digital vital sign monitor, Mayo instrument stand, and virtual reality bronchoscopy machine (CAE Healthcare EndoVR). The SimMan 3G mannequin simulates real-time human physiologic parameters, including audible cardiopulmonary sounds and palpable pulses. Procedures can be performed on the mannequin, including but not limited to, endotracheal intubation and chest tube insertion. The SimMan 3G software additionally allows for creation of preprogrammed, standardized simulation scenarios. The CAE Healthcare EndoVR machine, which was positioned adjacent to the head of the mannequin, allows an operator to perform a virtual bronchoscopy and administer conscious sedation (Figure 1). Traditional vital sign monitors displaying the mannequin’s vital signs (heart rate, blood pressure, oxygen saturation, and respiratory rate) were available 90° from the procedural field for all subjects. Blood pressure was displayed continuously as arterial line pressure. Positioning of the mannequin, monitor, equipment tray, and virtual reality bronchoscopy machine was kept constant for all participants and all subjects completed the scenarios on the same day. In the simulation center, an affiliated control room behind a 2-way mirror housed a touch-screen control panel, voice control system, computer with Laerdal SimMan 3G software, and remotely operated audiovisual capture equipment. Simulation center staff and 2 study investigators were present in the control room during all scenarios to ensure proper deployment and recording. All scenarios were digitally recorded from two camera angles using SimCapture software (B-Line Medical, Washington, DC). Immediately prior to participating in each scenario, those subjects randomized to the experimental group were fitted with Google Glass to optimize the display view and received training on how to operate the device by a technical expert. VitalVideo software was tested with each participant in the experimental group prior to entering the scenario to ensure the vital sign screen was clear, readable, and appeared in the visual field.
Scenarios
Scenarios were selected to be representative of bedside procedures performed by surgeons and surgical trainees that commonly require conscious sedation without the presence of an anesthesiologist. Scenarios were designed to represent fictional patients in the trauma and critical care settings. All subjects were provided an introduction to the virtual reality bronchoscopy machine and SimMan 3G mannequin prior to the start of the scenarios, including the ability to auscultate cardiopulmonary sounds, intubate the patient, administer medications or intravenous fluids, and place a thoracostomy tube.
Scenario 1 involved thoracostomy tube placement using a high-fidelity computer-controlled mannequin (Laerdal SimMan 3G) described above. The simulated patient was described as a 62-year-old male status post high-speed motor vehicle collision with multiple left-sided rib fractures, small left apical pneumothorax, pulmonary contusion, and Grade 3 splenic laceration. Participants were provided with baseline laboratory values and vital signs. Baseline systolic blood pressure on entering the scenario was 120 mm Hg. Participants were asked to proceed with left chest tube placement under conscious sedation following sterile technique. Subjects were provided with a sterile thoracostomy tray, chest tube, gowns, gloves, and drapes, all of which were identical to those supplied by the academic medical center for clinical use. Using Laerdal SimMan 3G software, the scenario was preprogrammed to include a continuous pre-programmed decline in blood pressure from systolic blood pressure of 120 to 58 mm Hg beginning 2 minutes after the start of the scenario.
Scenario 2 involved bronchoscopy using a hybrid platform with virtual reality bronchoscopy machine (CAE Healthcare EndoVR) and high-fidelity computer controlled mannequin (Laerdal SimMan 3G). The virtual reality bronchoscopy machine was placed at the head of the mannequin, 90° from the vital sign monitor. The simulated patient was a 55-year-old male in the surgical intensive care unit status post left hepatectomy for hepatocellular carcinoma with postoperative course complicated by myocardial infarction. Participants were told that the patient was requiring 6-L nasal cannula to maintain oxygen saturation and chest radiograph on morning rounds revealed opacification of the left upper lung field suspicious for a mucus plug. Study participants were instructed to perform a bedside bronchoscopy using the virtual reality bronchoscopy machine. Using Laerdal SimMan 3G software, the scenario was preprogrammed to include a continuous decline in oxygen saturation from 95% to 70% beginning one minute after the start of the scenario. When the oxygen saturation reached 70%, the heart rhythm was programmed to enter sustained ventricular tachycardia.
