
Abstract
Introduction
The amyloidoses are a heterogeneous group of disorders characterized by abnormal amyloid proteins deposit in the extracellular space of tissue and organs. Amyloid neuropathies can be observed due to amyloid deposition within the nerve more often in primary systemic amyloidosis or AL amyloidosis, associated with lymphoproliferative disorders where the amyloid deposits comprise immunoglobulin light-chain proteins. This may lead to focal, multifocal, or diffuse neuropathies involving sensory, motor, and/or autonomic fibers, and the symptoms depend on the distribution of nerves affected.2,15 Secondary amyloidosis or AA amyloidosis can occur in the setting of chronic infectious or inflammatory diseases. The main organ that is affected in AA amyloidosis is the kidney. The liver, spleen, and gastrointestinal tract are involved to a lesser degree. 13 AA amyloidosis rarely affects the nervous system 7 ; however, there are reported cases of autonomic neuropathy. 11
Case Report
We present the case of a 74-year-old man with a 16-month left radial nerve palsy. He had been diagnosed with a left lung apical mass of 50 mm, invading the second rib and extending to the second to third thoracic foramen 6 months before going to our office. After the mass was removed, the pathology confirmed it was an AA amyloidosis deposit with an intense immunoexpression of amyloid protein AA and negative immunoexpression of kappa and lambda light chains. Coincidental monoclonal gammopathy with a very low-value of lambda light chains was detected. The patient did not show weight loss, fever, or fatigue, and a detailed hematological follow-up examination did not indicate any systemic amyloidosis or lymphoproliferative disorders. Further imaging did not reveal any additional damage in the patient, and the abdominal fat biopsy was negative for amyloidosis. The only remarkable thing was the patient had only 1 kidney and suffered from previous urinary tract infections.
