
Abstract
Background
Traditional dogma regarding management of rheumatoid arthritis (RA) patients with trigger digit symptoms holds that A1 pulley release should be avoided. Surgical release was thought to further destabilize the metacarpophalangeal joint. Biologic disease modifying anti-rheumatic drugs (DMARDs) have limited the development of hand deformities. Despite advances in RA treatment, many textbooks continue to discourage release of the A1 pulley in RA patients. The aim of this study was to determine if this belief is consistent with current trends in surgical management of trigger digits in patients with RA.
Methods
Active Members of the American Society for Surgery of the Hand (ASSH) were surveyed on their training and current practices as related to RA patients with trigger digits.
Results
Five hundred three surveys were completed (16% response rate). During training, 55% of ASSH Members were taught to avoid releasing the A1 pulley in RA patients. Seventy-one percent of respondents currently release the A1 pulley in RA patients with no preexisting deformities, no tenosynovial thickening, or if tenosynovectomy and flexor digitorum superficialis slip excision fail to relieve triggering. Forty percent reported that their practice has evolved toward more frequent release of the A1 pulley in RA patients.
Conclusion
The majority of ASSH Active Members were taught during training to avoid surgical release of the A1 pulley in RA patients to prevent acceleration of finger deformities. Indications and contraindications for A1 pulley release are evolving along with the improved natural history of RA associated with the use of biologic DMARDs.
Introduction
Rheumatoid arthritis (RA) is a debilitating disease affecting at least 0.5% to 1% of adults. 1 It is characterized by chronic inflammatory polyarthropathy. Autoantibodies target the synovium leading to intra-articular inflammation with progressive degradation of cartilage, ligaments, and bone. 2 Small joints of the hand are affected in approximately 70% of the RA patients. 3 At the metacarpophalangeal (MCP) joint, chronic synovitis results in attenuation of the capsule, collateral ligaments, and volar plate, with eventual destabilization of the joint. Flexor tendon forces are applied in volar and ulnar vectors, leading to volar subluxation, and ulnar deviation (“drift”) of the proximal phalanx in the setting of a destabilized MCP joint. These deforming forces are exacerbated by the ulnar force vector applied by the extensor tendons in the presence of underlying carpal deformity.4-6
Stenosing flexor tenosynovitis, or trigger finger, is one of the most common hand ailments affecting 2% to 3% of the general population, with higher prevalence among patients with RA.7,8 It most commonly involves the A1 pulley, where friction between the flexor tendon and the tendon sheath leads to metaplasia, thickening, and stenosis that inhibits smooth gliding of the tendon. 9 Patients experience pain, catching sensation, and, in advanced stages, locking of the proximal interphalangeal joint in flexion. Patients with inflammatory diseases such as RA often develop similar symptomatology as a result of tenosynovial thickening or intratendinous nodules.10-12
Surgical release of trigger finger is typically reserved for patients that do not respond to conservative measures.13-15 Releasing the A1 pulley relieves the stenosis but also alters the vector of flexor tendon pull in an ulnar and volar direction. In a nonrheumatoid hand, the forces are redistributed to the collateral ligaments without clinically significant change in the biomechanics of the MCP joint. 16 In the rheumatoid hand, however, chronic inflammation may attenuate the collateral ligaments to such a degree that they cannot withstand this force redistribution. As a result, surgical release of the A1 pulley was thought to accelerate the process of volar subluxation and ulnar deviation of a digit with an unstable MCP joint. For these reasons, literature has discouraged release of the A1 pulley in favor of limited tenosynovectomy in RA patients with symptomatic triggering.17-28
The implementation of early, aggressive medical therapy has drastically changed the natural history of RA and prevents the onset of debilitating hand deformities.2,29 Despite these remarkable outcomes with medical treatment alone, the dogma of A1 pulley preservation persists in recent hand surgery textbooks.6,12,30-32 Delaying or avoiding adequate surgical treatment of such a prevalent hand problem due to unchallenged dogma has the potential to negatively affect many patients. The aim of this study was to better understand the clinical decision making of hand surgeons with regard to the treatment of RA patients with trigger finger symptoms. We surveyed Active Members of the American Society for Surgery of the Hand (ASSH) as to their training, current practice, and experience in treatment of the RA patient with stenosing tenosynovitis. We hypothesized that hand surgeons’ clinical practices will have evolved in response to the altered presentation of RA patients resulting from the implementation of treatment with biologic disease modifying anti-rheumatic drugs (DMARDs).
