
Abstract
Objective:
Femoral artery cannulation is the most commonly used approach for cardiopulmonary bypass (CPB) in robotic cardiac procedures. However, without adding a distal perfusion cannula, leg ischemia can occur in up to 11.5% of patients. There is a well-described 2 to 4 mm size arterial branch that originates from the medial side of the external iliac artery or inferior epigastric artery, immediately above the inguinal ligament, and connects to the obturator artery. Therefore, it was historically named the corona mortis, which means “crown of death” in Latin. When peripheral cannulation is performed above this branch in the external iliac artery, we consider it a corona “vitae” because of its role as a limb-saving collateral. We report herein our standard technique of peripheral cannulation without the need of a distal perfusion cannula and preventing limb ischemia.
Methods:
We included all patients who underwent robotic cardiac surgery with peripheral cannulation over a 16-month period at our institution. We cannulated just above the level of the inguinal ligament through a 2 to 3 cm transverse skin incision. The incidence of limb ischemia and vascular complications was recorded and analyzed.
Results:
During the study period, 133 patients underwent robotic cardiac procedures with peripheral “external iliac” CPB. The size of the cannula was 21F or larger in 73% and 23F in 54% of the patients. No leg ischemia or femoral artery complications requiring additional intervention occurred.
Conclusions:
External iliac cannulation can be successfully performed in robot-assisted cardiac surgery using relatively large cannulas without the need of a distal limb perfusion catheter, with good results. In our view, given the importance of the corona mortis (“crown of death” in Latin) in perfusing the limb during CPB, we propose a new name for this artery in robotic cardiac surgery, namely, the corona vitae (“crown of life” in Latin).
Central Message
Our study demonstrates the safety and efficacy of direct external iliac cannulation with reliance on the corona mortis collateral for CPB during robotic and minimally invasive cardiac procedures. We propose the term corona vitae to describe the corona mortis collateral in the context of cardiac surgery.
Introduction
Femoral artery cannulation is a frequently used method for establishing cardiopulmonary bypass (CPB) during robotic cardiac procedures. However, without the addition of a distal perfusion cannula, the risk of leg ischemia during CPB can be as high as 11.5%. 1 Fortunately, there exists a well-described anatomical collateral artery known as the corona mortis (Fig. 1), a 2 to 4 mm arterial branch that connects the external iliac artery to the internal iliac artery. This branch can function as a natural collateral for lower extremity perfusion during femoral CPB. 2 The corona mortis typically originates from the medial side of the external iliac artery or the inferior epigastric artery, immediately above the inguinal ligament, and connects to the obturator artery. 2 However, due to its unique course, injury to the corona mortis during orthopedic or inguinal hernia surgery can result in severe, life-threatening bleeding that is difficult to control, leading to the historical name of “crown of death” in Latin. 3
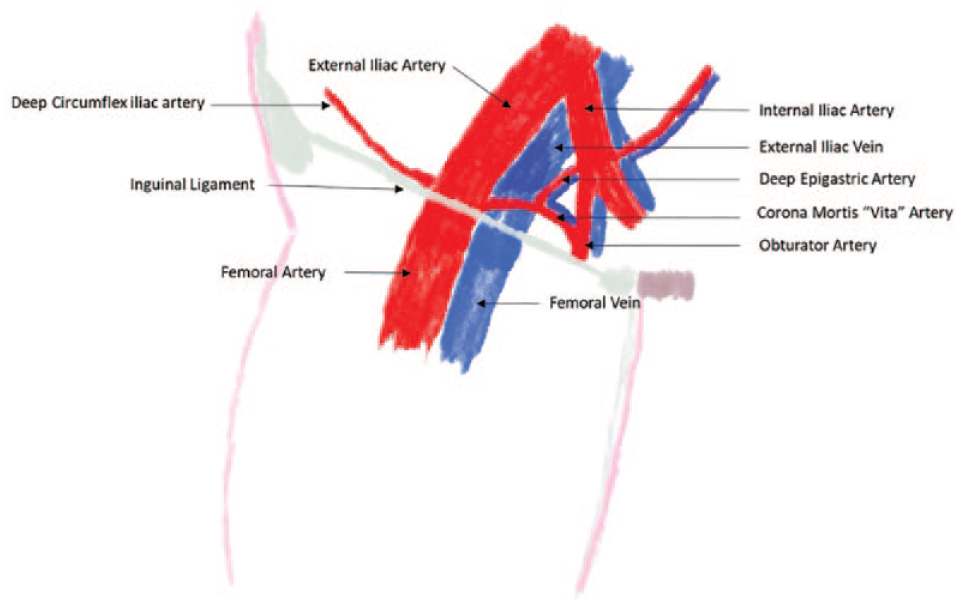
The external iliac artery and its anatomical relation to corona mortis, deep epigastric, and deep circumflex iliac arteries.
