
Abstract
Background:
Assessment of outcomes for cubital tunnel syndrome (CuTS) surgeries has been difficult due to heterogeneity in outcome reporting. Our objective was to evaluate the outcomes for 2 cohorts treated surgically for isolated CuTS and for combined CuTS and carpal tunnel syndrome (CTS) using Patient Reported Outcomes Measurement Information System (PROMIS).
Methods:
There were 29 patients in the isolated CuTS cohort and 30 patients in the combined CuTS and CTS cohort. PROMIS Physical Function (PF), Pain Interference (PI), Depression, and Upper Extremity (UE) were completed preoperatively and 1-week, 6-weeks, and 3-months postoperatively. Responsiveness was evaluated by standardized response means (SRM).
Results:
Significant improvements from the 1-week to 6-week postoperative period are shown in the isolated CuTS cohort for PROMIS PF (P = .002), PI (P = .0002), and UE (P = .02), but scores plateau after 6-weeks postoperatively. A similar pattern for the same time points was seen for the combined CuTS and CTS group for PROMIS PF (P = .001), PI (P = .02), and UE (P = .04), with a plateau of scores beyond 6 weeks postoperatively. PROMIS UE was more responsive (SRM range: 0.11-1.03) than the PF (SRM range: 0.02-0.52) and PI (SRM range: 0.11-0.40), which were both mildly responsive for both cohorts.
Conclusions:
PROMIS lacks the sensitivity to show improvement beyond 6-weeks postoperatively for both isolated CuTS and combined CuTS and CTS. Patients with combined nerve compressions follow similar trajectories in the postoperative period as those with isolated CuTS.
Level of Evidence:
Level IV.
Keywords
Introduction
Cubital tunnel syndrome (CuTS) is the second most common compressive neuropathy of the upper extremity (UE) with an estimated 75000 new cases reported every year.1-3 This is second to carpal tunnel syndrome (CTS) with an estimated incidence of 3% to 5% in the general population.4-6 Of the patients who develop CuTS, approximately 40% are ultimately treated surgically. 3 Assessment of outcomes after surgical treatment of CuTS has been difficult due to the differences in outcome reporting across published studies. 7 Previous systematic reviews of CuTS have concluded there is marked heterogeneity in the outcomes evaluation of patients undergoing surgery for CuTS, and standardized assessment through a disease-specific outcome measure would provide improvement.7,8 At this point in time, there is not a preferred instrument to assess surgical outcomes after cubital tunnel surgery.
Patient reported outcome measures (PROMs) are increasingly being incorporated into routine clinical care. 9 They are being adopted into electronic medical records to track outcomes and are being used as a measure of patient status, function, and disability.4,10 Health care payers, in addition, are now considering outcome data when evaluating cost-effectiveness and determining reimbursement rates.11,12 In an attempt to provide a unified and complete health outcome system, the National Institutes of Health (NIH) created the Patient Reported Outcomes Measurement Information System (PROMIS) based on the biopsychosocial model, including instruments to measure physical, mental, and social health.9,13,14 These instruments are intended to limit floor and ceiling effects of traditional PROMs and when administered as a computer adaptive test (CAT), decrease responder burden.10,11,15 PROMIS scores are designed to have scores standardized to a mean of 50 with a standard deviation of 10 in a normative population. 5
The primary purpose of this study was to evaluate the trajectory of recovery following surgical treatment for isolated CuTS and combined CTS and CuTS, based on PROMIS PF, PI, Depression, and UE scores. Our secondary purpose was to compare the outcomes for our patient cohorts. Our null hypothesis is there would not be a significant improvement in the PROMIS domains throughout the early recovery period in either cohort or a difference in recovery between cohorts.
Methods
This study was approved by our institutional review board (IRB), and a waiver of consent was granted by our IRB, as this was a retrospective evaluation of a prospectively collected database. PROMIS PF (v1.2/v2.0), which have been shown to be comparable across versions, PI (v1.1), Depression (v1.0), and UE (v2.0) instruments using CAT were collected at routine clinic visits between January 1, 2016 to October 31, 2019 on computer tablets (Apple iPads). Patients who were included in the study had been diagnosed with CuTS based on history, physical examination, and/or electrophysiologic studies and neuromuscular ultrasound. Additional inclusion criteria were patients aged 18 years or older with elective surgical treatment for isolated CuTS or for combined CuTS and CTS. Exclusion criteria for the study included patients who were under 18 years old, those who did not complete PROMIS questionnaires, or those with inadequate follow-up, defined as a lack of a clinic visit at least 6 weeks after surgical intervention. Additional exclusion criteria included major concurrent procedures such as those for elbow trauma or arthroplasty.