Methods
The proposed study was approved by our institutional review board as well as the research division of the ASSH. An 18-question online survey was created using the TypeForm electronic survey tool (www.typeform.com). A brief introductory cover letter and a link to the survey were distributed electronically to all 3167 Active Members using the ASSH Listserv. The survey was available for 3 months, with 1 follow-up email sent to the members as a reminder. Not all questions were answered by all participants as branching logic was used to avoid questions not applicable to each individual responder. The first series of questions focused on surgeons’ training and current management preferences for trigger fingers in patients with RA. The second series focused on whether the surgeon’s practice has evolved over time and on possible experience with poor outcomes attributable to A1 pulley release. Demographic data included gender, practice type, region of practice, and number of years in practice.
Descriptive statistics were generated from demographic information. Chi-square, row means score, or Mantel-Haenszel chi-square test were performed to explore associations between surgeon characteristics and responses, as appropriate. Incomplete surveys were excluded from data analysis and a P-value less than .05 was considered significant.
Results
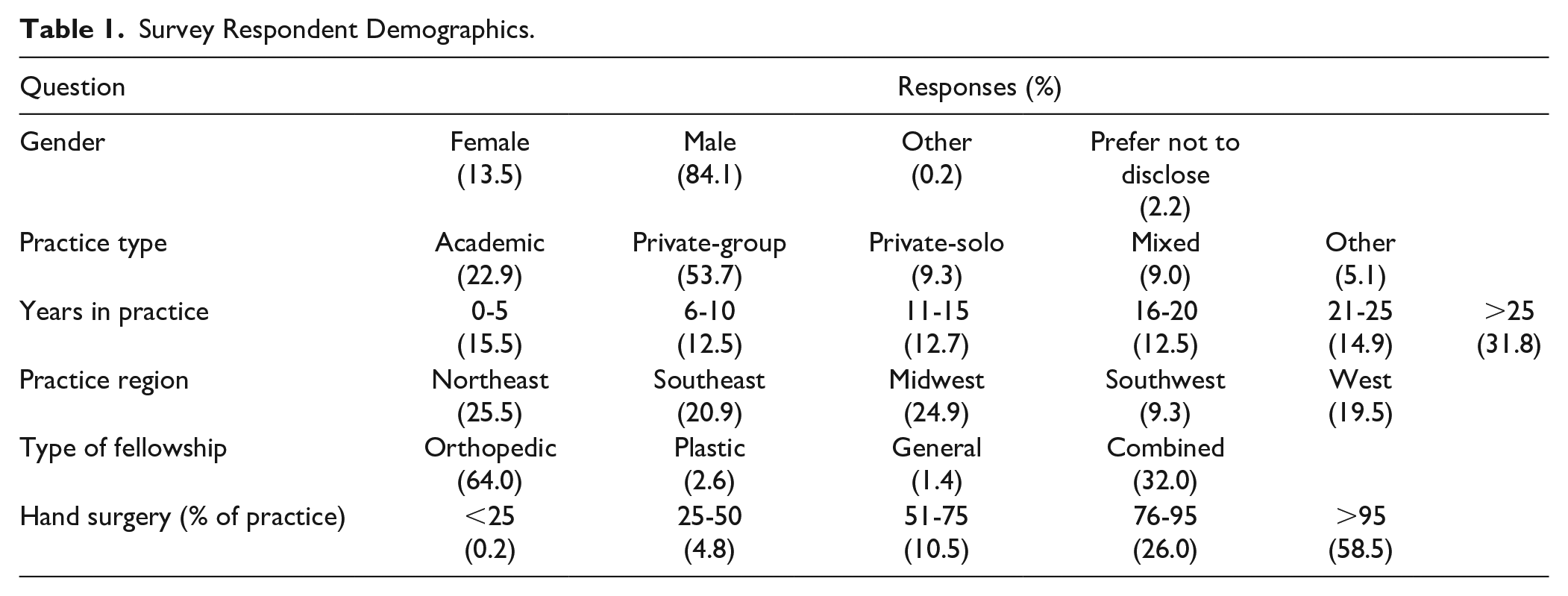
A total of 503 ASSH Active Members completed the survey for a response rate of 16%. Demographic data are displayed in Table 1. The majority of respondents (58%) practiced hand surgery almost exclusively (>95% of practice) while another 26% reported that hand surgery comprised more than 75% of their practice. Sixty percent of respondents had more than 15 years of experience.