It was thought the radial nerve deficit was secondary to the lung apical mass compressing the brachial plexus, but no improvement was observed after excision. An electromyography examination revealed denervation of muscle groups supplied by the radial nerve, except for the triceps. Electromyographic testing of the axillar, musculocutaneous, median, and cubital nerves was normal. The physical examination revealed a left wrist drop, an inability to extend the patient’s fingers, and decreased feeling in the dorsal tissue between the first and second digits.
The patient underwent an arm-elbow high-resolution magnetic resonance (MR) imaging that showed an enlarged, irregular-shaped radial nerve at the level of the lateral middle-distal part of the arm (Figure 1), in addition to atrophy of the extensor carpi radialis longus, brachioradialis, and supinator muscles.
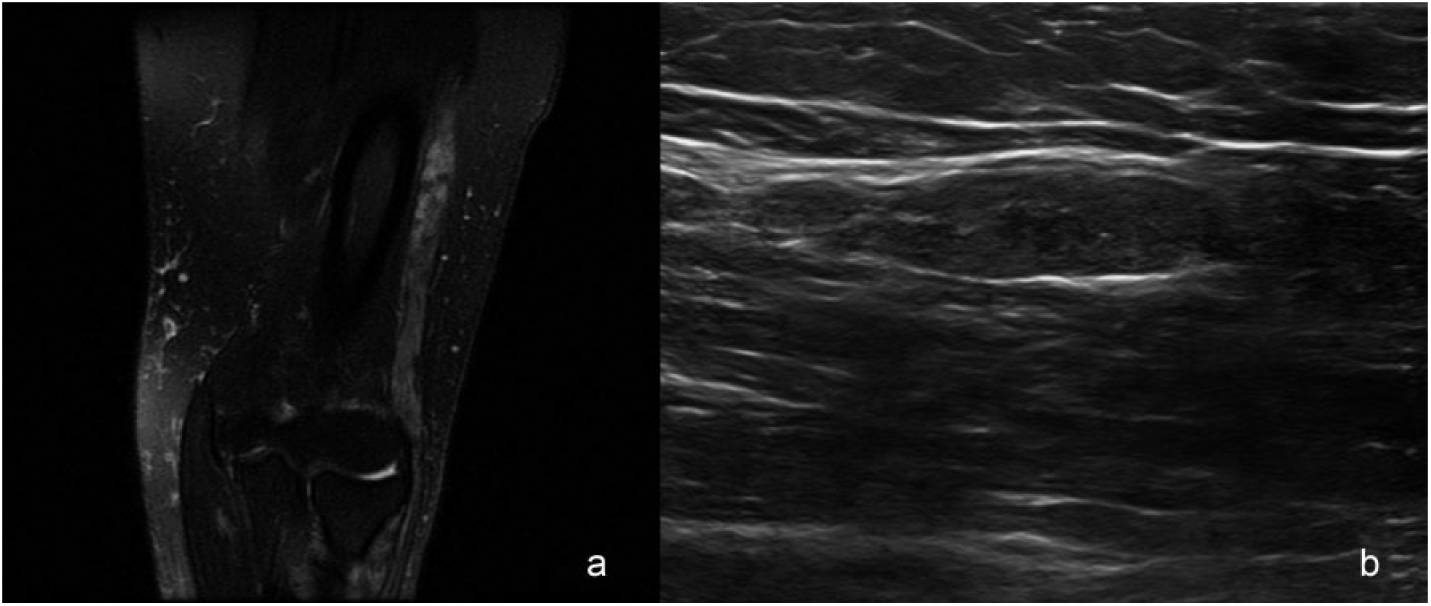
(a) Coronal T2 fat suppression magnetic resonance weighted image of radial nerve. (b) Ultrasound shows enlarged and irregular-shaped radial nerve.
Intervention
A preliminary ultrasonography was performed to mark the site of the open biopsy, where the radial nerve was enlarged (Figure 1). Exploration was done in the lateral medial-distal third of the left arm, and the radial nerve was estimated thicker and darker than a normal nerve (Figure 2).

Site of de nerve biopsy. The nerve is thicker and darker than a normal nerve.
A 4-mV stimulation was conducted along the nerve exposure without noting any visible muscular contraction, and a 1-cm fascicular biopsy was taken.
Amyloid material shows positive staining with Congo red staining (Figure 3) and immunoexpression of amyloid protein AA was evidenced, the same in the lung (Figure 4).
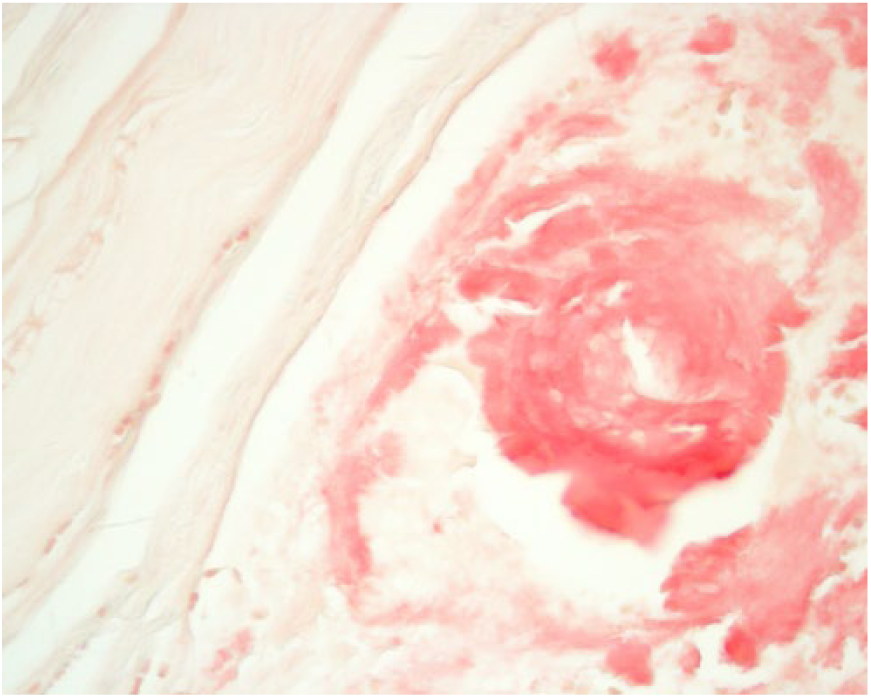
Amyloid material shows positive staining with Congo red (Congo red, original magnification ×400).
