
Abstract
Introduction
Health is affected by health literacy—the ability to obtain, process, and understand health information to make appropriate health decisions. 7 Ninety million individuals, nearly half of all American adults, fail to meet the Institute of Medicine’s definition of health literate. 13 There is an association between patients with low health literacy and lower adherence to appropriate care, suggested by lower rates of influenza vaccination, control over their asthma, 9 mammography screening, medication adherence, and inability to properly interpret health-related labels and messages.6,29 Furthermore, health disparities correlate with race and socioeconomic factors.8,10,12,30 Overall, patients with lower health literacy have greater health care utilization and expenditure 26 but increased risk of hospitalization, complications, and death.5,14,20,28
Because low health literacy is associated with decreased medical knowledge, and poorer health-related outcomes, one might expect that patients with lower levels of healthy literacy would spend more time with physicians to compensate for these known limitations. However, in hand surgery, patients with limited health literacy have shorter visits. 18 Patients with limited health literacy have less medical knowledge 24 and are limited in their ability to complete necessary administrative tasks such as scheduling appointments, filling out insurance forms, and following instructions for diagnostic procedures, treatment, and postoperative care. 15 These limitations could lead to a greater amount of time between scheduling an appointment and seeing the physician, travel time to see the physician, and overall time seeking care.
This study tested the primary null hypothesis that there is no correlation between health literacy and total time spent seeking hand surgery care accounting for other factors. In addition, we addressed the secondary null hypotheses that: (1) there is no correlation between health literacy and time from booking until appointment accounting for other factors; (2) there are no factors associated with variation in (a) total time spent seeking hand surgery care, (b) travel time, (c) waiting time in the office, (d) face-to-face time, and (e) time from booking until appointment; (3) there are no factors associated with patient satisfaction; and (4) there are no factors associated with Patient-Reported Outcomes Measurement Information System (PROMIS) upper extremity (UE) function.
Materials and Methods
Study Design
In this prospective cross-sectional, institutional review board–approved study, new patients seeking hand surgery care at a suburban academic medical center were asked to complete a questionnaire directly after their visit at a hand surgery clinic. The hand surgery clinic involved in our study serves a small city with a population of 85 288 people, as well as the surrounding area. 31 Also, in the United States, there are 0.64 hand surgeons per 100 000 people; this ratio is consistent within the state in which our clinic is located. 27
Explanatory variables collected included age, sex, socioeconomic elements (race/ethnicity, health insurance, years of education, work status, marital status, annual salary), means of transportation, presence of a companion, reason for visit (trauma or nontrauma), whether visit was a second opinion, whether another office was initially contacted first, and outcome instruments (PROMIS pain interference, 1 PROMIS depression, 25 PROMIS UE function 11 ), satisfaction, and health literacy. Health literacy scores were measured using Newest Vital Signs (NVS) test 32 and dichotomized to limited (0-3) versus adequate (4-6) health literacy. Descriptive statistics were calculated for patients in each of the original 3 levels of scoring on the NVS test for completeness (0-1, 2-3, 4-6) (Supplemental Table 1). Satisfaction was determined using an 11-point ordinal scale.
Primary response variable was the total time spent seeking hand surgery care, defined as time spent traveling for care (patient self-reported), plus office time (waiting time in the office plus face-to-face time) was collected from the electronic health record and timed during the visit by a researcher. Secondary response variables included travel time, waiting time in the office, face-to-face time, and time from booking until appointment.
All questions, except for the NVS test, were completed on a tablet or computer (assessmentcenter.net). A researcher read NVS questions out loud to the patient and completed the documentation on paper. Health literacy was only used for research purposes. No measures were taken based on the health literacy score outcomes. No identifiable information was recorded.
Inclusion criteria for the study were new patient to the clinic, greater than18 years of age, and English fluency and literacy. Exclusion criteria included patients unable to give informed consent, and pregnant women.
Statistical Analysis
An a priori power analysis based on a chi-square test was performed. To detect a 0.30 correlation between health literacy and time spent seeking hand surgery care at an alpha of 0.05 and 90% power, a total sample size of 112 patients was calculated.
