
Abstract
Introduction
The radial artery is frequently accessed in a wide range of clinical settings, from the hemodynamically unstable critically ill patient requiring frequent blood draws or arterial lines to elective outpatient procedures. Transradial cardiac catheterization has been on the rise in use due to its benefits of increased patient comfort, early time for ambulation, reduced length of stay, and decreased vascular complications compared with femoral access.1-3 Fortunately, radial artery injury is rare and often asymptomatic, as most patients have ulnar dominant vasculature to the hand. However, up to 4% of patients may have radial artery dominance. 1 , 2 Slogoff et al 2 examined 1699 patients at the Texas Heart Institute and found abnormal flow in 21.2% of patients 1 day after cannula removal; however, only 4 patients (0.24%) had symptoms.
Reported complications after transradial cannulation include hematoma, perforation, artery spasm, artery occlusion, emboli, pseudoaneurysm, and even forearm compartment syndrome. 4 Some of these conditions may be self-limiting, not requiring intervention, but others may require urgent treatment to prevent permanent tissue loss or sensorimotor deficits.
The guidelines for the management of iatrogenic radial artery injuries have not been well described. The purpose of our study was to retrospectively identify those patients developing complications from radial artery access, presenting symptoms, and treatment modalities to help guide decision making regarding iatrogenic radial artery injuries.
Methods
A retrospective chart review was performed from 2008 to 2018 at a single tertiary academic institution. Patients with radial artery injuries were identified by International Classification of Disease (ICD) code 903.2 and cross-referenced with patients having undergone arterial line placement or radial artery access for heart catheterization. Traumatic injuries and injuries to ulnar, brachial, and axillary arteries were excluded. Patient demographics, index procedure resulting in injury, presenting symptoms, timing of presentation, diagnostic procedures performed, management, and outcomes were collected and analyzed. Statistical analysis was performed using SPSS software. Values of P < .05 were considered statistically significant.
Results
Eighteen patients with iatrogenic radial artery injuries were identified between the years 2008 and 2018. Six of these patients (33%) presented with a pseudoaneurysm of the radial artery. The remaining 12 patients (66%) presented with signs consistent with radial artery thrombosis (RAT).
Radial Artery Pseudoaneurysm
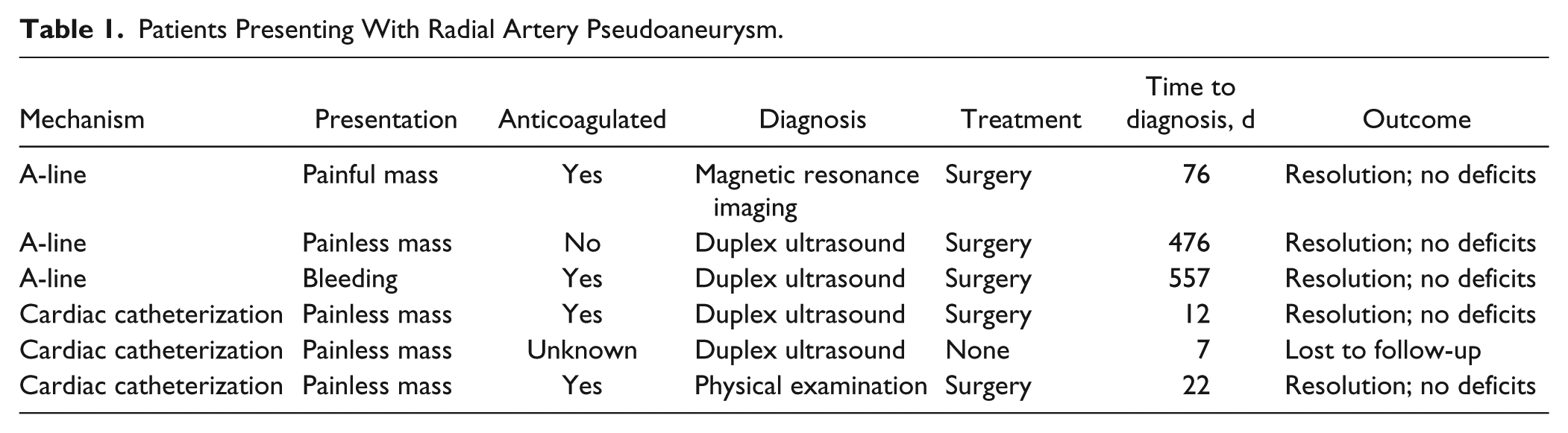
Of the 6 patients who presented with radial artery pseudoaneurysm (RAP), 50% were the result of arterial line cannulation, and 50% occurred after cardiac catheterization (Table 1). Four of the 6 patients presented with a painless mass at the wrist. One patient presented with a painful mass at the wrist. One patient presented with bleeding from his arterial line site. No patients had any sensorimotor deficits or signs of tissue compromise. Four patients had diagnosis confirmed with duplex ultrasound, 1 by magnetic resonance imaging, and 1 by physical examination alone. Four of the 6 patients were on therapeutic anticoagulation at the time of intervention. In one patient, the anticoagulation status was unknown, and one patient was not anticoagulated. Five patients underwent operative intervention. Operations performed included excision of pseudoaneurysm with ligation of the radial artery versus primary end-to-end repair. One patient did not undergo surgical intervention and was lost to follow-up. All 5 patients who underwent surgical intervention had resolution of their symptoms and did not have any sensorimotor deficits on follow-up evaluations (2 weeks to 1 year). Of note, there was a wide range of time to diagnosis after radial artery intervention (7-557 days, mean = 191.7 days).