Survey Respondent Demographics.
Fifty-five percent of respondents reported that they were trained to either avoid releasing the A1 pulley (43%) or to never release it (12%) if patients carried a diagnosis of RA. Conversely, 38% were trained to treat these patients no differently than patients without RA. Surgeons with more experience (and therefore earlier training) were more likely to have been taught to avoid releasing the A1 pulley (P = .003) (Figure 1). Of those taught to preserve the A1 pulley, their training was based on the belief that preservation of the A1 pulley prevented ulnar deviation (64%), MCP volar subluxation (3%), or both (31%). Those trained to avoid releasing the A1 pulley treat the triggering by tenosynovectomy alone (19%), tenosynovectomy followed by flexor digitorum superficialis (FDS) slip excision as needed (61%), or tenosynovectomy with routine FDS slip excision (11%).
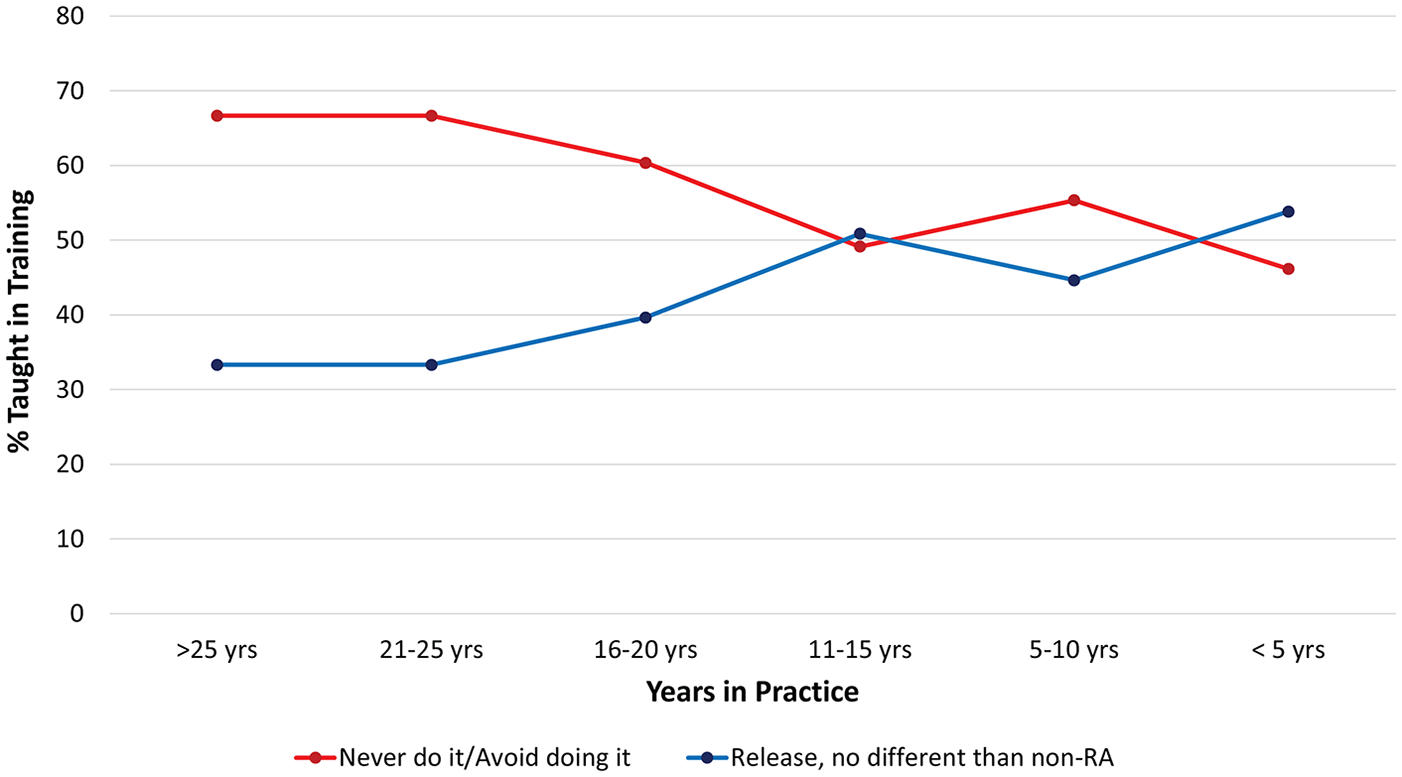
Demonstrates how training of hand surgeons has evolved over time regarding management of the A1 pulley to correct trigger finger in RA patients.
Fifty-four percent of respondents have not altered the way they manage trigger fingers in RA patients over the course of their career. Of these 272 hand surgeons, 58% release the A1 pulley in RA patients just as they would in a patient without RA. Forty-one percent of respondents are now more likely to release the A1 pulley in RA patients. Of the surgeons in practice for less than 10 years, 23% are more likely to release the A1 pulley in their current practice. Forty-nine percent of surgeons in practice more than 20 years and 44% of surgeons in practice 10 to 20 years and are now more likely to release the A1 pulley in RA patients. Surgeons with more experience (and therefore presumably earlier training) were significantly more likely to have altered their practice over the course of their career (P < .0001). Overall, in their current