Descriptive statistics were calculated for each outcome of interest and shown as the frequency for categorical variables and mean (standard deviation) for continuous variables. Bivariate analyses were conducted to test the association of each explanatory variable with outcomes. Chi-square tests were used for binary categorical variables (eg, sex), a 1-way analysis of variance was used for categorical variables with multiple groups (eg, annual salary), and t tests were used for continuous variables (eg, age). Variables that were associated with a given outcome at a P < .10 level were included in multivariable regressions. Full model pseudo-R2 values were used to determine the variation that could be explained using the model. Pseudo-R2 values from the bivariate analyses were also recorded for each variable in the multivariable regression models to better understand the contribution to variation of each individual factor.
Results
A total of 112 patients participated in this study. There was no correlation between health literacy rate and the total time seeking hand care (Table 1). Accounting for potential confounding in the multivariable analysis, only the presence of a companion was associated with an increase in total time seeking hand care. In bivariate analyses, the presence of a companion and having a nontraumatic diagnosis led to a significant increase in the total time spent seeking care. Also in bivariate analysis, 30 patients (27%) had limited health literacy and an average total time seeking hand surgery care of 118 minutes (SD, 81 minutes), while 82 patients (73%) had an adequate level of health literacy and average total time seeking hand surgery care of 93 minutes (SD, 49 minutes).
Association of Patient Characteristics With Different Times Related to Receiving Hand Surgery Care.
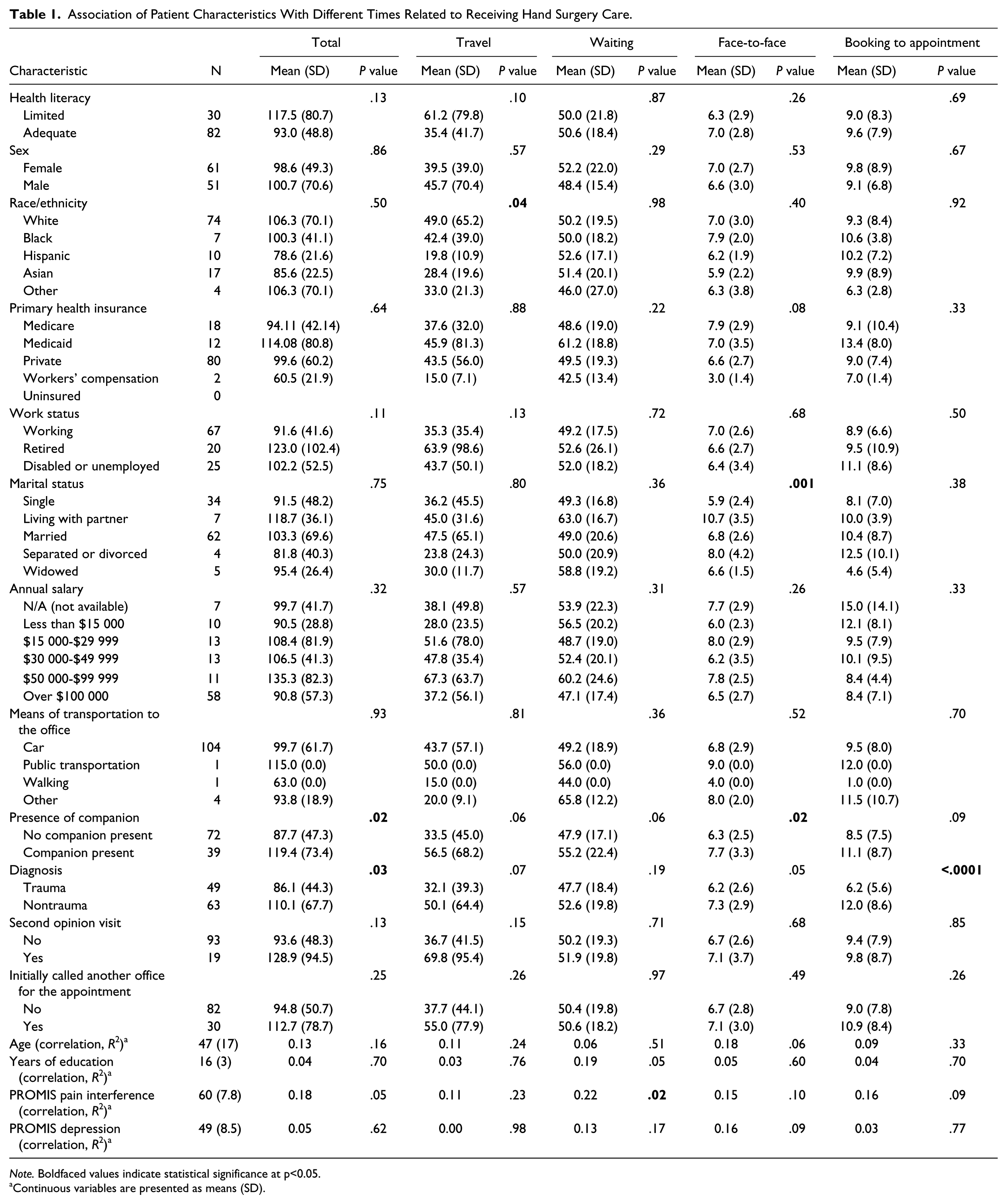
Note. Boldfaced values indicate statistical significance at p<0.05.