In both scenarios, subjects were instructed to monitor the vital signs of the patient while performing the procedure and to verbalize their findings. Subjects were not aware that preprogrammed vital sign deterioration would occur. In both scenarios, the preprogramed vital sign deteriorations were timed to occur well before completion of the bedside procedure. An actor playing the role of a nurse confederate was present in the simulation suite during the scenarios, seated at the foot of the patient’s bed with their back to the vital sign monitor. An additional actor simulated the voice of the patient from the adjacent control room via overhead intercom to respond to participant’s questions. Each scenario was preprogrammed to end after 5 minutes.
Data Collection
Objective outcome measures included time to recognition of hypotension (scenario 1), blood pressure at time of recognition of hypotension (scenario 1), time to recognition of desaturation (scenario 2), oxygen saturation at time of recognition of desaturation (scenario 2), number of glances at traditional monitor, and time spent looking away from the procedural field to view the traditional vital sign monitor. All scenarios for all subjects were video recorded in the simulation suite using ceiling-mounted cameras and SimCapture software (B-Line Medical, Washington, DC). Time to recognition of vital sign deterioration was defined as the number of seconds from the time of preprogrammed vital sign deterioration to initiation of verbal recognition by the study participant. Two sets of investigators independently reviewed video recordings to confirm time and vital sign metrics.
Demographic data and user feedback were collected by electronic survey, which was completed by each subject after participation in the scenarios. Participants were asked to respond to a series of statements on a 4-point Likert-type scale (“strongly disagree,” “disagree,” “agree,” “strongly agree”). Statements included in the survey queried subjects about topics such as ease of use, situational awareness, ability to perform task, potential to improve patient care, potential to replace traditional vital sign monitors, and likelihood they would consider using Google Glass in their future practice. The survey also qualitatively collected participants’ overall impressions of using Google Glass in this setting.