Despite its potential danger during certain procedures, the corona mortis can also play a vital role in maintaining limb perfusion when peripheral cannulation is performed above this branch in the external iliac artery. Therefore, we propose renaming it the corona vitae or “crown of life.” 2 This study reports our standard technique for peripheral cannulation utilizing the corona vitae without the need for a distal perfusion cannula to prevent limb ischemia during CPB. We present our experience with this technique in a cohort of 133 patients undergoing robotic cardiac surgery with peripheral cannulation.
Surgical Technique
Methods
We conducted a retrospective analysis of 133 patients who underwent robotic cardiac surgery at our institution over a 16-month period. The study population consisted of patients who underwent mitral valve repair or replacement (n = 105), aortic valve replacement (n = 11), isolated maze procedure (n = 7), and other procedures (n = 10). There were 5 patients who required axillary artery cannulation because of aorto-iliac and peripheral vascular disease and were excluded from the analysis. The study was approved by the institutional review board, and patient consent was waived due to the retrospective and deidentified nature of the study.
The external iliac artery was cannulated just above the level of the inguinal ligament through a 2 to 3 cm transverse skin incision. Specifically, after opening the external oblique aponeuroisis and reflecting the retroperitoneal tissues cephalad, the supra-inguinal artery and vein were dissected, the collateral (corona vitae) artery was identified, and a purse-string suture was placed for arterial cannulation above it (Fig. 2). Flow from the cannula into the internal iliac artery collateralizes the distal femoral circulation through this (and sometimes other collaterals) as a natural inflow for the lower extremity during CPB (Fig. 3, Supplemental Video).
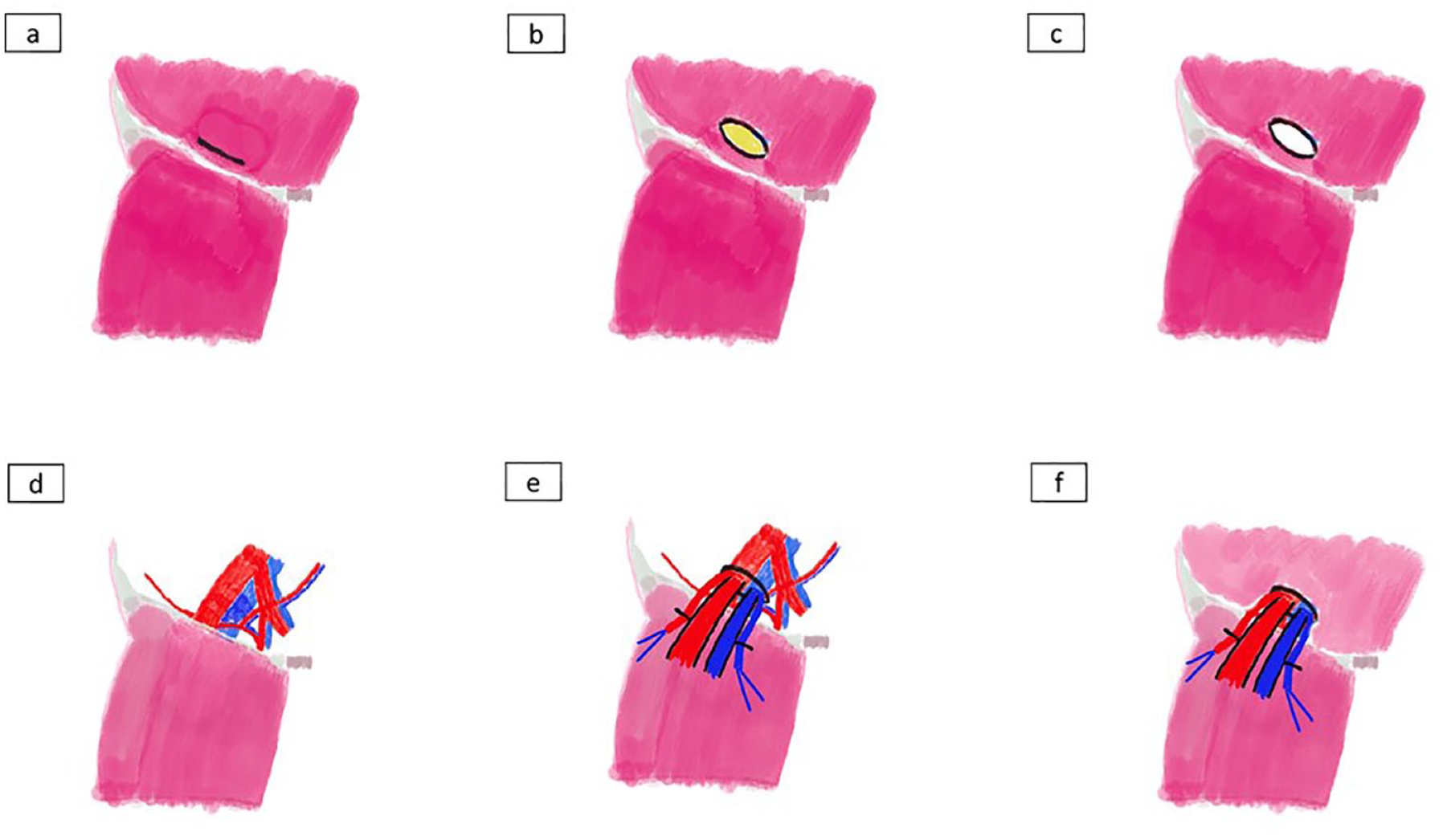
Steps of external iliac artery cannulation. (a) Mark inguinal ligament 2 to 3 cm above the inguinal ligament. (b) Dissect through the subcutaneous tissue. (c) Expose the inguinal ligament by dissecting the inguinal ligament, followed by dissecting the muscle/fat from the inguinal ligament. (d) Expose the external iliac artery and vein, corona mortis, and deep epigastric arteries. (e) (f) Cannulate the external iliac artery above the corona mortis.
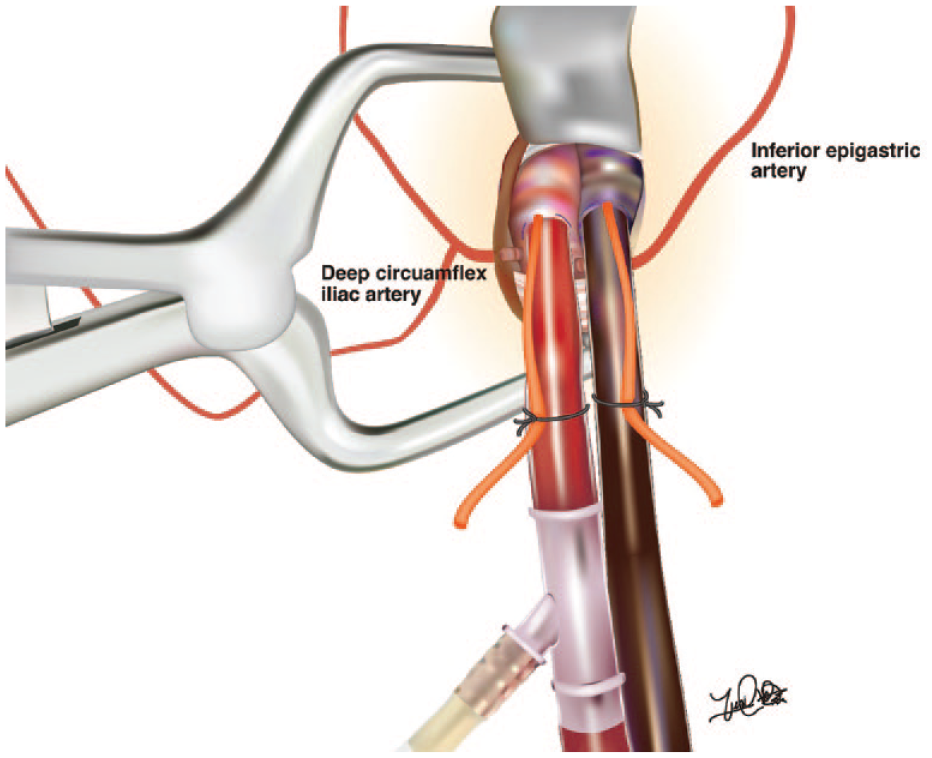
Illustration of the external iliac vessel cannulation and its anatomical relation to the deep epigastric and deep circumflex iliac arteries. Illustration by Yuki Ikeno, MD.