Continuous variables are presented as means (SD).
There was not a significant difference in average time from booking an appointment to being seen for patients with limited (9 ±8 days) and adequate health literacy (10 ± 8 days; Table 1). Travel time was associated with race/ethnicity. Time spent in the waiting room was associated with PROMIS pain interference scores. Marital status and presence of a companion was associated with time spent face-to-face with the surgeon. Trauma diagnosis was associated with a shorter time from booking to appointment. In addition to total time seeking hand care, the presence of a companion was the only variable associated with both an increase in travel time and face-to-face time in the multivariable linear regressions (Table 2). No variables were associated with waiting time, booking to appointment time, or patient satisfaction in the multivariable linear regressions. No patient characteristics were associated with patient satisfaction (Table 3).
Factors Independently Associated With Different Times Related to Receiving Hand Surgery Care.
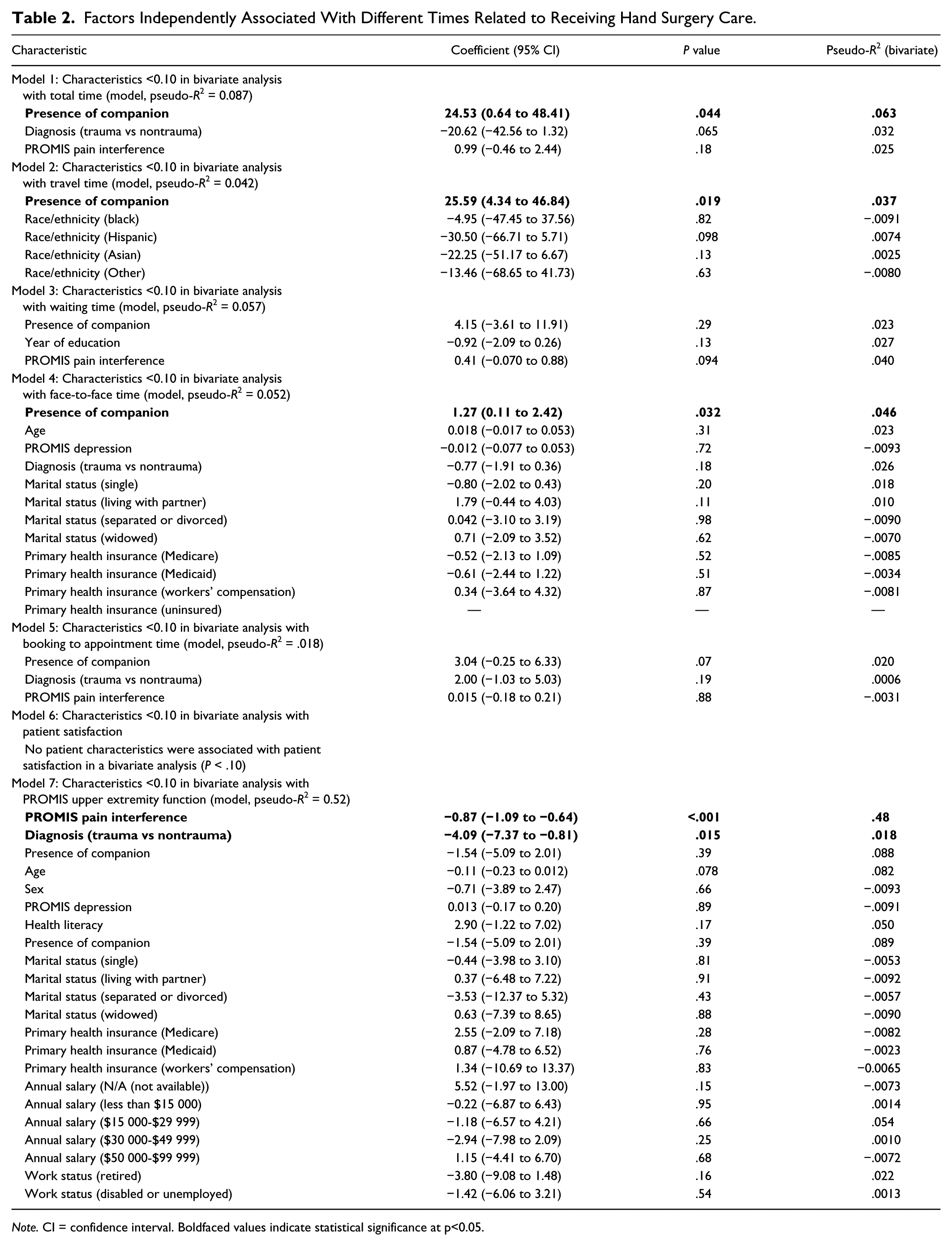
Note. CI = confidence interval. Boldfaced values indicate statistical significance at p<0.05.