We identified 73 patients who met the inclusion criteria with clinic visits within the defined study visit windows: preoperative (within -45 days), 1-week postoperative (+/-1 week), 6-week postoperative (+/-2 weeks), and 3-month postoperative (+/-4 weeks). From this pool of 73 patients, 29 patients were identified as being surgically treated for isolated CuTS, and 30 patients had been treated for combined CuTS and CTS. Three patients had surgical treatment for combined CuTS and CTS bilaterally. Surgical treatment was performed by 9 orthopedic or hand surgeons. In the combined CuTS and CTS group, there were 30 cubital tunnel releases in situ/nerve decompression, 2 anterior transpositions, and 1 submuscular transposition. Meanwhile, in the isolated CuTS group, there were as follows: 15 cubital tunnel releases in situ/nerve decompression, 10 anterior transpositions, 2 subcutaneous transpositions, 1 submuscular transposition, and 1 medial epicondylectomy. Patients included in the combined CuTS and CTS group underwent surgical treatment for CuTS as listed along with ipsilateral open (23) or endoscopic (10) carpal tunnel release (CTR) concurrently. Patients with minor additional procedures were also included in this study. Within the combined CuTS and CTS group, there were 7 patients with minor procedures including: decompression of the ulnar nerve at the level of the wrist, injection of the A-1 pulley, excision of a subcutaneous mass, A-1 pulley release, Guyon canal release, and palmar fasciectomy and excision of a palmar cord. In the isolated CuTS cohort, there were 5 patients with minor additional procedures including: excision of a ganglion cyst, lipoma excision, medial epicondylar debridement, and trigger finger release.
Statistical Analysis
Statistical analysis was performed with RStudio (R Foundation for Statistical Computing, Version 1.2.5042 [2009 – 2020]; Vienna, Austria) and Microsoft Excel ® (Redmond, Washington). Descriptive statistics (mean, standard deviation [SD], and frequency) were calculated for all demographic variables. The mean, SD, and standardized response mean (SRM) were calculated for every PROMIS domain evaluated at each study time point. The Cohen SRM is an effect size index used to gauge an instrument’s responsiveness, which is defined as an instrument’s sensitivity to change over time. Standardized Response Mean is the difference in the preoperative and postoperative means divided by the standard deviation of the difference.3,16 Using Cohen’s effect size definition, 0.2 to 0.49 is considered a small response, 0.5 to 0.79 is a moderate response, and 0.8 or greater is a large response. The paired t-test was used to compare PROMIS domain means of the same cohort between different time points. An unpaired t-test was used to compare age and body mass index (BMI) between both groups, and the chi squared test was used to compare gender, race, and ethnicity. Values of P < .05 were considered statistically significant.
Results
The PROMIS PF, PI, and depression had 89.7% to 100% completion across all time points, while the UE had 27.6% to 48.5% completion across all time points for both cohorts. Medical records were reviewed, and demographic data were collected for age, gender, race, ethnicity, BMI, surgical side, and hand dominance. A total of 59 patients were included in this study with 3 patients identified as having combined CuTS and CTS bilaterally. Descriptive characteristics of the isolated CuTS and the combined CuTS and CTS groups are reported in Table 1. Patients in the isolated CuTS group had an average age of 53.7 years, 65.5% were male, and 79.3% were Caucasian. Patients in the combined CuTS and CTS group had an average age of 57.4 years, 76.7% were male, and 83.3% were Caucasian. There were no statistically significant differences in the demographics of our 2 groups in terms of mean age, gender, race, ethnicity, or average BMI. Results of the PROMIS PF, PI, Depression, and UE scores are shown in Table 2 for the isolated CuTS group and Table 3 for the combined CuTS and CTS group. PROMIS scores for all domains over time are represented visually in Figures 1 to 4.
Baseline Characteristics of All Patients Undergoing Surgery for Cubital Tunnel Syndrome With and Without Concurrent Carpal Tunnel Release.
