
Abstract

To the Editors:
We present and discuss, to the best of our knowledge, the first successful robotic-assisted total hysterectomy performed in a cardiac transplantee. A 45-year-old woman, who 14 years previously had orthotopic cardiac transplantation for post-partum cardiomyopathy, developed menorrhagia and cyclical migraines impacting heavily upon her quality of life. Ultrasound examination revealed an enlarged, multi-fibroid uterus (largest fibroid 23 × 17 × 15 mm).
An intrauterine progesterone-releasing system worsened migraines; endometrial ablation achieved only short-term symptom control, and systemic hormonal therapy was contraindicated because of migraine and prior deep vein thrombosis. Preoperative echocardiography demonstrated good left ventricular function with no significant valvular lesions. The patient was offered hysterectomy. The procedure was undertaken using a da Vinci robot, which has advantages over conventional laparoscopy, particularly reduced intraoperative blood loss and postoperative pain. 1 Other benefits of robotic surgery include smaller incisions, reduced infection and scarring, improved postoperative mobility, and overall faster recovery, whilst technical benefits include superior intraoperative visualisation of intra-abdominal structures, increased dexterity, and precision. 2
Intraoperatively, ports were placed in the supraumbilical region, left iliac fossa, and right and left hypochondria. Anaesthetic induction comprised preoxygenation, propofol, remifentanil, and atracurium. Hemodynamic parameters were monitored with a radial arterial line. The patient was placed in the steep Trendelenburg position required for robotic pelvic surgery, during which there were 2 brief, self-terminating tachyarrhythmias, most likely supraventricular in origin with pre-existing aberrant conduction; however, defibrillator pads were applied as a precaution. A delayed, but normal magnitude, hypertensive response was noted in response to pneumoperitoneum and surgical incision. Brief, yet more prolonged than typical, hypotension was observed upon pneumoperitoneum release, treated with 3 mg of intravenous ephedrine.
Cardiac transplantees may have reduced physiological tolerance to intrinsic or extrinsic factors, causing or requiring a change in haemodynamics. During insufflation, stretching of the intra-abdominal peritoneum may increase vagal tone that can lead to hypotension and bradycardia, 3 whilst pneumoperitoneum and the steep Trendelenburg position required for robotic surgery can place unusual physiological strains on the cardiovascular system, unmasking subclinical systolic or diastolic dysfunction. For example, both systemic and pulmonary vascular resistance increase upon abdominal insufflation, with resultant effects including increased myocardial oxygen demand, unmasking coronary stenoses due to cardiac allograft vasculopathy, and worsening of commonly present tricuspid valve regurgitation.3,4 On the other hand, increased abdominal pressure may cause caval