Patients Presenting With Radial Artery Pseudoaneurysm.
Radial Artery Thrombosis
Of the 12 patients who presented with RAT, 50% were after arterial line cannulation, and 50% were caused by cardiac catheterization (Table 2). Six patients presented with hard signs of vascular injury with loss of radial pulse or Doppler signal, or with tissue loss. One patient had tissue sloughing; however, this patient was also on vasopressors. Two patients complained of pain and cyanosis, 2 patients demonstrated sensorimotor deficits of the hand and fingers, and 2 patients complained of pain alone. Five patients had diagnosis confirmed with duplex ultrasound, 4 with angiogram, 2 with physical examination alone, and 1 with magnetic resonance angiography.
Patients Presenting With Radial Artery Thrombosis.
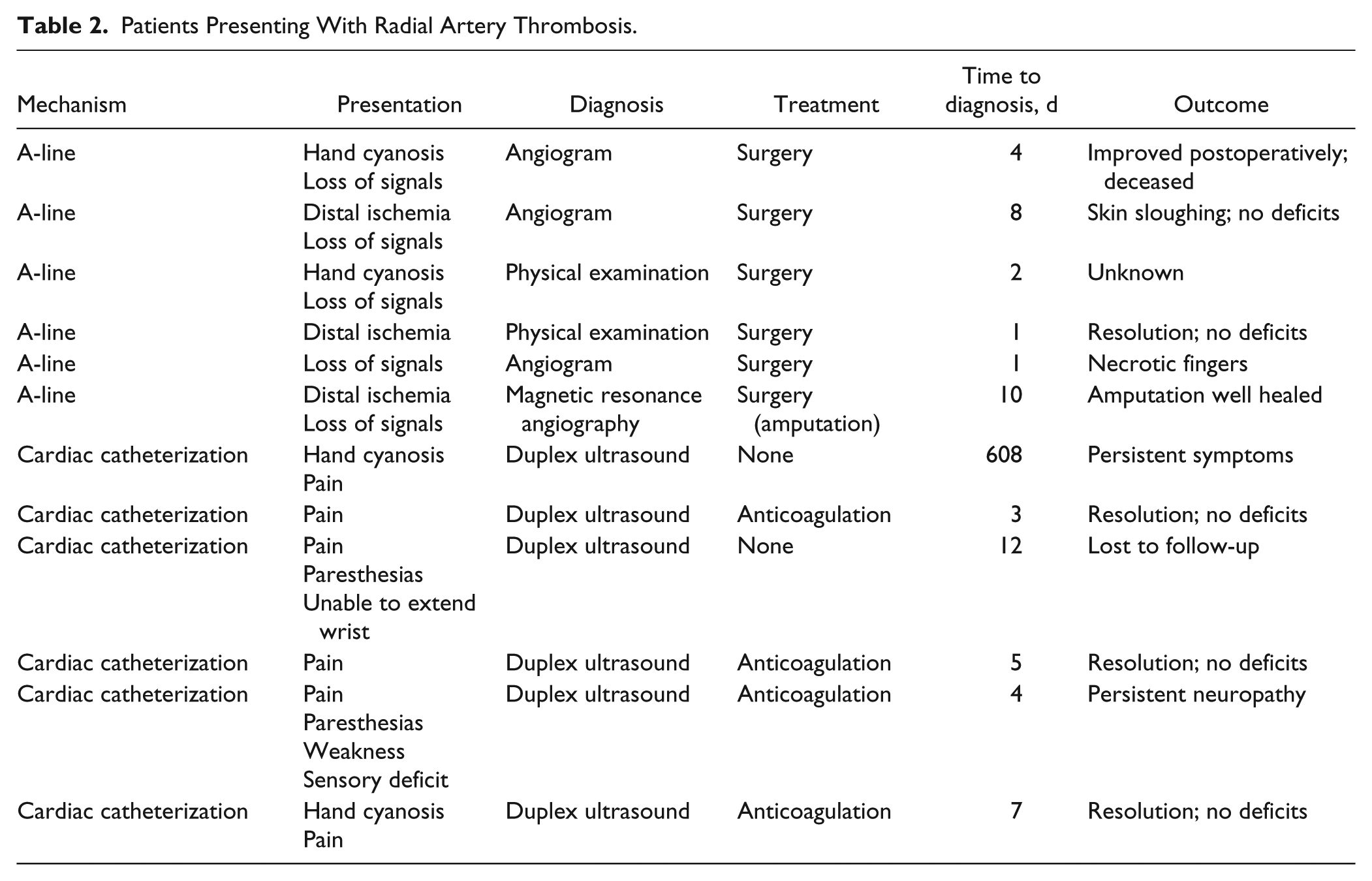
The 6 patients with hard signs of vascular injury underwent surgical intervention, which included open thrombectomy and resection of injured artery with primary repair in 4 patients and thrombectomy with interposition vein graft in 1 patient. The patient on vasopressors with tissue loss underwent amputation through the radiocarpal joint and healed well. Two patients had initially improved perfusion postoperatively but died in the intensive care unit. Two patients regained perfusion postoperatively with full recovery, and one patient was lost to follow-up.
Four patients with soft signs of vascular injury received 3 months of therapeutic anticoagulation. Three patients reported complete resolution of symptoms. One patient had continued pain but had improved strength in his hand and refused any further intervention.
Two patients were treated conservatively, without an operation or anticoagulation. Of these patients, one reported persistent wrist pain and one was lost to follow-up.
Time to diagnosis after initial radial artery intervention ranged from 1 to 608 days, with an outlier of 608 days. After removing the outlier, the average time to diagnosis was 5.2 days after radial artery intervention.