practice, 71% of surgeons release the A1 pulley in RA patients under certain conditions. Reported indications included absence of obvious hand deformity (38%), absence of significant tenosynovial thickening (14%), continued triggering after tenosynovectomy (9%), or FDS slip excision (8%). With regard to their contraindications, surgeons listed preexisting ulnar drift/deviation (75%), MCP subluxation (35%), any hand deformity (21%), or tenosynovial thickening (21%).
Fifty-three percent of the respondents apply the same principles with systemic lupus erythematosus (SLE) patients that they use in patients with RA. Twenty-two percent are more likely to release A1 in SLE patients than RA patients, and 2% are less likely to release A1 in patients with SLE.
Twelve percent of responding members had experience managing a patient with RA who developed ulnar drift attributable to A1 pulley release (performed by them or another surgeon) (Figure 2). Seven percent reported MCP subluxation in an RA patient attributable to A1 pulley release (Figure 3). Of those who indicated they release the A1 pulley routinely or under certain conditions, 8.6% had seen patients develop ulnar deviation and 4.1% MCP subluxation, though it was not specified if this occurred in patients treated according to their stated indications. Surgeons with more experience were more likely to have treated patients with secondary ulnar deviation (P = .0004) or MCP subluxation (P = .02). Of surgeons that had encountered ulnar deviation or MCP subluxation due to A1 pulley release, 52% have not changed their practice, 16% are less likely to release the A1 pulley, and 32% are more likely to release the A1 pulley today. The majority of respondents reported a decrease in the total number of hand procedures performed on patients due to RA, with 64% reporting a decrease in volume of more than 50%. Forty percent reported a decrease in volume of greater than 75%.