Association of Patient Characteristics With Patient Satisfaction.
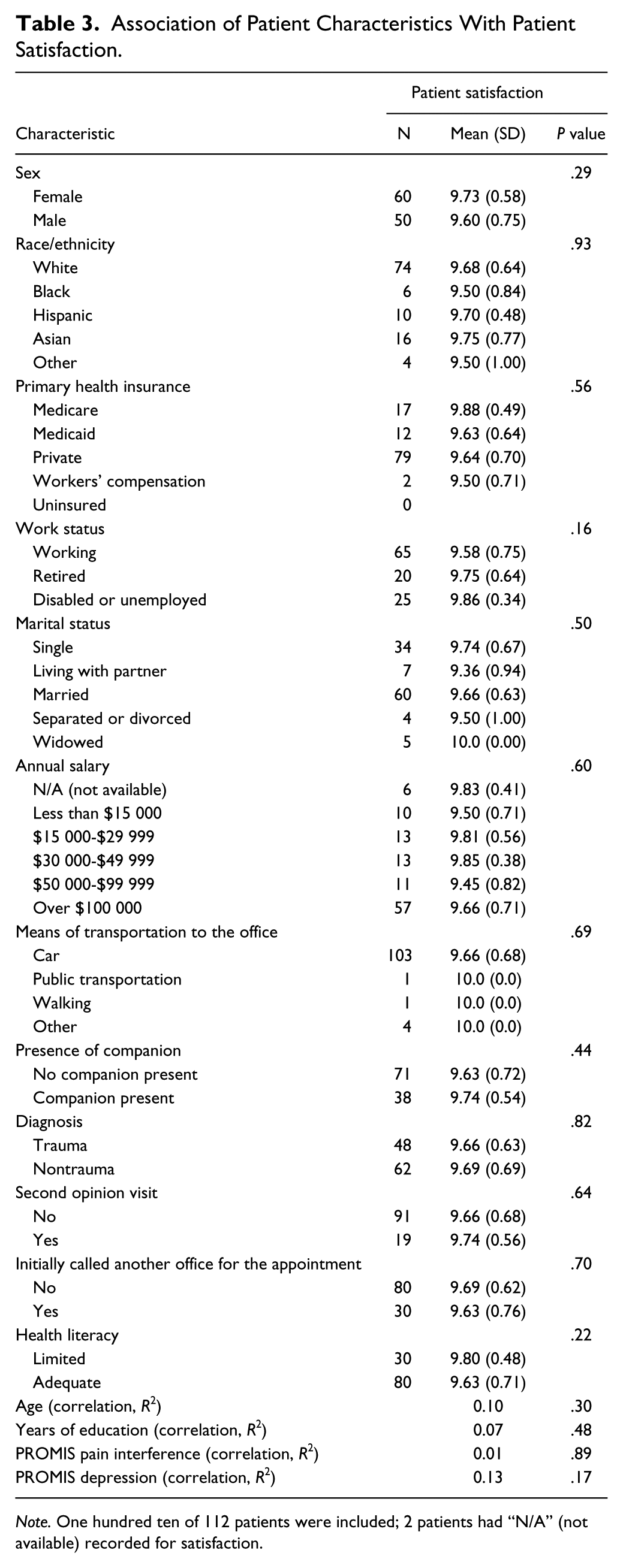
Note. One hundred ten of 112 patients were included; 2 patients had “N/A” (not available) recorded for satisfaction.