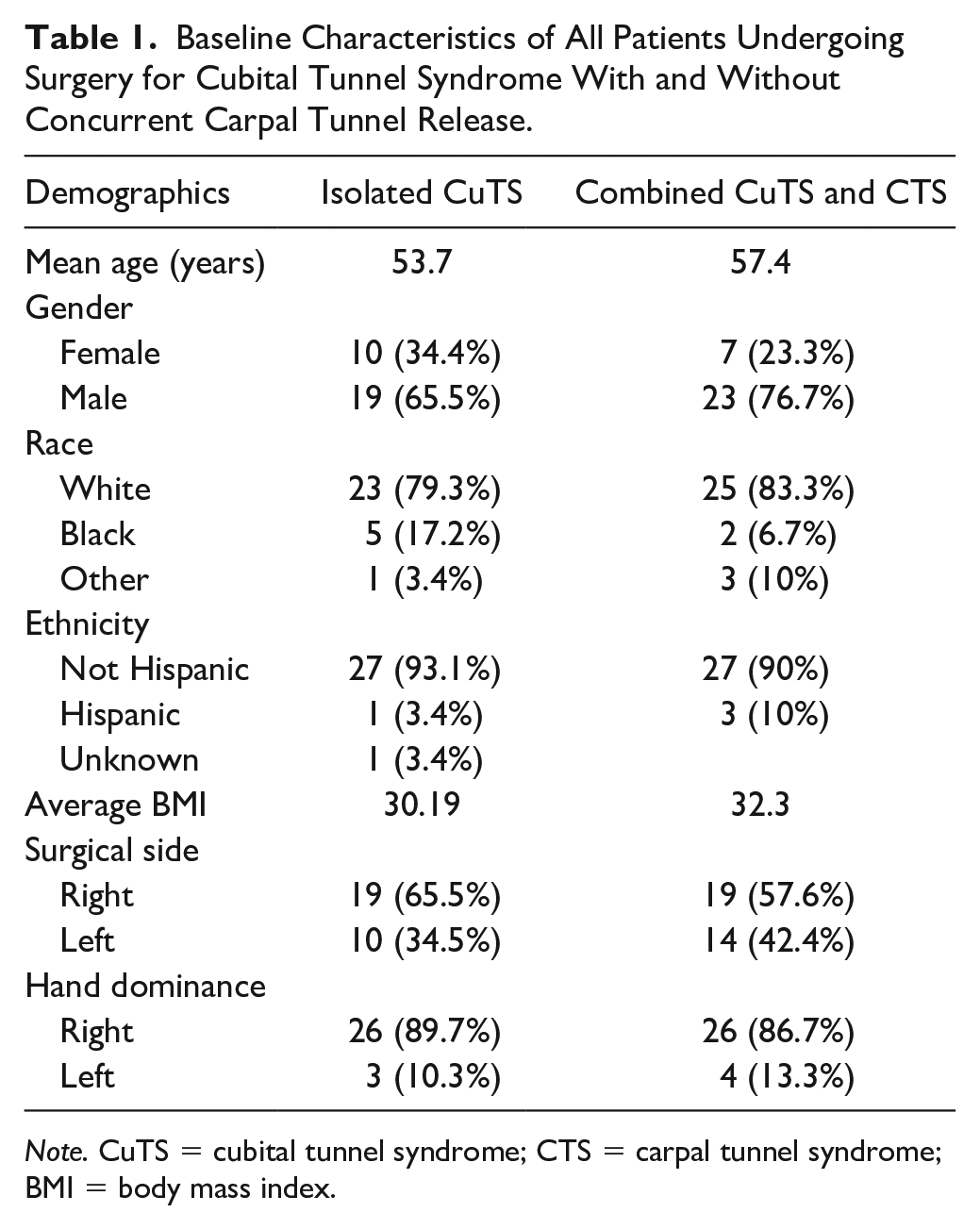
Note. CuTS = cubital tunnel syndrome; CTS = carpal tunnel syndrome; BMI = body mass index.
Results From PROMIS Physical Function, Pain Interference, Depression and Upper Extremity for Surgically Treated Patients With Isolated CuTS.