Statistical Analysis
Mean and standard deviation were calculated for all continuous variables. Gender, PGY-level, specialty, prior Google Glass use, and user feedback data are reported as percentages. For time to recognition of vital sign abnormality and vital sign metrics at time of recognition (Tables 2 and 3), the average value recorded by the 2 independent reviewers was calculated and used for analysis. Absolute effect size was calculated as the difference between the group means. Effect size was calculated as Cohen’s d. Student’s t test was used to determine whether there was a statistically significant difference in continuous variables between the control and experimental groups. Chi-square test was performed to assess for statistical significance of proportions. A P value ≤.05 was considered statistically significant. Statistical analyses were performed using Microsoft Excel.
Results
Demographics
Demographic data are shown in Table 1. The mean age of the study population was 29.7 years, with level of training ranging from PGY-1 to PGY-5. The majority of study participants were categorical (71%) or preliminary (14%) general surgery residents. The specialties of the remaining participants (15%) included plastic surgery and cardiothoracic surgery. The majority of the participants were male (64%). There were no statistically significant differences in demographics observed between those randomized to the control group versus experimental group (group A vs group B). The majority (79%) of subjects had never used Google Glass prior to participation in the study, with the remaining participants (21%) reporting having used Google Glass once prior (data not shown). No subjects reported using Google Glass on a regular basis.
Demographics of Study Participants.
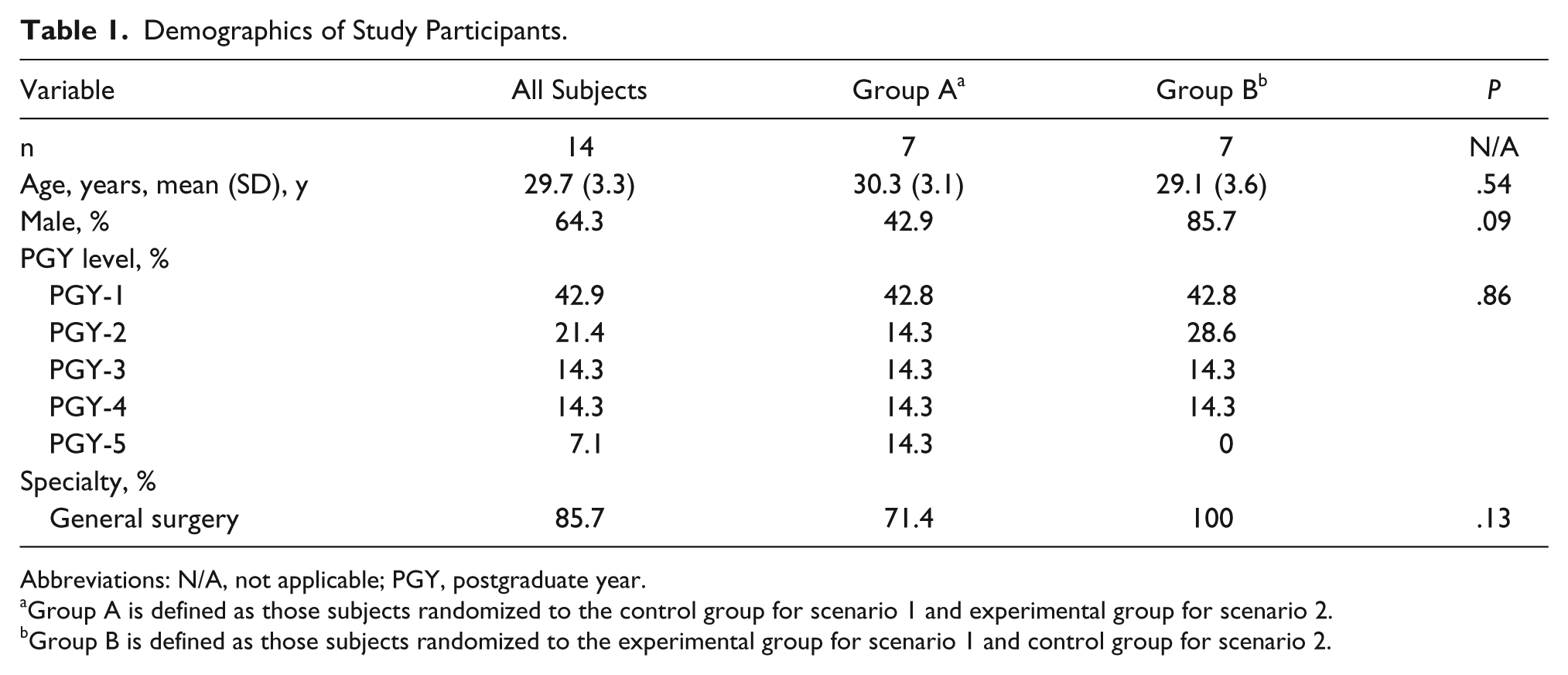
Abbreviations: N/A, not applicable; PGY, postgraduate year.