In bivariate analysis, patients with private insurance, an annual salary greater then $100 000, presence of a companion at the consultation, adequate health literacy level, age, lower PROMIS pain interference score, and lower PROMIS depression score were all associated with higher PROMIS UE function scores (Table 4). In multivariable analysis, PROMIS pain interference scores and diagnosis (trauma vs nontrauma) were independently associated with PROMIS UE function scores in the multivariable linear regression analysis.
Association of Patient Characteristics With PROMIS UE Function.
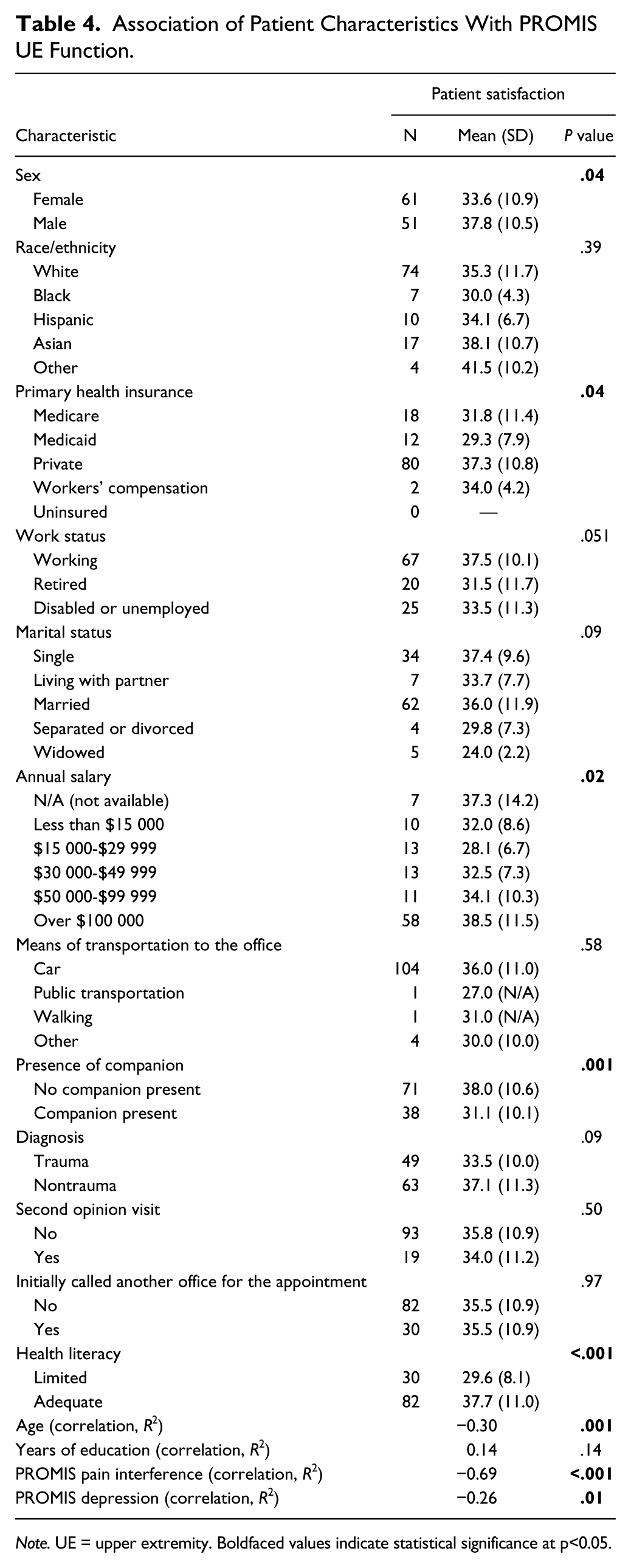
Note. UE = upper extremity. Boldfaced values indicate statistical significance at p<0.05.
Discussion
Health literacy impacts health, and limited health literacy is common among patients seeking hand surgery care 17 ; however, its influence on time spent seeking health care is less well studied. Williams et al previously demonstrated that 42% of the patients tested could not understand directions for taking medication on an empty stomach, 26% could not understand the information on an appointment slip, and 60% could not understand a standard informed consent form. 33 Navigating through the health care system requires a patient to understand times, directions, building and physician names and specialty names, and place the value of these visits in the context of their other illnesses and their lives. Moreover, patients with lower health literacy may be embarrassed by their limitation, do not always ask for help, and develop strategies to hide their limitation.4,15,22 Based on these known associations with limited health literacy, we tested the null hypothesis that there is no correlation between health literacy and total time spent seeking hand surgery care. Based on our results from a suburban academic medical center, we could not reject the null hypothesis.