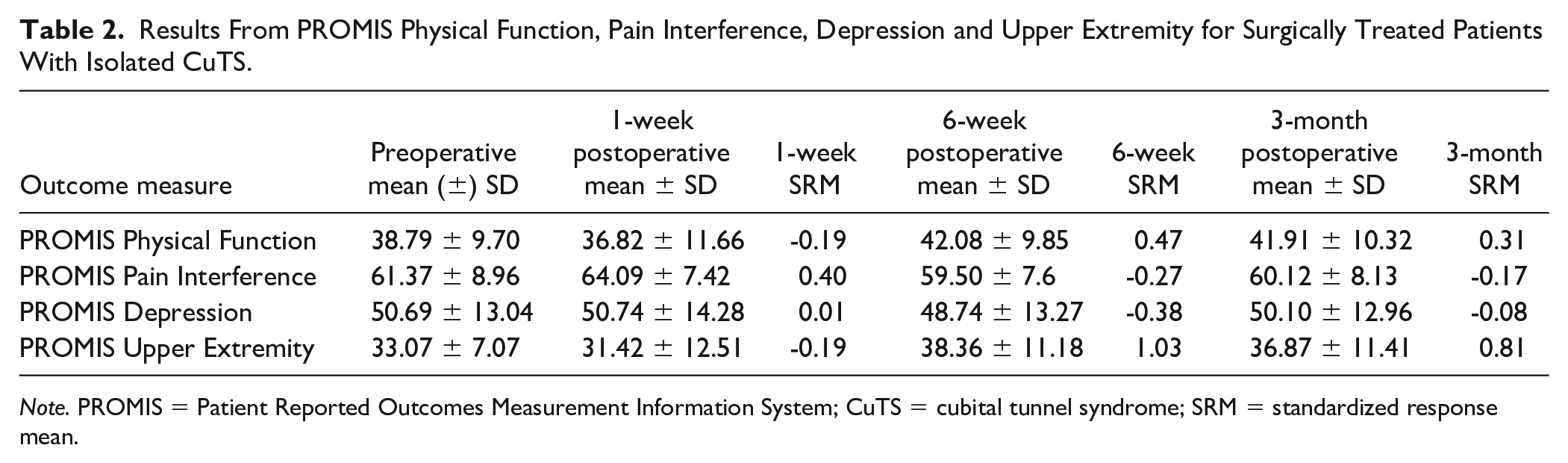
Note. PROMIS = Patient Reported Outcomes Measurement Information System; CuTS = cubital tunnel syndrome; SRM = standardized response mean.
Results From PROMIS Physical Function, Pain Interference, Depression and Upper Extremity for Surgically Treated Patients With Combined CuTS and CTS.
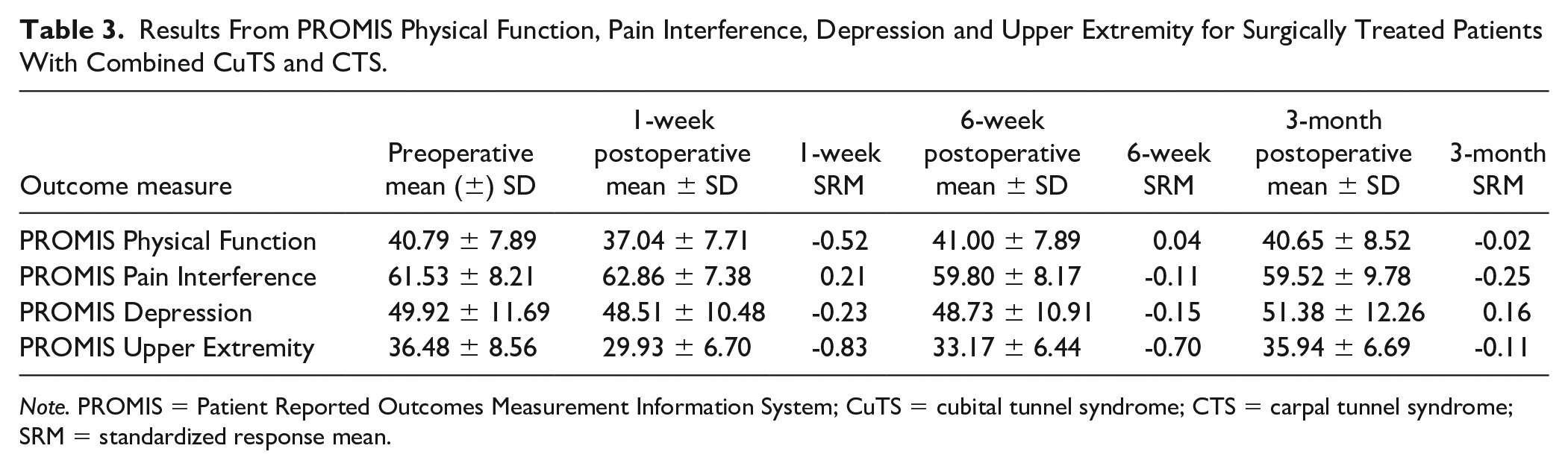
Note. PROMIS = Patient Reported Outcomes Measurement Information System; CuTS = cubital tunnel syndrome; CTS = carpal tunnel syndrome; SRM = standardized response mean.