Group A is defined as those subjects randomized to the control group for scenario 1 and experimental group for scenario 2.
Group B is defined as those subjects randomized to the experimental group for scenario 1 and control group for scenario 2.
Recognition of Vital Sign Deterioration
Scenario 1: Chest Tube Placement
While performing bedside thoracostomy tube placement, the experimental group recognized severe hypotension 10.1 seconds earlier than the control group (31.8 and 41.9 seconds, P > .05) (Table 2). Hypotension was less severe at time of recognition in the experimental group compared with the control group (67.6 and 59.9 mm Hg, P > .05); these findings did not reach statistical significance. The experimental group utilized traditional vital sign monitors less frequently (P = .04) and spent 71% (P = .01) less total time looking away from the procedural field to view the traditional vital sign monitors compared with the control group.
Recognition of Hypotension in Scenario 1.
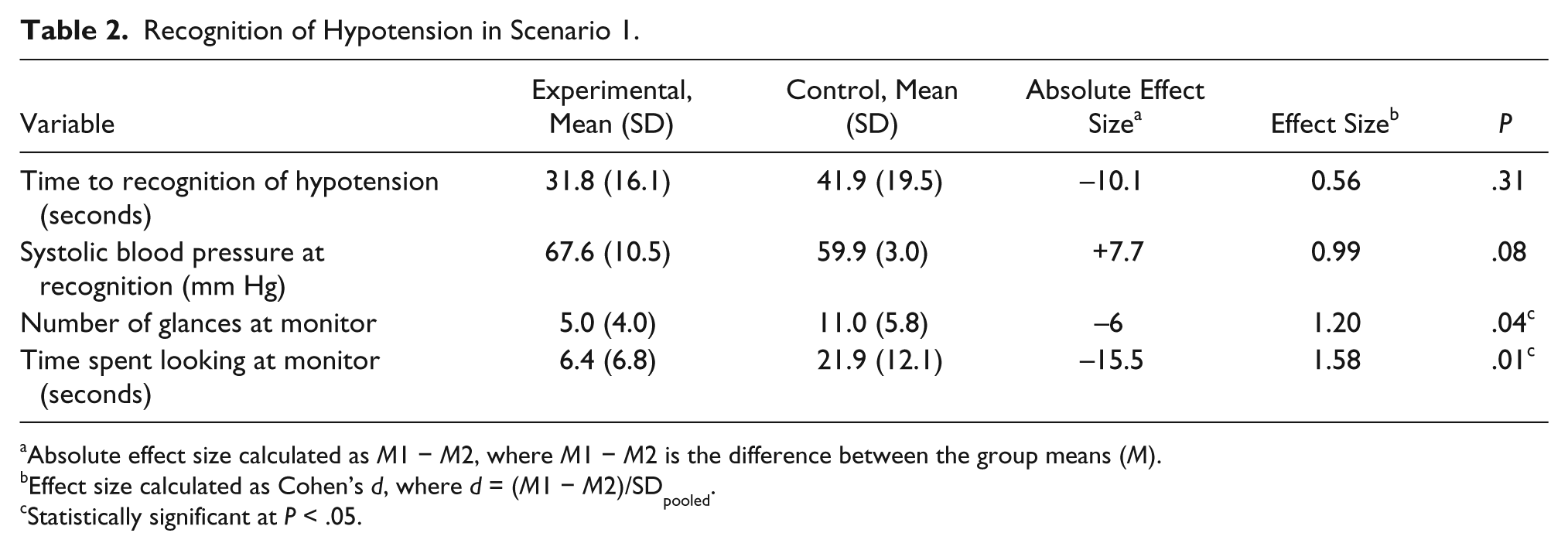
Absolute effect size calculated as M1 − M2, where M1 − M2 is the difference between the group means (M).
Effect size calculated as Cohen’s d, where d = (M1 − M2)/SDpooled.
Statistically significant at P < .05.
Scenario 2: Bronchoscopy
Wireless streaming of vital signs to Google Glass resulted in a nonsignificant trend toward earlier recognition of critical desaturation and progression to ventricular tachycardia, with the experimental group recognizing critical desaturation 8.8 seconds earlier than the control group (64.6 vs 73.4 seconds, P > .05) (Table 3). Similar to findings in scenario 1, the experimental group utilized traditional vital sign monitors less frequently (P = .001) and spent significantly less total time looking away from the procedural field to view the monitor (P = .003) compared with the control group. There was no statistical difference in oxygen saturation at time of recognition between the control and experimental groups.
Recognition of Desaturation in Scenario 2.
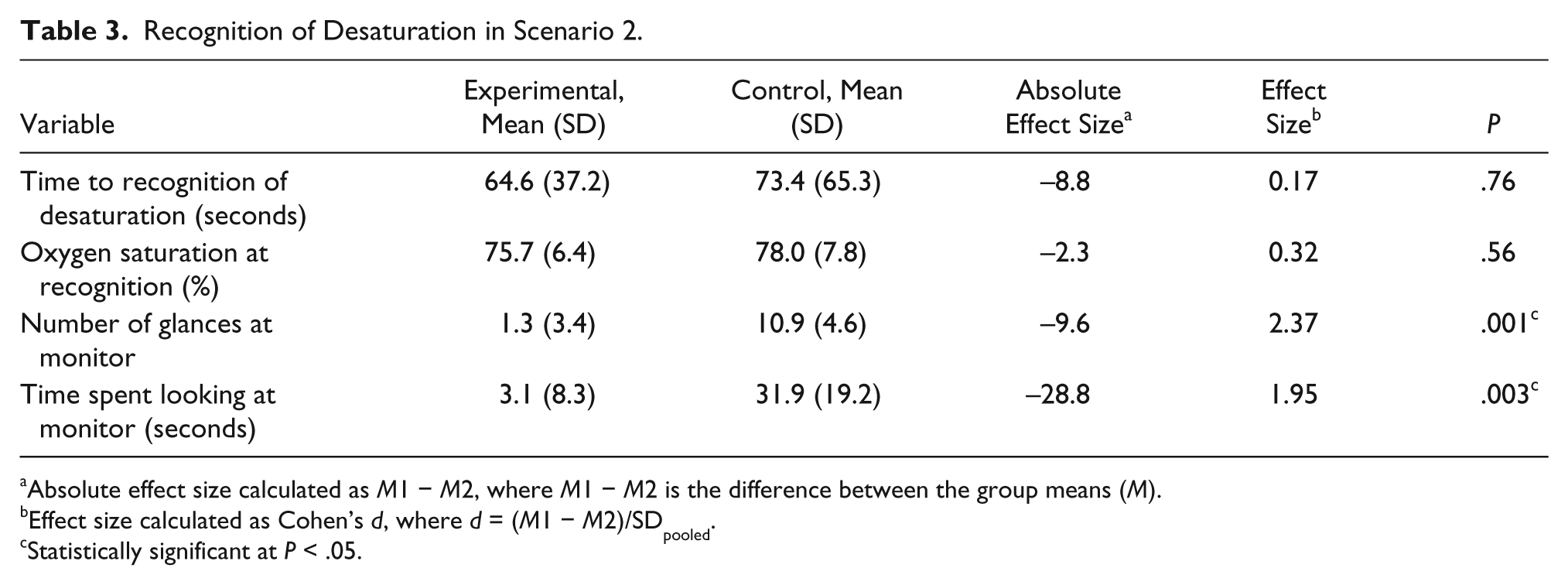
Absolute effect size calculated as M1 − M2, where M1 − M2 is the difference between the group means (M).