We found that health literacy did not affect the time from booking an appointment to being seen by a physician. Previous work within internal medicine has also shown that limited health literacy is not associated with the time to first visit. 3 We postulate that this may be secondary to increased use of electronic health systems that track patient referrals, as well as increased opportunities for verbal instructions on appointment times and locations. We also found that the presence of a companion increased the total time seeking hand surgery care by 36% and face-to-face time with the attending surgeon by 22%. Living with a partner also increased face-to-face time with the physician. Previous research has shown that having a companion (eg, family member) in a consultation with the patient increases the length of a visit by approximately 20%. 34 However, the same meta-analysis showed that longer visits and companion accompaniment to office visits do not necessarily lead to better care. 34
Patients with nontraumatic hand injuries had a longer total time seeking hand surgery care compared with those with traumatic injuries. Given the elective nature of nontraumatic injuries, it makes sense that neither health system nor physician would prioritize these visits over traumatic injuries. As expected, having a traumatic injury led to decreased time from booking an appointment to receiving a consult.
No factors studied were associated with patient satisfaction. This is supported by a study by Parrish et al, which showed that patient satisfaction with hand surgery care is not associated with visit duration in hand surgery. 23 In contrast, Anderson et al showed that time spent with a physician is a predictor for patient satisfaction in primary care. 2 In hand surgery, satisfaction is strongly correlated with patient-rated surgeon empathy. 16
The observation that maladaptive coping strategies (pain interference) is the strongest correlate of UE specific limitations is consistent with prior research. 21 The bivariate analysis implies that greater income and private insurance (socioeconomic measures) diminish limitations and are confounded with more effective coping strategies (because they were not independently associated with lower PROMIS UE function scores). Greater attention of efforts to optimize coping strategies and limit stress and distress are merited. 19
Our study results should be viewed with the following limitations kept in mind. First, our study results come from a suburban academic hand surgery clinic within the United States; therefore, the results may not be generalizable to all populations and practice types. Second, only new patients to the clinic were included to limit any relationship bias that may have been built between previous interactions between the physician and patients. Third, whether patients were self-referred for care or referred by a primary care provider (PCP) was not recorded. Patients referred by a PCP may be able to seek hand care more quickly due to their involvement in the health care system already regardless of health literacy levels. Fourth, we excluded patients who did not speak English because of the languages available for our questionnaire. This may bias our result as we suspect unfamiliarity with language may be correlated with limited health literacy. Therefore, our results may be different if all patients, regardless of language, were included. Fifth, because we focused on a limited number of physicians in one academic medical center, we were unable to control for physician characteristics or health system characteristics in our analyses. Last, time spent traveling for care was self-reported and might be inaccurate and susceptible to recall bias.
Our findings suggest that navigating the numerous steps involved from initial inquiry for an appointment, to being seen, is not dependent on how well an individual understands health information. Future work may analyze correlations between health literacy and other surgical outcome measurements, including infection rates and pain levels. In addition, correlations between health literacy and the number of occupational therapy visits may also offer valuable insight into the impact of health literacy on postoperative recovery. Additional research could compare the impact of health literacy on trauma versus elective hand surgery care. Last, hand surgery clinics in other practice settings, such as urban and public health systems, safety-net clinics, and rural nonacademic health systems should be studied.
Footnotes
Supplemental material is available in the online version of the article.
Ethical Approval
The institutional review board of Stanford University approved this study under Protocol ID: 36003; IRB Number: 6208 (Panel: 8).
Statement of Human and Animal Rights
All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2008.
Statement of Informed Consent
Informed consent was obtained from all individual participants included in the study.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: DR received royalties from Tornier (formerly Wright Medical): Elbow Plates (received <$10 000/year) and Skeletal Dynamics: Internal Joint Stabilizer Elbow (contract; nothing received). He received research grant support from Skeletal Dynamics ($50 000). He is deputy editor for hand and wrist, Journal of Orthopaedic Trauma (volunteer) and deputy editor for hand and wrist, Clinical Orthopaedics and Related Research ($5000/year). He received honoraria from AO North America, AO International, and various hospitals and universities. All other authors (RK, DB, AA, NS, LU) certify that they have no commercial associations (eg, consultancies, stock ownership, equity interest, patent/licensing arrangements, etc) that might pose a conflict of interest in connection with the submitted article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.