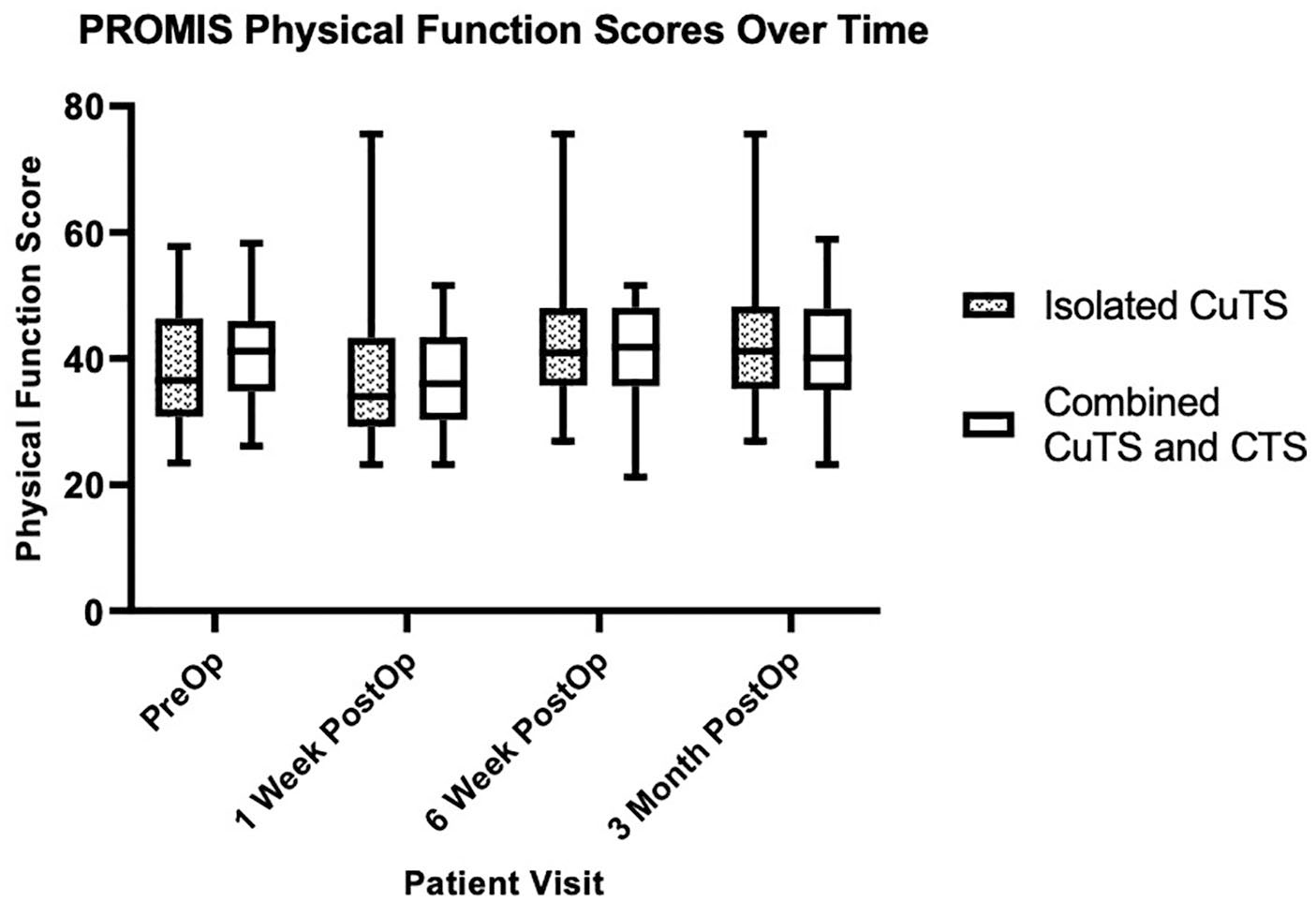
This figure illustrates the trajectory of PROMIS Physical Function outcomes for both the isolated CuTS and for the combined CuTS and CTS groups preoperatively to 3 months postoperatively.