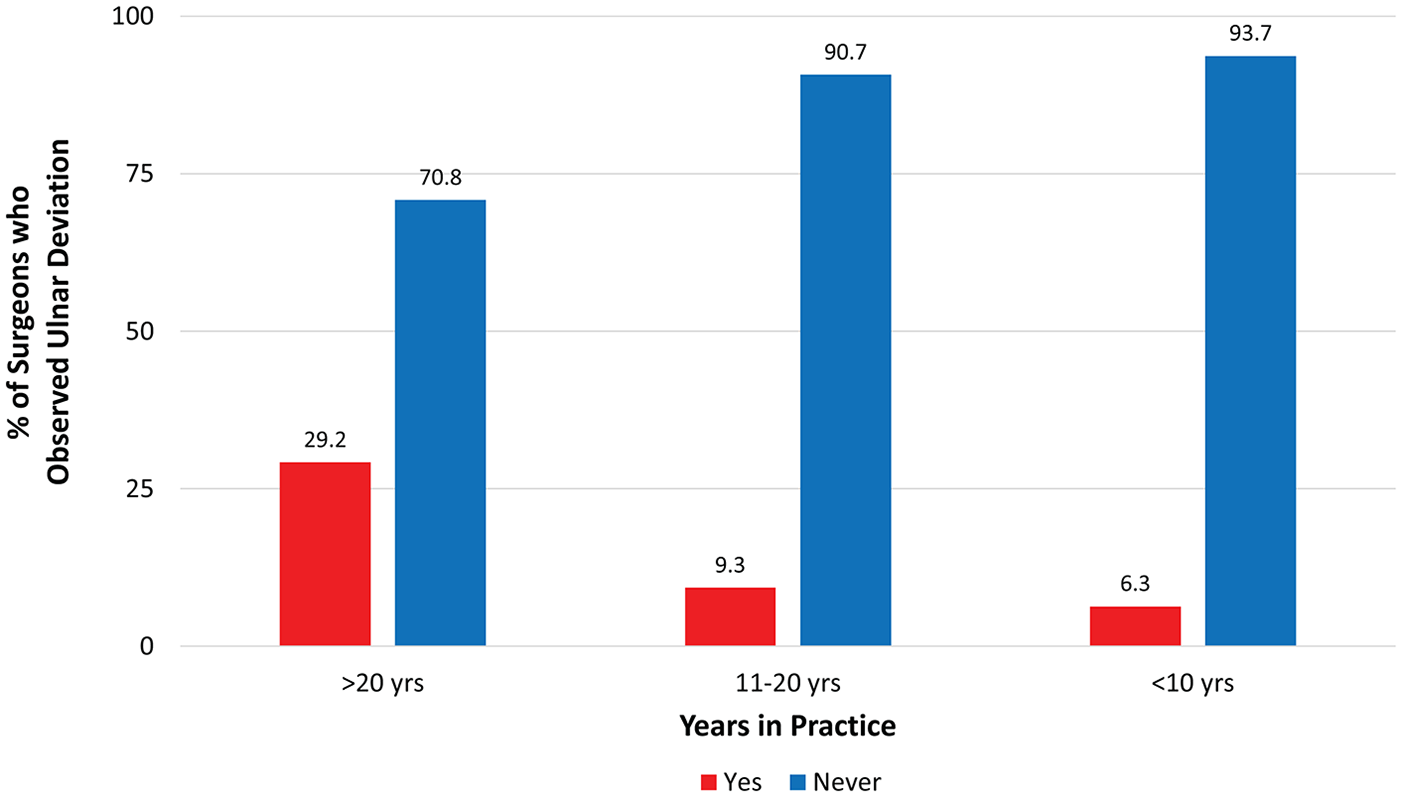
Illustrates the percentage of surgeons who had observed ulnar deviation which they attributed to A1 pulley release in patients with rheumatoid arthritis, as related to years in practice.