compression and hence reduce preload. Similarly, post-transplantation atrial scarring can reduce the ability to compensate for changes in preload, whilst also pre-disposing to both conduction disease and supraventricular arrythmia, 5 which may be exacerbated by the circulating catecholamines induced by surgery. Modulation or absence of the neural autonomic response may also result from cardiac denervation, which typically leads to resting sinus tachycardia in cardiac transplant recipients.
The importance of adequate preparation, awareness of the altered physiology within a cardiac transplantation patient, and the demands of robotic and laparoscopic surgery are crucial for a safe, uneventful procedure. These factors along with the disadvantages of robotic surgery (longer operating time, need for specialist, expensive equipment, and appropriately trained surgeons and assistants) should be carefully considered (Figure 1) Benefits and drawbacks of robotic surgery.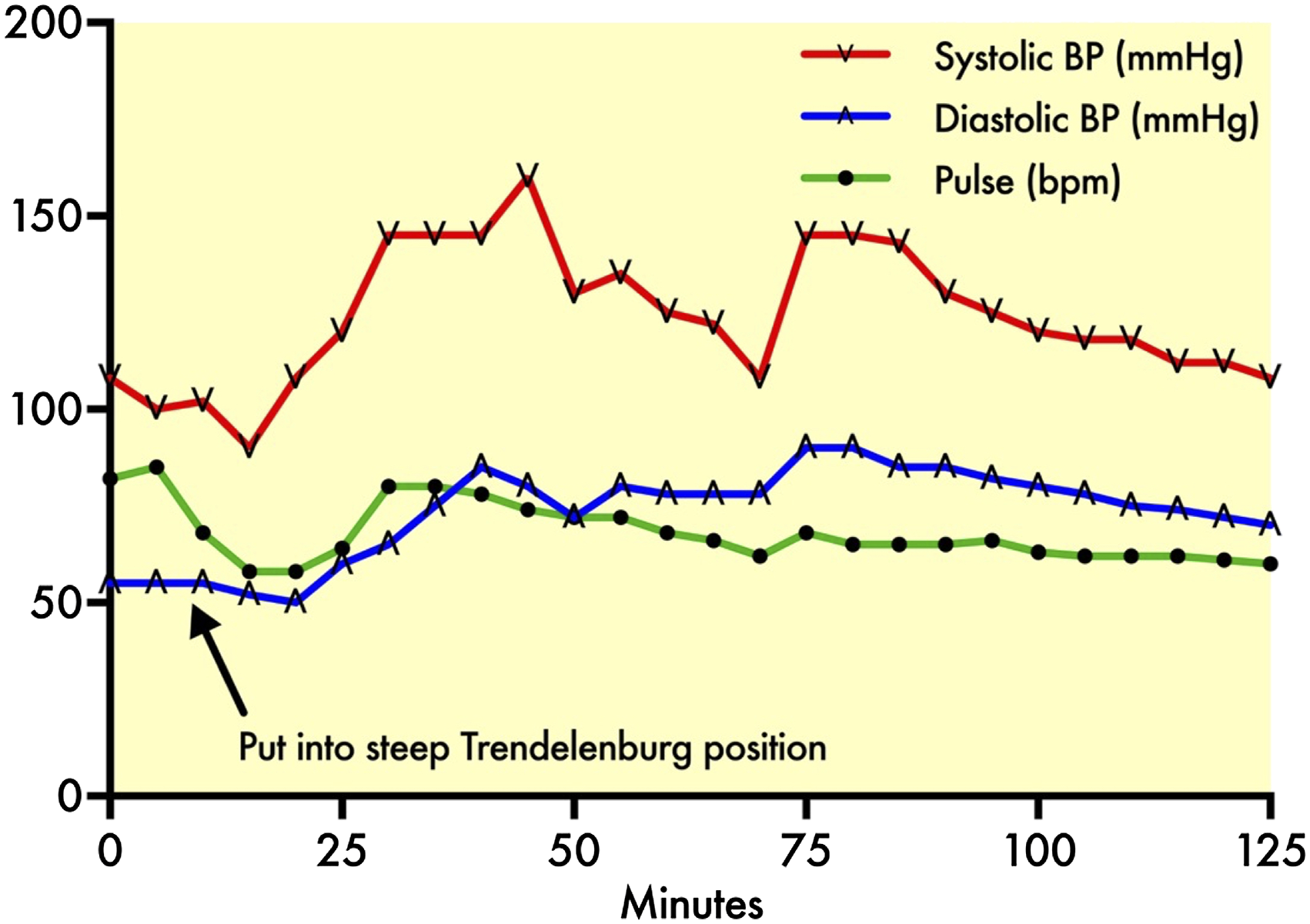
Footnotes
Author Contributions
Dr Victoria Parker was part of the surgical team during the robotic hysterectomy of the reported case, and has reviewed the patient records, collected data, and co-written and edited this manuscript. Dr William Parker was part of the clinical care team for the patient whose case is reported, and has reviewed the patient records, collected data, and co-written and edited this manuscript. Dr Holly Davies was part of the surgical team during the robotic hysterectomy, and has reviewed the patient records and collected data; Mrs Helen Ramshaw was part of the clinical care team for the patient whose case is reported, and reviewed the patient records and collected data; Mrs Emma K. D’Arcy was part of the clinical care team for the patient whose case is reported, and reviewed the patient records and collected data; Professor Abdallah Al-Mohammad was part of the clinical care team for the patient whose case is reported and edited this manuscript; Dr Olena Mateszko led the anaesthetic team during the robotic hysterectomy, and has reviewed the patient records, collected data, and edited this manuscript; Miss Fiona Kew led the surgical team during the robotic hysterectomy and edited this manuscript; and Mr Peter Braidley was part of the clinical care team for the patient whose case is reported and has edited this manuscript.
Study concept and design: Victoria L. Parker, William A.E Parker, Holly M Davies, Abdallah Al-Mohammad, Olena Mateszko, Fiona M. Kew and Peter C. Braidley.
Acquisition of data: Victoria L. Parker, William A.E Parker, Holly M. Davies, Helen J. Ramshaw, Emma K. D'Arcy, Olena Mateszko and Fiona M. Kew.
Analysis and interpretation: Victoria L. Parker, William A.E Parker, Holly M. Davies, Abdallah Al-Mohammad, Olena Mateszko, Fiona M. Kew and Peter C. Braidley.
Study supervision: Abdallah Al-Mohammad, Olena Mateszko, Fiona M. Kew and Peter C. Braidley.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Patient Consent
Patient consent was obtained for this study.