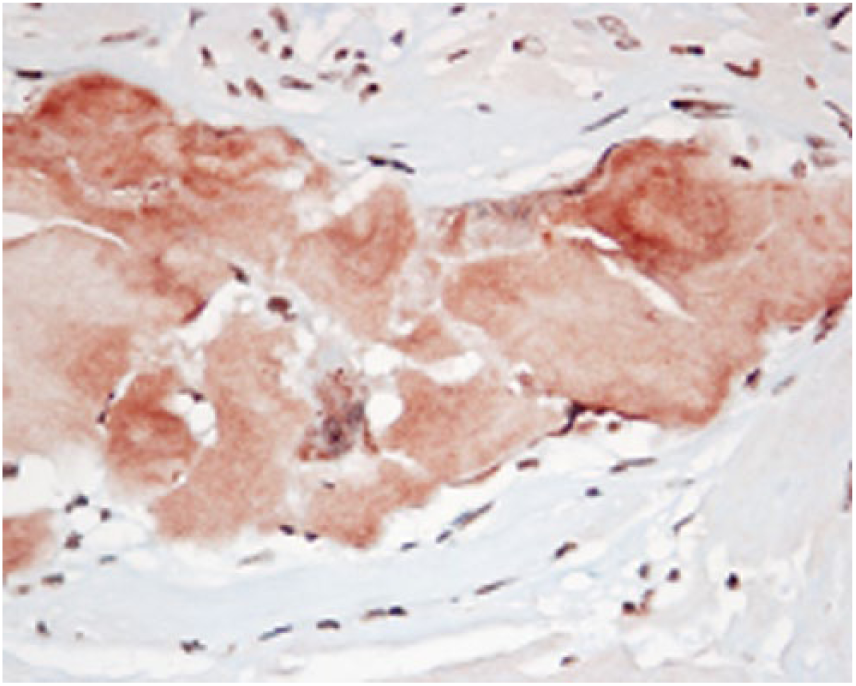
The amyloid deposit shows intense immunoexpression of amyloid protein AA (immunoperoxidase, original magnification ×400).
We determined that nerve restoration was not possible due to the long denervation time and extent of the damage, so tendon transfers were proposed to the patient but he refused to be operated on.
Discussion
Amyloidosis is a family of diseases characterized by abnormal extracellular deposition of protein fibrils that lead to the disruption of normal tissue and function. The main subtypes of systemic amyloidosis are AL (associated with a light chain-producing plasma cell dyscrasia), AA (associated with longstanding inflammation or chronic infections), wild-type ATTR (associated with transthyretin and old age), and hereditary ATTR (associated with a transthyretin mutation).10,12
Incidence
Kyle et al 8 conducted a retrospective study with data collected from 1950 to 1990 from the general population residing in Olmsted Count, Minnesota, USA. These authors reported an incidence of AL Amyloidosis in 9 cases per million person-years (95% confidence interval, 5.1-12.8 cases per million person-years). The authors inferred that approximately 2200 new cases of AL amyloidosis could occur annually in the United States.