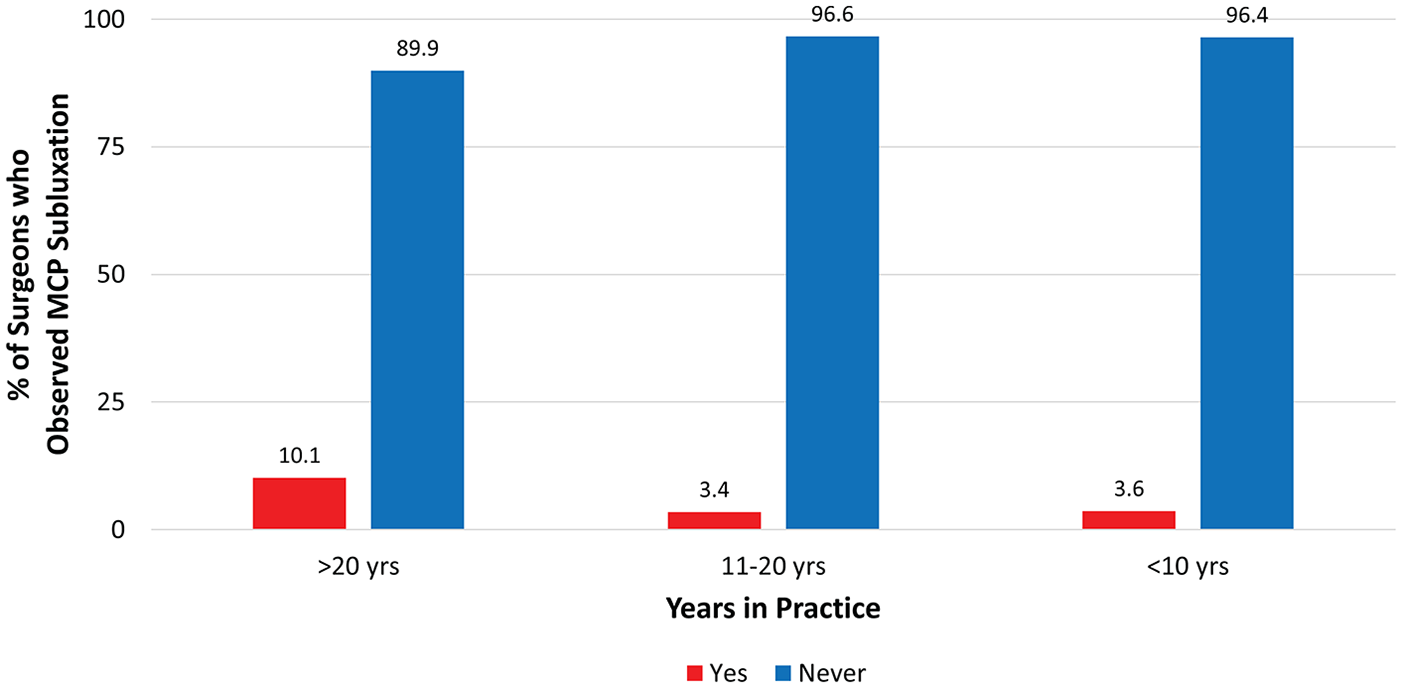
Illustrates the percentage of surgeons who had observed MCP subluxation which they attributed to A1 pulley release in patients with rheumatoid arthritis, as related to years in practice.
