
Abstract

Laparoscopic cholecystectomy (LC) is one of the most frequently performed procedures in general surgery worldwide. Although considerable advances have been achieved in technology and surgical techniques, iatrogenic bile duct injuries (BDI) still represent a major public health problem related to both medicolegal terms and health care costs. It has been demonstrated that the primary cause of BDI is the misinterpretation of biliary anatomy (71% to 97% of all cases). 1 Various methods have been proposed and described in the scientific literature to prevent iatrogenic biliary tract lesions: the evaluation of the critical view of safety (CVS) method, antegrade dissection, subtotal cholecystectomy, and landmark techniques, such as Rouviere’s sulcus and radiographic intraoperative cholangiography.2,3 The CVS technique was introduced by Strasberg and Brunt in 1995, 2 and it is considered the gold standard to perform a safe cholecystectomy with identification of biliary structures (eg, cystic duct, common hepatic duct, and common bile duct) during dissection. Three criteria are required to achieve the CVS: (1) the hepatocystic triangle must be cleared of adipose and fibrotic tissues; the common bile duct and common hepatic duct must not be exposed; (2) the lower third of the gallbladder must be separated from the liver bed to expose the cystic plate; and (3) 2 and only 2 structures should be seen entering the gallbladder.
Near-infrared fluorescent cholangiography (NIRF-C) was introduced by Ishizawa et al in 2009. 4 This is an intraoperative imaging technique that allows a real-time enhanced visualization of the extrahepatic biliary tree by fluorescence (Figure 1). NIRF-C is based on the administration of a fluorophore, the indocyanine green, which is excreted in the biliary system, and on the use of a near-infrared light source, exciting the fluorophore and enabling the visualization. NIRF-C offers some clear advantages when compared with the conventional cholangiography (real-time visualization of biliary tree, reduced costs, easy learning curve, lack of X-ray exposure, safer dissection of Calot’s triangle, and possibility to associate fluorescent angiography to highlight vessels).5,6 Additionally, NIRF-C has shown a good potential as a teaching tool for trainees.5,7
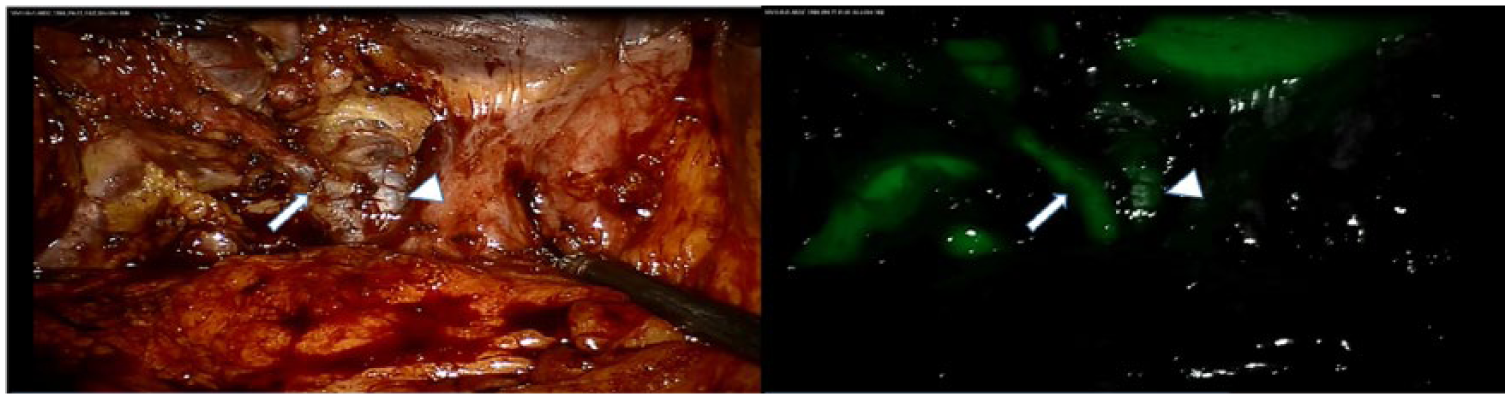
(Left) White light view of the Calot’s area after dissection of the cystic duct (arrow) and visualization of the hepatic duct (arrow head). (Right) Same image in near-infrared mode, confirming the anatomy.
In the early 1990s, Professor Strasberg asserted that bile iatrogenic lesions do not depend on the total number of performed cholecystectomies but on the technique used, underscoring the importance of the critical view of safety method. Today, innovations in surgical technology is augmenting the surgeon’s “eye” in order to improve the correct identification of the CVS during LC.8,9 It is a perfect combination of surgical anatomy and technological innovation. NIRF-C could well represent a useful method to identify the CVS with the aid of real-time fluorescent vision. With the use of fluorescent cholangiography, the common hepatic duct and the common bile duct can be often visualized before the direct exposure of these structures. Only biliary structures can emit fluorescence, and this property could help in distinguishing biliary and vascular elements intraoperatively and in recognizing anatomical biliary variants during dissection.8-10 In the ongoing, randomized, controlled FALCON trial, 10 the investigators have set as a main outcome and surrogate marker of efficacy, the “time to achieve the CVS” with or without the fluorescence enhancement. A limit with NIRF-C can be seen in the relatively high fluorescence background from the liver, which can be sometimes disturbing and could affect the correct visualization of the biliary tree. 11 In order to reduce such a drawback, some optimizations are still required and a consensus should be reached regarding the optimal dosing and timing of injection of the fluorophore. 12
We would like to stress that every single cholecystectomy may hide pitfalls, and that any efforts toward the reduction of the risk profile of everyday cholecystectomy is appreciated. Despite the current level of evidence remaining low, 6 and randomized trials are still ongoing, we believe that NIRF-C has an enormous potential to become a gold standard during all cholecystectomies and a paramount teaching tool for trainees and might lead to lowering the incidence of BDI during LC.
Footnotes
Authors’ Note
Michele Diana is the recipient of a grant from the ARC Foundation (the largest French foundation dedicated to cancer research) to develop fluorescence-guided surgery.
Author Contributions
Study concept and design: Antonio Pesce, Michele Diana
Analysis and interpretation: Antonio Pesce, Michele Diana
Acquisition of data: not applicable
Study supervision: Michele Diana