Effect size calculated as Cohen’s d, where d = (M1 − M2)/SDpooled.
Statistically significant at P < .05.
User Feedback
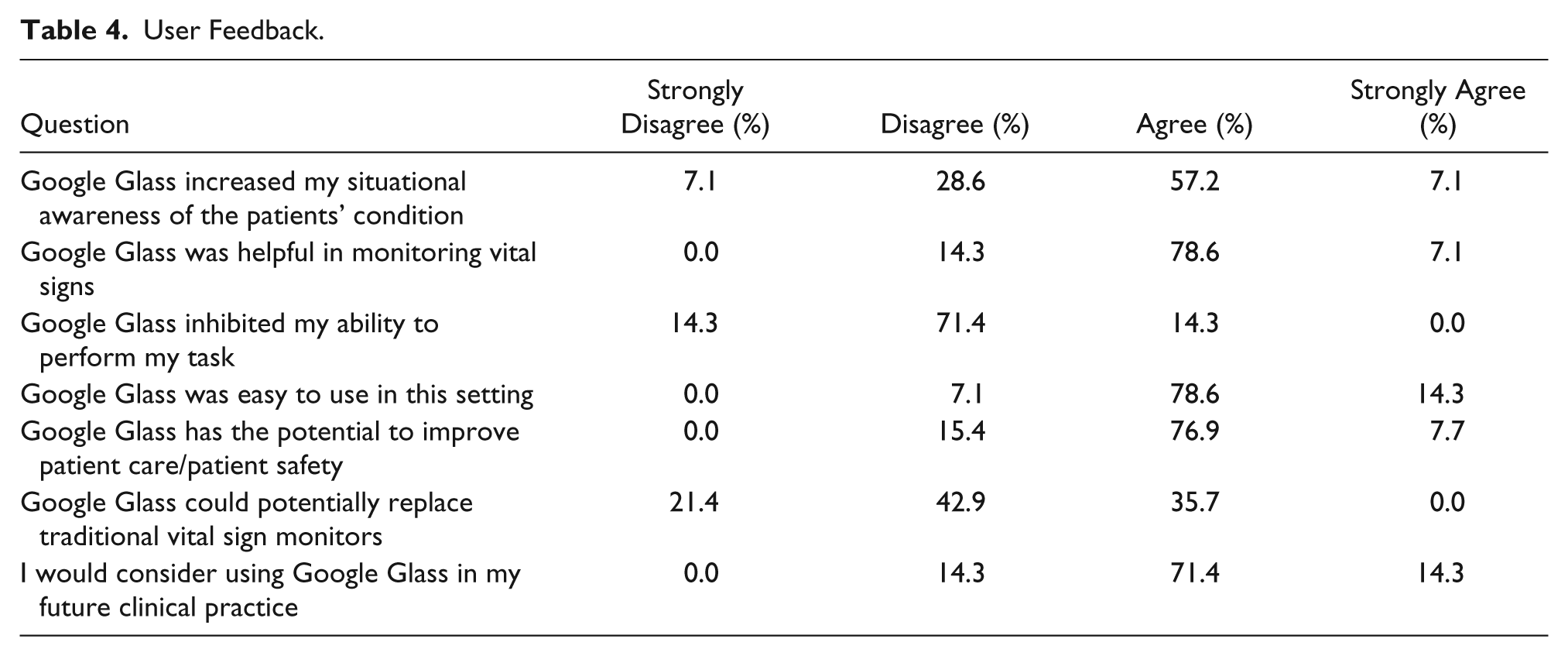
All participants (n = 14) completed the online survey following completion of the study. The majority “agreed” or “strongly agreed” that Google Glass increased their situational awareness (64%), was helpful in monitoring vital signs (86%), and was easy to use in the procedural setting (93%). Participants felt that wireless vital sign streaming with Google Glass has the potential to improve patient safety (85%). When asked if Google Glass inhibited their ability to perform their task, the majority (86%) disagreed. Although participants did not feel that Google Glass could replace traditional vital sign monitors, most participants “agreed” or “strongly agreed” that they would consider using Google Glass in their future practice. A summary of user feedback data is provided in Table 4.