Discussion
The increase in cardiovascular disease in the United States has led to a similar increase in the number of percutaneous procedures being performed annually.1,2 The radial artery has more recently become the access method of choice for many of these procedures. 4 Although radial artery injuries are uncommon after cannulation procedures, the true incidence is likely unknown as many of these injuries remain asymptomatic. 2 When injury does occur, it puts the patient at risk of irreversible sensorimotor deficits and tissue loss. Kanei et al 5 estimated the prevalence of radial artery occlusion after catheterization to range between 2% and 18%. Stella et al 6 reported that 5.3% of patients had clinical evidence of radial artery occlusion immediately following a transradial catheter procedure, and roughly 3% of patients had clinical evidence of this persist beyond 1 month after discharge. Critical hand ischemia following radial artery cannulation is a rare occurrence, with a reported estimate of 0.09% in the literature. 7 , 8 Our study identified 2 distinct presentations of symptomatic iatrogenic radial artery injuries: RAP and RAT.
Upper extremity pseudoaneurysms are rare and have been documented to occur at an incidence of 0.009% after cardiac catheterizations. 9 In our study, 4 out of 6 patients who developed pseudoaneurysms were fully anticoagulated at the time of intervention. This was consistent with a case series by Collins et al, 10 who found that 80% of patients who developed RAP after transradial cardiac intervention were also fully anticoagulated. In their study, a TR band or a RadStop device was applied after the procedure and used as directed by their respective companies. This is thought to occur, as these patients are more prone to artery perforation and hematoma at the time of procedure, likely leading to increased risk of pseudoaneurysm. 5 Documentation in our study did not elucidate whether an occlusive dressing was used after procedure.
