
Abstract
Dear Editors,
Hernia repair remains one of the most commonly performed surgical procedures worldwide, with an estimated twenty million operations performed each year.
1
Despite this volume and a history spanning more than a century, the field is far from static. Hernia surgery stands at an inflection point, shaped by converging advances in biomaterials, robotics, data science, and patient-centered care.
2
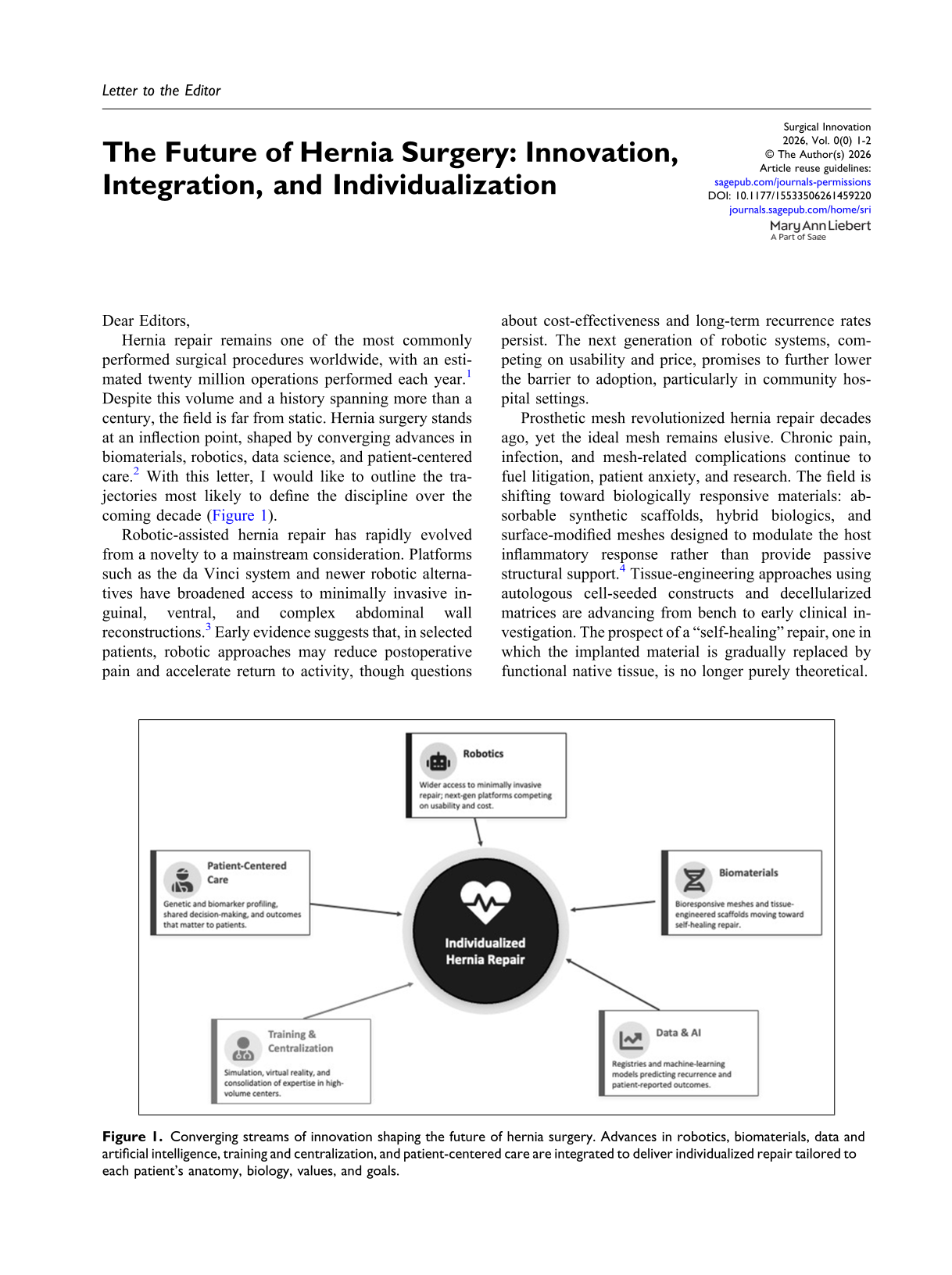
With this letter, I would like to outline the trajectories most likely to define the discipline over the coming decade (Figure 1). Converging streams of innovation shaping the future of hernia surgery. Advances in robotics, biomaterials, data and artificial intelligence, training and centralization, and patient-centered care are integrated to deliver individualized repair tailored to each patient’s anatomy, biology, values, and goals.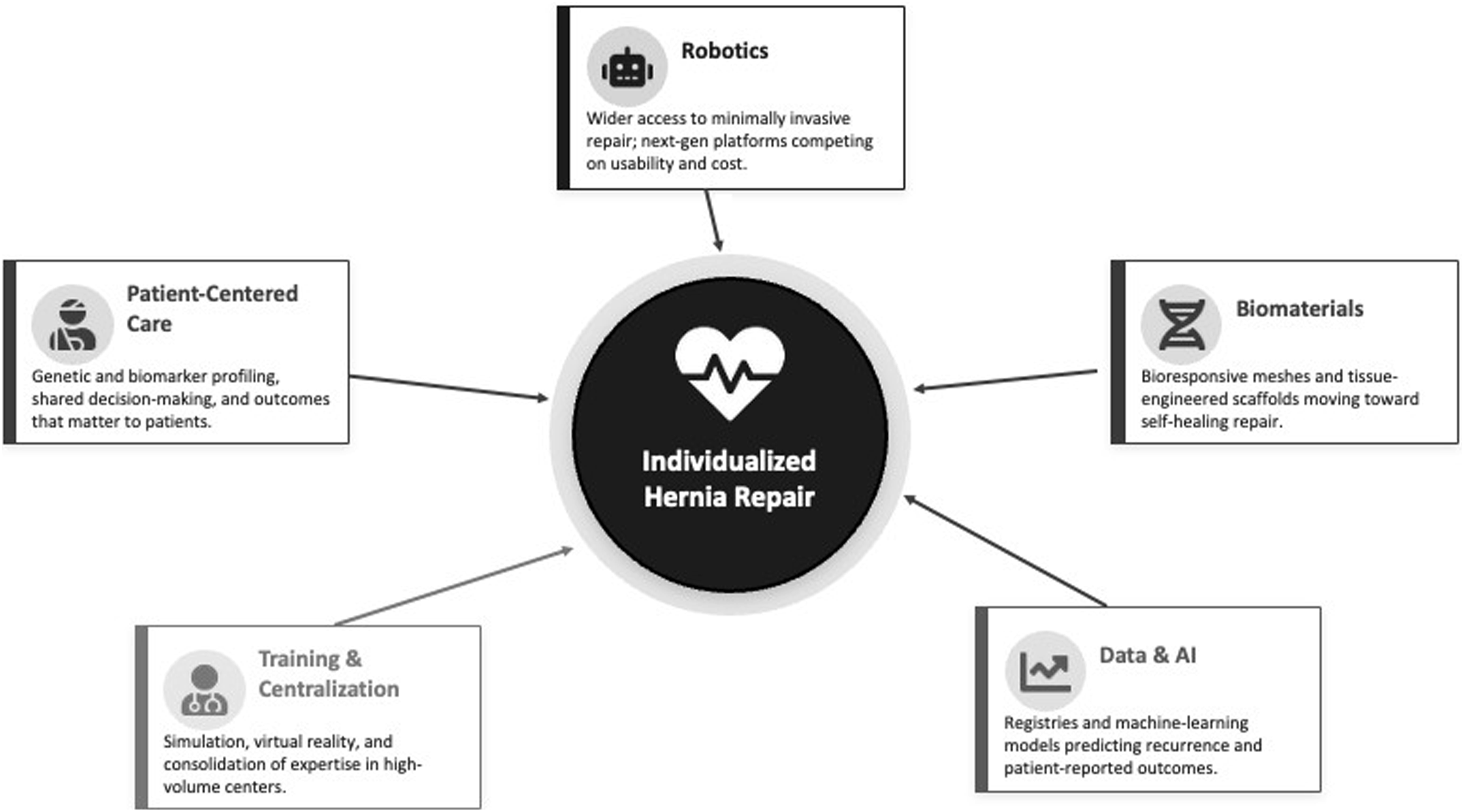
Robotic-assisted hernia repair has rapidly evolved from a novelty to a mainstream consideration. Platforms such as the da Vinci system and newer robotic alternatives have broadened access to minimally invasive inguinal, ventral, and complex abdominal wall reconstructions. 3 Early evidence suggests that, in selected patients, robotic approaches may reduce postoperative pain and accelerate return to activity, though questions about cost-effectiveness and long-term recurrence rates persist. The next generation of robotic systems, competing on usability and price, promises to further lower the barrier to adoption, particularly in community hospital settings.
Prosthetic mesh revolutionized hernia repair decades ago, yet the ideal mesh remains elusive. Chronic pain, infection, and mesh-related complications continue to fuel litigation, patient anxiety, and research. The field is shifting toward biologically responsive materials: absorbable synthetic scaffolds, hybrid biologics, and surface-modified meshes designed to modulate the host inflammatory response rather than provide passive structural support. 4 Tissue-engineering approaches using autologous cell-seeded constructs and decellularized matrices are advancing from bench to early clinical investigation. The prospect of a “self-healing” repair, one in which the implanted material is gradually replaced by functional native tissue, is no longer purely theoretical.