User Feedback.
When asked of their overall impressions of using Google Glass for vital sign monitoring of a patient in a surgical or procedural setting, the majority of participants responded positively. Participants’ comments about Google Glass for vital sign streaming included “it has a lot of potential,” “offers the chance for improved situational awareness in the clinical setting,” “didn’t have to look away from procedure to see vitals,” “great way to know patients’ vitals during procedures,” and “very helpful.” Two subjects commented about the learning curve, with one participant reporting their overall impression of using Google Glass in this setting as “a little cumbersome but most likely just a little awkward given my inexperience with it thus far.” One participant commented about the benefit of not having to take the procedural field out of view to monitor vital signs. Another participant noted that the usefulness of Google Glass for vital sign monitoring would depend on whether or not a nurse or technician was available to assist with vital sign monitoring.
Discussion
Periprocedural surveillance of patient vital signs is a critical aspect of safe surgical practice. Prompt recognition of vital sign deteriorations such as desaturations or hypotension can prevent serious complications and improve patient safety. Although traditional vital sign monitoring displays patient vitals in real time, this display is not always visible to the surgeon while they are focused on the procedural field. Thus, critical vital sign changes can easily be overlooked with traditional vital sign monitoring alone. This is particularly relevant in procedures requiring conscious sedation where an anesthesiologist or assistant is not present, such as emergency endotracheal intubation, bronchoscopy, angiography, endoscopy, and thoracostomy tube placement.
This randomized controlled pilot study is the first to successfully demonstrate the feasibility of wireless vital sign streaming from a traditional patient monitor to a mobile head-mounted Google Glass platform. This study also confirms that real-time wireless streaming of vital signs is possible without perceptible time delay. This platform offers operators the option of keeping the patient’s vital signs in their immediate peripheral field of view at all times, therefore not having to actively look away from the procedural field during critical steps of the procedure. Many have likened the experience to looking into a rear view mirror of a car (meaning the data are there if you choose to look at it). Possible applications of this type of technology are numerous, in settings ranging from the operating room to intensive care unit to outpatient clinic.
This study also aimed to explore potential utility of this technology and whether use of the head-mounted platform in addition to the traditional vital sign monitor could improve time to recognition of vital sign deterioration. In this pilot, live streaming of vital signs to Google Glass resulted in a slight trend toward earlier recognition of critical vital sign changes in both bedside procedure scenarios but did not reach statistical significance. In both scenarios, there was a statistically significant difference in the time spent looking away from the procedural field to view the traditional vital sign monitor and the number of glances at the traditional vital sign monitor between the control and experimental groups. This suggests that head-mounted display platforms could allow surgeons to closely and accurately monitor vital signs of a patient without taking their visual focus away from the procedural field during critical portions of a procedure. The visual display of Google Glass is designed to be transparent (see through) even when material is being displayed on it the user’s peripheral visual field. This unique design feature helps limit distractions, and prevents obstruction of the user’s active visual field.
User feedback regarding use of Google Glass for wireless vital sign monitoring was overall positive. The majority of participants agreed that Google Glass increased their situational awareness, was helpful in monitoring vital signs, was easy to use, and has potential to improve patient safety. Users did not feel that Google Glass was distracting or inhibited their ability to perform procedural tasks. Although most users agreed they would consider using Google Glass in their future surgical practice, they did not feel that it could replace traditional vital sign monitors and felt that there was a learning curve associated with its use.