Transcutaneous near-infrared spectroscopy (NIRS) monitors were routinely placed on the calf of both lower extremities to monitor O2 saturation during CPB. The incidence of limb ischemia and vascular complications was recorded and analyzed. Any local complications, such as laceration or bleeding, were also documented. The data were collected retrospectively from electronic medical records and operative reports.
Results
In total, 113 patients who underwent robotic cardiac procedures with peripheral femoral CPB were included in the study. The mean body surface area of the patients was 1.95 ± 0.26 m2, and the mean maximum and minimum diameters of the supra-inguinal femoral artery were 9.7 ± 1.6 mm and 8.7 ± 1.6 mm, respectively. A 21F or larger cannula was used in 73% of patients, with the majority (54%) being a 23F EndoReturn arterial cannula (Edwards Lifesciences, Irvine, CA, USA) with a side-arm for the endoballoon.
There were no cases of leg ischemia or femoral artery complications requiring additional intervention. Transcutaneous NIRS showed that the variance of the mean O2 saturation from baseline to cannulation (prepump) and postcannulation to on CPB was −12.7% (the mean decreased from 69.6 to 56.8) and −25.3 (the mean decreased from 69.6 to 44.3), respectively (Table 1).
Left-Side and Right-Side Cerebral and Leg Transcutaneous Near-Infrared Spectroscopy at Baseline, Postcannulation, and on CPB.
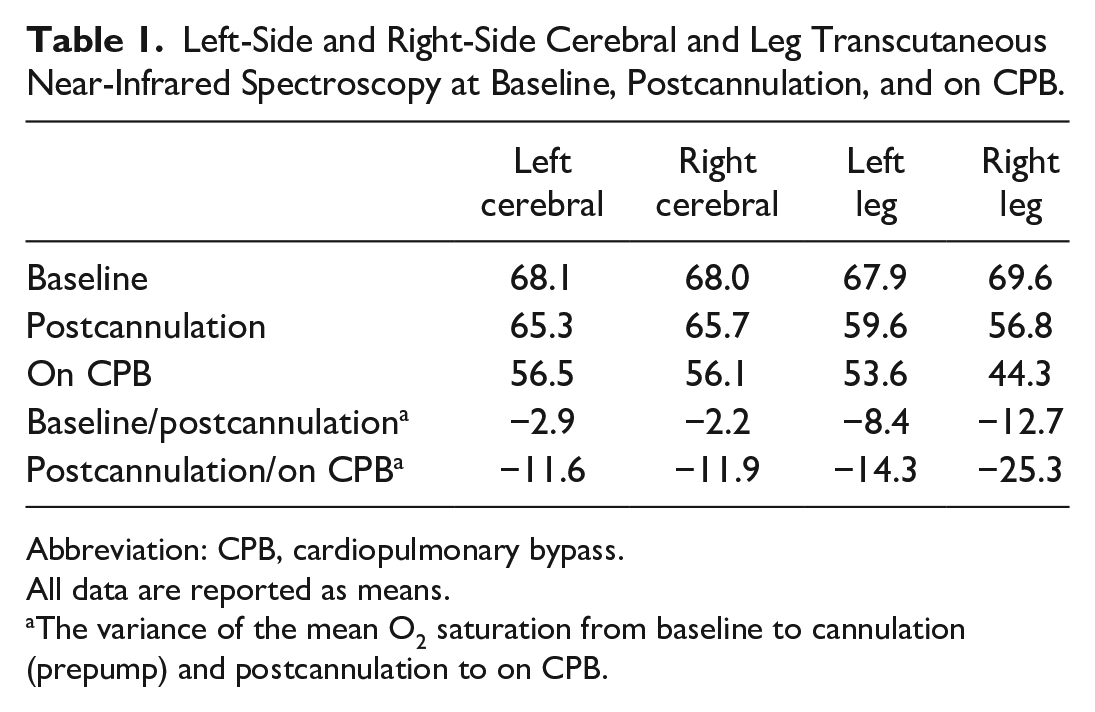
Abbreviation: CPB, cardiopulmonary bypass.