Large hernia registries are generating unprecedented volumes of outcome data, and machine learning applied to these datasets is beginning to yield predictive models for recurrence, surgical site infection, and patient-reported outcomes. 5 In the near future, surgeons may consult decision-support tools that integrate patient-specific variables such as body mass index, comorbidities, defect characteristics, and prior surgical history to recommend tailored operative strategies. These tools do not replace clinical judgment; they augment it. Realizing this potential requires standardized data collection, interoperability across registries, and rigorous external validation of predictive models.
Perhaps the most consequential shift is philosophical: the recognition that no single technique suits every patient or every defect. The era of the “one-size-fits-all” repair is giving way to a more nuanced, individualized approach. Future refinements will likely incorporate genetic susceptibility to connective tissue disorders, biomarker-based assessments of wound-healing capacity, and patient preferences regarding trade-offs between recurrence risk and mesh avoidance. The surgeon of the future will function less as a technician and more as an integrator, synthesizing biological, technological, and personal variables into a personalized operative plan.
As techniques proliferate and complexity rises, surgical training must adapt. High-fidelity simulation, virtual reality, and proctored cases will be essential to ensure that innovation translates into improved outcomes rather than a prolonged learning curve borne by patients. In this context, we will likely see a trend toward further centralization in the coming decades, solely to increase surgical expertise.
The future of hernia surgery is defined not by a single breakthrough but by the convergence of multiple streams of innovation. For clinicians and researchers, the imperative is clear: embrace interdisciplinary collaboration, contribute to shared data ecosystems, and maintain rigorous standards of evidence even as innovation accelerates. The hernia of the future will still require repair, but that repair will be smarter, safer, and more precisely tailored than ever before.