In January 2015, Google, Inc, announced discontinued production of the first generation of Google Glass. However, it is anticipated that the company will release in 2016 a newer version of Google Glass intended for enterprise/industry consumers. In the meantime, select Glass partners have received preliminary access to this newer version of Google Glass. Concurrently, other enterprises (ODG R-7, EPSON, VUXIZ, and Sony) have also developed competing head-mounted displays, several of which have reached production, and each with their own unique design features. In March 2014, the online social networking service, Facebook, acquired the head-mounted display Oculus Rift for more than $2 billion—highlighting the potential and wide applicability of this type of technology.
There are several limitations of this study, most notably the limited statistical power due to the small sample size, which limits the interpretation of the statistical analysis for time to recognition of vital sign deterioration. A post hoc power analysis was performed, which revealed inadequate statistical power for time to recognition of hypotension and time to recognition of desaturation. We therefore cannot draw a definitive conclusion at this time whether or not this technology results in earlier recognition of vital sign abnormality compared with traditional vital sign monitors alone. The study was also performed in a simulated setting, and future studies would be needed to replicate these findings in an actual clinical environment. In addition, most residents had never used Google Glass prior to this study. Similar to other eyewear, Google Glass requires personalized fitting to optimal viewing. This was not possible in our study for every resident, especially for those who required corrective lenses. In addition, there was limited time given for participants to become accustomed to Google Glass prior to entering the scenarios. Based on user feedback from this study, a learning curve may exist before users are fully comfortable with the new viewing experience. Only surgical residents at a single academic institution were included, thus limiting the generalizability of the findings. Future larger studies at multiple institutions including trainees and faculty from multiple specialties are needed. Finally, although the findings of this study suggest that use of wireless streaming of vital signs to Google Glass is feasible and may reduce the time spent looking away from the surgical field, additional studies are needed to draw conclusions regarding the utility of this technology in patient safety. Future studies aimed at detecting improvements in clinical patient outcomes are ultimately needed.
Conclusions
This pilot study adds to the growing body of literature of potential applications of Google Glass in the medical setting and provides preliminary evidence for the feasibility and potential utility of wireless streaming of patient vital signs to mobile head-mounted display devices. Wireless streaming of vital signs to Google Glass holds promise in allowing physicians to monitor patient vital signs without looking away from the surgical field. Application of this nascent technology in the clinical setting for periprocedural monitoring of patients holds potential for increased situational awareness and improved patient safety. Future studies, including a randomized controlled trial in the clinical setting, are needed.
Footnotes
Acknowledgements
The authors would like to thank Kate McGurk, Operations Manager at the Goodman Surgical Education Center, for her assistance with implementing the study and performing data collection.
Authors’ Note
Results from this study were presented as an oral presentation at the 10th Annual Academic Surgical Congress in Las Vegas, NV, February 3-5, 2015.
Author Contributions
CAL contributed to conception and design, acquisition of data, analysis and interpretation, study supervision, drafted the manuscript, critically revised the manuscript, gave final approval, and agrees to be accountable for all aspects of work ensuring integrity and accuracy.
MAZ contributed to conception and design, acquisition of data, analysis and interpretation, study supervision, critically revised the manuscript, gave final approval, and agrees to be accountable for all aspects of work ensuring integrity and accuracy.
OA contributed to conception and design, acquisition of data, study supervision, critically revised the manuscript, gave final approval, and agrees to be accountable for all aspects of work ensuring integrity and accuracy.
JT contributed to acquisition of data, analysis and interpretation, study supervision, critically revised the manuscript, gave final approval, and agrees to be accountable for all aspects of work ensuring integrity and accuracy.
JNL contributed to acquisition of data, analysis and interpretation, study supervision, critically revised the manuscript, gave final approval, and agrees to be accountable for all aspects of work ensuring integrity and accuracy.
Study concept and design: Cara A. Liebert, Mohamed A. Zayed, Oliver Aalami
Acquisition of data: Cara A. Liebert, Mohamed A. Zayed, Oliver Aalami, Jennifer Tran, James N. Lau
Analysis and interpretation: Cara A. Liebert, Mohamed A. Zayed, Jennifer Tran, James N. Lau
Study supervision: Cara A. Liebert, Mohamed A. Zayed, Oliver Aalami, James N. Lau
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr Aalami and Dr Zayed were involved in the development of the VitalVideo software platform and report equity in Vital Enterprises, Inc. Dr Aalami is an advisor to Vital Enterprises, Inc. Dr Liebert, Dr Lau, and Ms Tran report no proprietary or commercial interest in any product mentioned or concept discussed in this article. No funding was received from Vital Enterprises, Inc for this research.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.