All data are reported as means.
The variance of the mean O2 saturation from baseline to cannulation (prepump) and postcannulation to on CPB.
Discussion
Our study demonstrates that direct external iliac cannulation with reliance on the corona mortis collateral is a safe and effective technique for CPB during robotic and minimally invasive cardiac surgery procedures. Our results showed no incidence of leg ischemia or vascular complications requiring additional intervention. These findings suggest that this technique can be safely and effectively used for peripheral cannulation in robotic cardiac procedures, without the need for a distal perfusion cannula.
We believe that this technique has an advantage over the use of a distal perfusion cannula, which can be associated with risks such as dislodgement or inadequate perfusion. Robotic cardiac surgery offers many advantages such as smaller incisions, reduced blood loss, and faster recovery times.4 –6 However, the use of peripheral cannulation for CPB carries the risk of leg ischemia and vascular complications.7 –11 Several techniques have been developed to prevent the complications associated with peripheral cannulation, including the use of bidirectional self-expanding cannula, 12 distal perfusion cannula, sewing an end-to-side graft, and the use of an endovascular balloon.13,14 However, these techniques are not without drawbacks. The use of a distal perfusion cannula can increase the risk of bleeding and dissection of the distal artery, whereas the sewing of an end-to-side graft may require more extensive exposure of the artery and can be time consuming. 15 The use of endoaortic balloon occlusion, although desirable in endoscopic robotic surgery, requires a larger cannula size that may not be suitable for all patients, especially those with peripheral vascular disease. 16 Therefore, there is a need for a reliable and safe technique for peripheral cannulation in robotic cardiac surgery that can minimize the risk of limb ischemia without the need for additional devices or procedures.
The corona mortis is a well-described anatomical variation that is present in up to 84% of individuals. Its laceration during orthopedic or inguinal hernia surgery can lead to life-threatening bleeding, which has led to the name “crown of death.”17,18 However, in cardiac surgery, its presence can be considered a “crown of life,” as it serves as a natural collateral for lower extremity perfusion during CPB. Our technique of direct external iliac cannulation above the corona mortis collateral utilizes this unique anatomical variation to prevent leg ischemia and vascular complications.
We propose the use of the term corona vitae, meaning “crown of life,” to describe the corona mortis collateral in the context of cardiac surgery. This collateral can serve as a valuable adjunct for distal limb perfusion during CPB when arterial cannulation is performed in the external iliac artery proximal to its takeoff.
Conclusions
In summary, our study demonstrates the safety and efficacy of direct external iliac cannulation with reliance on the corona mortis collateral for CPB during robotic and minimally invasive cardiac procedures. This technique offers a natural mechanism for providing distal perfusion to prevent leg ischemia and vascular complications in many patients who would otherwise need alternative measures of distal limb perfusion during CPB with femoral cannulation.
Footnotes
Acknowledgements
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.