Most patients (83%) presenting with RAP underwent surgical management with complete resolution of their symptoms. This was similar to a study by Tosti et al. They identified 11 patients with RAP. Half resulted from arterial lines and the other half from cardiac procedures. Four patients with lesions smaller than 3 cm spontaneously resolved at a mean of 27 days. The remaining 7 patients (63%) underwent surgery with excision of the stalk and repair of the artery. All patients had resolution of their symptoms, and only one patient required emergent surgery for acute carpal tunnel syndrome. 11 Garg et al reviewed their series of 30 patients with radial artery complications after indwelling catheters. They identified 10 patients with pseudoaneurysms. All patients underwent surgery. Five patients had excision of the aneurysms and repair of the artery, 4 had radial artery ligation, and 1 required a vein patch angioplasty. 12
Our study uniquely demonstrates a wide range in time between intervention and diagnosis of pseudoaneurysm. Two patients were extreme outliers with time to diagnosis over 1 year. Previous reports documented that most pseudoaneurysms present within a week of the procedure. 3
Radial artery thrombosis after percutaneous access has a higher incidence when compared with pseudoaneurysm. However, this complication is not always symptomatic and does not become clinically obvious. Following radial artery cannula removal, screening duplex has shown a 10% to 18% incidence of RAT. 1 , 5 Interestingly, 1 month after transradial catheterization, 34.8% of patients with thrombosis were found to have spontaneously recanalized. These patients were followed for up to 6 months, and even the 5.1% with persistent RAT remained asymptomatic. 1 This demonstrates iatrogenic radial artery injury is a largely underreported problem. These asymptomatic patients with persistent thrombosis must have sufficient blood flow from the dominant ulnar artery. Performing an Allen test prior to radial arterial catheterization may help identify the 4% of patients with radial artery dominant flow and prevent symptomatic radial artery injury. 2
Valentine et al reported their experience with 8 patients who developed RAT and signs of digit or hand ischemia after arterial cannulation for hemodynamic monitoring over a 5-year period. The mean ischemia time was 3 days, and all diagnoses were confirmed with duplex ultrasound or anteriography. Five patients underwent surgical thrombectomy, 4 of whom required patch angioplasty and 1 vein graft interposition. Two patients were treated nonoperatively with vasodilators, and one was observed. 13 Mandel retrospectively reviewed 1000 patients with radial artery cannulations and found only 2 major thrombotic complications requiring embolectomy in one patient and arterial reconstruction in another. 14 Digit and hand ischemia requiring amputations in the setting of arterial cannulation are extremely rare but do occur in the severely ill patients usually in the setting of other comorbidities. Several studies have shown diabetes, Raynaud phenomenon, current smokers, and peripheral vascular disease to be risk factors for RAT, and these patients should be approached with caution. 15 In our study, we did have one patient require hand amputation at the radiocarpal joint. This patient was severely ill on vasopressor support with multiple comorbidities, including hypertension, diabetes, and immunosuppression with a history or renal transplant.
Four patients in our series with soft signs of RAT (pain and discoloration at the finger tips) were treated with anticoagulation for 3 months after RAT was confirmed using duplex ultrasound. The use of anticoagulation in symptomatic RAT has shown promising results in the literature. In a prospective study from Zankl et al, patients were screened by ultrasound 1 day after transradial coronary angiography. They identified 10.5% had RAT, and of these patients, only 58.8% had symptoms. These patients were put on 4 weeks of low-molecular-weight heparin, with 86.7% of patients developing partial or complete recanalization of the radial artery. 16
As there are no current guidelines for evaluating and treating iatrogenic radial artery injuries, we propose the following algorithm (Figure 1). When evaluating patients with suspected iatrogenic radial artery injury, we recommend using duplex ultrasound as the first-line imaging modality. It can accurately diagnose both pseudoaneurysm and thrombosis. All the patients in our series who were evaluated with duplex did not need any further workup. Pseudoaneurysms that do not resolve spontaneously within 3 weeks, are larger than 2 to 3 cm, or cause persistent pain can safely be treated with surgical excision and repair of the artery. Patients with RAT should be evaluated for hard signs of vascular injury. If present, these patients require surgical intervention with open thrombectomy and repair of the artery primarily, and vein patch or vein grafting when extensive injury exists. This requires a detailed physical examination and palpation of the distal digits and palmar arch for Doppler signals. Those with soft signs may be treated with 3 months of anticoagulation with resolution of symptoms.