Discussion
Prior to the introduction of modern medical therapy (DMARDs), the literature strongly advocated for preservation of the A1 pulley in favor of tenosynovectomy and/or FDS slip excision when treating trigger digits in patients with RA.17,21,26,33 Chronic inflammation in these patients caused tenosynovial thickening, but also collateral ligament laxity and destabilization of the MCP joint. Release of the A1 pulley in these patients was therefore thought to accelerate ulnar deviation and volar subluxation.34-36 Ferlic’s 1978 publication is repeatedly cited to justify this recommendation. 21 Given that unrelenting inflammation consistently resulted in such deformities, Ferlic’s recommendation became hand surgery dogma.
In the late 1990s, a paradigm shift occurred in the treatment approach to patients with RA. Initially, DMARDs were used as monotherapy, undertreating the disease and allowing the inflammation to settle in and smolder. 37 Regression is now achievable with aggressive, multimodal DMARD therapy early in the disease process. Currently available biologic DMARDs include tumor necrosis factor α (TNFα) inhibitors, anti-TNF antibodies, anti-interleukin 1 (IL-1) antibodies, and IL-1 receptor antagonists. As therapeutic strategies have improved, few patients progress to advanced disease and severe joint deformity, whereas most achieve sustained remission.29,37,38 This observation is supported by our data, as the majority of hand surgeons noted a greater than 50% decrease in rheumatoid hand surgical procedures over the course of their career. Many of these patients will, however, continue to develop stenosing flexor tenosynovitis given their predilection for tenosynovial thickening and the 2% to 3% incidence in the general population. 39
Despite this altered natural history of RA, many textbooks continue to issue a blanket recommendation against the release of the A1 pulley in RA patients due to the increased risk of ulnar drift and MCP subluxation.12,32 Other textbooks indirectly discourage release of A1 pulley in these patients without providing specific reasons for avoiding it.30,31 Our survey confirms that most hand surgeons were trained to avoid surgical release of the A1 pulley. The current practice, however, of most surgeons is to release the A1 pulley if an RA patient presents without preexisting sequelae of chronic, progressive inflammation.
Surgeons with more experience were more likely to have been trained not to release the A1 pulley but were also more likely to have changed their practice over the course of their career. Additionally, surgeons who have practiced for fewer years were less likely to have observed ulnar deviation or MCP subluxation attributable to A1 pulley release. It is difficult, however, based on our data, to clearly delineate how much of this is due to a decrease in these deformities over time secondary to medical therapy advancements or a reflection of these surgeons’ less extensive experience with RA deformities of the hand. The 16% response rate may be viewed as a limitation of our study. It is, however, consistent with recent literature, given the well-documented phenomenon of “survey fatigue.” 40 The authors noted a trend for declining response rates specifically in published ASSH survey studies over the past 17 years.
In conclusion, indications and contraindications for A1 pulley release in RA patients are evolving along with the improved natural history of this disease associated with medical therapy advancement. The literature should also be evolving to reflect these new therapeutic advances and current hand surgery practice. The surgeons’ responses reported here indicate that standard of care for these patients has developed as a more nuanced algorithm. This assertion has potential medicolegal implications as it supports A1 pulley release in appropriately selected RA patients. This study may provide surgeons with guidance in making evidence-based decisions regarding the surgical management of stenosing tenosynovitis in patients with inflammatory arthritis based on disease severity and intraoperative findings.
Footnotes
Author’s Note
This was presented at the American Society of Plastic Surgeons 88th Annual Meeting, San Diego, CA, 2019 September 20 to 23, 2019 and the Robert H. Ivy Society 65th Annual Meeting, Pittsburgh, PA, April 13, 2019.
Ethical Approval
This study was approved by our institutional review board as well as the research division of the ASSH.
Statement of Human and Animal Rights
All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinski Declaration of 1975, as revised in 2008 (5).
Statement of Informed Consent
Informed consent was not required for this survey.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: AP reports a research internal grant from our institution, internal grant # 51, 2017, The remaining primary authors have no conflict of interest to disclose.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by our institution, internal grant # 51, 2017.