Recently studies have been carried out in 2 European regions: Pinney et al, from the National Health Service National Amyloidosis Centre in the United Kingdom, estimated a global incidence of amyloidosis in England of 5 cases per million person-years. Of these, close to 3 cases would have the AL type and 1 case the AA type. 14 In Sweden, Hemminki et al calculated an incidence of 8 patients per million person-years, and of these, 3 cases were ascribed to the AL type and 2 to the AA type. 6
Prevalence
Very little data are available about the prevalence of systemic amyloidosis. The prevalence of AA amyloidosis is higher than that of AL amyloidosis in developing countries because of a higher prevalence of associated underlying infectious diseases and AL amyloidosis is the most prevalent in the developed countries. 15
The estimated prevalence of systemic amyloidosis in the United Kingdom is 20 per million inhabitants. 8
Wild-type ATTR amyloidosis affects 25% of the very old people (over 85 years of age) in Finland, 19 and about 13% of the patients above 60 years having heart failure with preserved ejection fraction were thought to suffer from wild-type ATTR amyloidosis in a Spanish study. 5
Amyloid deposits can affect a variety of organ systems most commonly the kidneys, liver, and heart and can also affect the peripheral motor, sensory, and autonomic nerves but when peripheral neuropathy is the presenting manifestation of amyloidosis, diagnosis is often delayed, as significant time may be spent pursuing more common causes of neuropathy such as diabetes or autoimmune disorders.9,16,18
In AA amyloidosis the usual presentation is kidney disease as reflected by proteinuria or loss of renal function. Autonomic dysfunction may cause abdominal complaints such as diarrhea and disturbed gastric emptying. Hepatomegaly and cardiomyopathy are seen, although infrequently. And peripheral nerve damage is very rare. 10
High-resolution MR imaging helps to identify the characteristic enlarged, irregular nerve appearance that represents the diffuse nerve amyloid infiltration, 20 and ultrasonography can be helpful to mark the site of the nerve biopsy allowing a more targeted approach.
Diagnosis is confirmed based on clinical organ involvement and histological demonstration of amyloid deposits. Diagnosis cannot be confirmed based on the finding of amyloid deposits in an indirect biopsy in the absence of clinical organ involvement or in the presence of a predisposing condition, even with highly elevated amyloidogenic proteins in serum and no histological evidence of organ damage. 15
Tissue diagnosis can be made by biopsy of the abdominal fat or involved organ. Fat biopsy, which was negative in our patient, has a reported sensitivity of 70% to 85%. In nerve amyloidosis, the sural nerve can be taken with a sensitivity of 86% to 90%. 21 But we decided to take a direct biopsy of the radial nerve because no extra-nerve damage would be produced due to longtime denervation.
In amyloidosis, nerve biopsies reveal amyloid deposits in the endoneurial and epineurial connective tissue, along with deposits in the endoneurial and epineurial blood vessel walls. There is a decreased density of all types of nerve fibers with small myelinated and unmyelinated fibers being affected the most. With Congo red staining, amyloid exhibits an apple-green birefringence under polarized light and appears red when viewed under a light microscope. 4
Accumulation of amyloid deposits in nerves can lead to focal, multifocal, or diffuse forms of neuropathy. In hereditary type of ATTR amyloidosis, the carpal tunnel syndrome can be the first presentation of the amyloidosis, and in the acquired wild-type ATTR amyloidosis, that is seen at old age and its cause is unknown, a slowly progressive cardiomyopathy is seen and carpal tunnel syndrome often precedes the clinical picture of cardiomyopathy by a couple of years.1,2,10
Isolated peripheral nerve amyloidosis is an unusual condition, and there are only 2 previously documented cases, both of them in radial nerve and none of which are in AA amyloidosis. Kanta et al 7 describe a case of a limited 6-cm amyloid deposit in the radial nerve, also located in the middle third of the arm, and Cheng et al 3 describe another case of a focal amyloid deposit of 5 to 6 mm in the radial nerve at the level of the lateral epicondyle. In the first case, the amyloid type could not be identified by immunohistochemical analysis, and in the second case, it was determined to be an AL amyloidosis.
The timing of surgery should be based on clinical features and the course of the disease. In the case of an isolated peripheral nerve amyloidosis, it can be managed with curative resection or if a nerve gap is present, by bridging the defect. But if the nerve lesion is all along the nerve, as in our case, with no possible resection, tendon transfers are recommended. 17
However, this treatment option was rejected by our patient.
Footnotes
Ethical Approval
This study was approved by our institutional review board.
Statement of Human and Animal Rights
This article does not contain any studies with human or animal subjects.
Statement of Informed Consent
Informed consent was obtained from all patients for being included in the study. Additional informed consent was obtained from all patients for which identifying information is included in this article. Informed consent was obtained from all individual participants included in the study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.