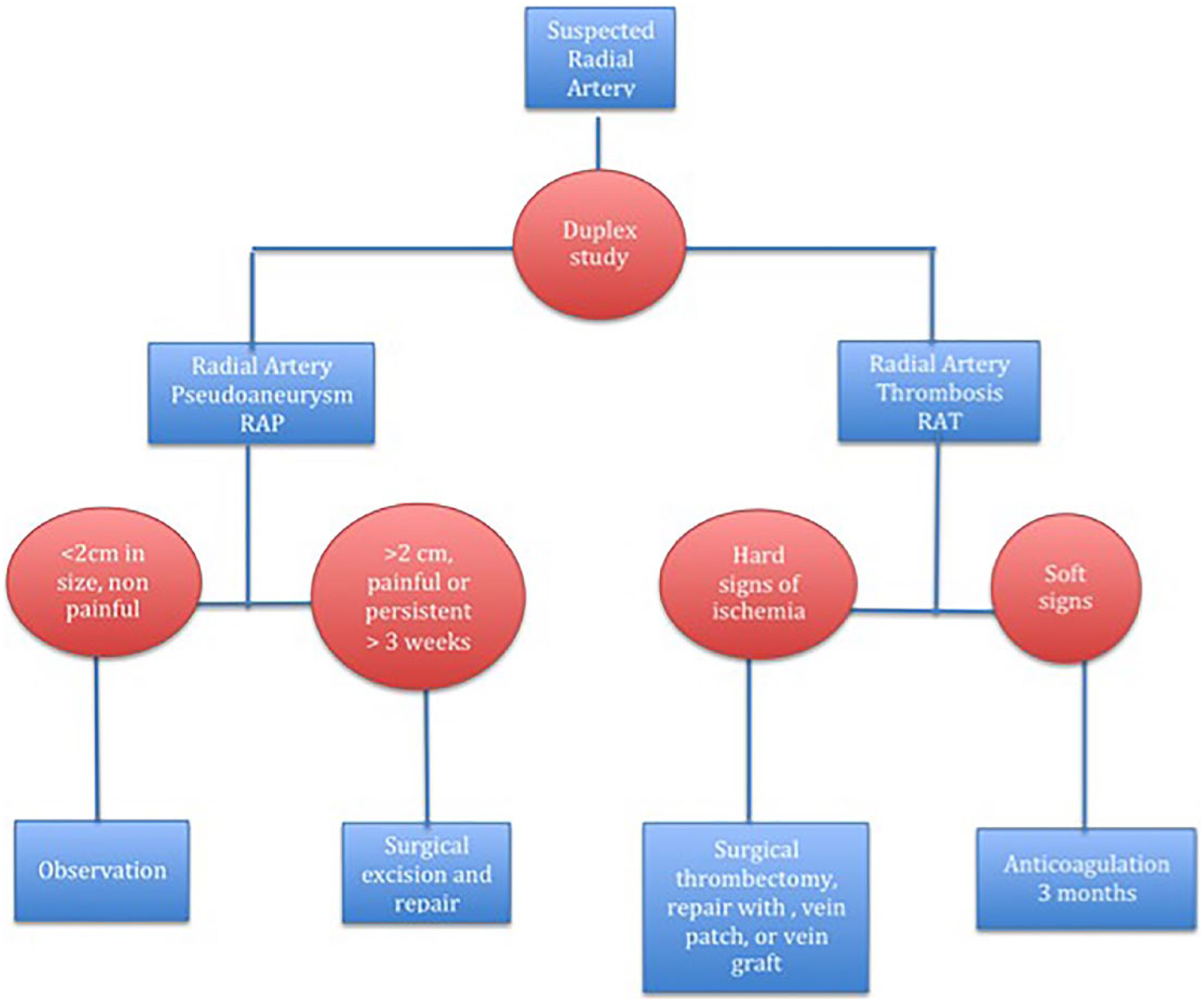
Treatment algorithm for iatrogenic radial artery injury.
Our study has several limitations; these include the fact that this was a retrospective chart review. Our data were captured by chart review using specific ICD and Current Procedural Terminology codes for documented injuries that required surgical treatment. There are likely many cases that may not have been captured using this method. We must also rely on appropriate and detailed documentation, which may be deficient in some cases. The injury may also go unnoticed and resolve without intervention, thus making it difficult to know the true incidence.
Conclusion
Iatrogenic radial artery injury is fortunately a rare event. With the increasing use of transradial cardiac catheterization, the incidence of injuries is likely to rise. With proper and timely diagnosis, the patient may undergo appropriate treatment to prevent permanent sensorimotor deficits or tissue loss.
Footnotes
Ethical Approval
This study was approved by our institutional review board.
Statement of Human and Animal Rights
All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2008. Informed consent was obtained from all patients for being included in the study.
Statement of Informed Consent
Authors are required to ensure the following guidelines are followed, as recommended by the International Committee of Medical Journal Editors, Uniform Requirements for Manuscripts Submitted to Biomedical Journals. “Informed consent was obtained from all individual participants included in the study.”
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.