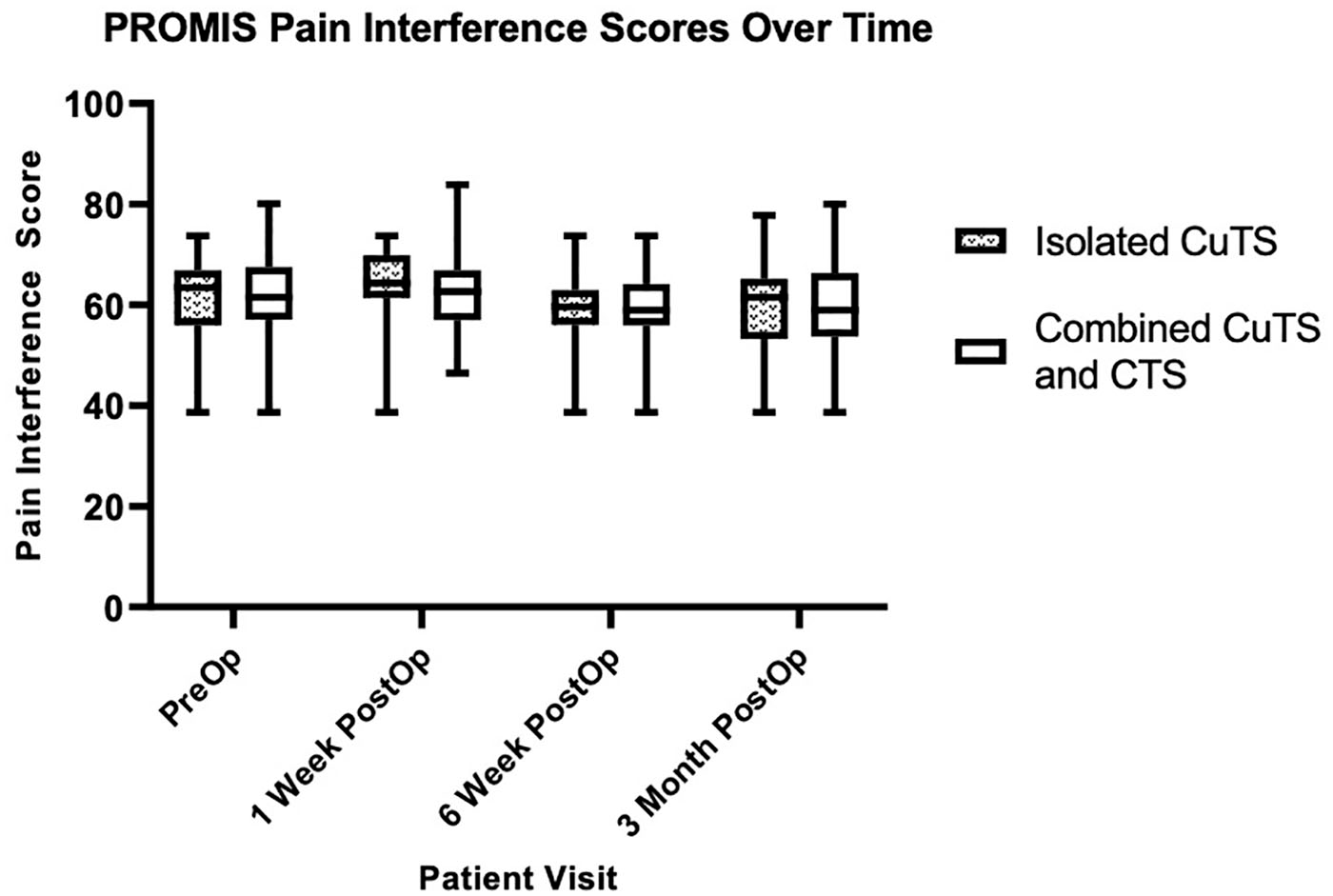
This figure illustrates the trajectory of PROMIS Pain Interference outcomes for both the isolated CuTS and for the combined CuTS and CTS groups preoperatively to 3 months postoperatively.
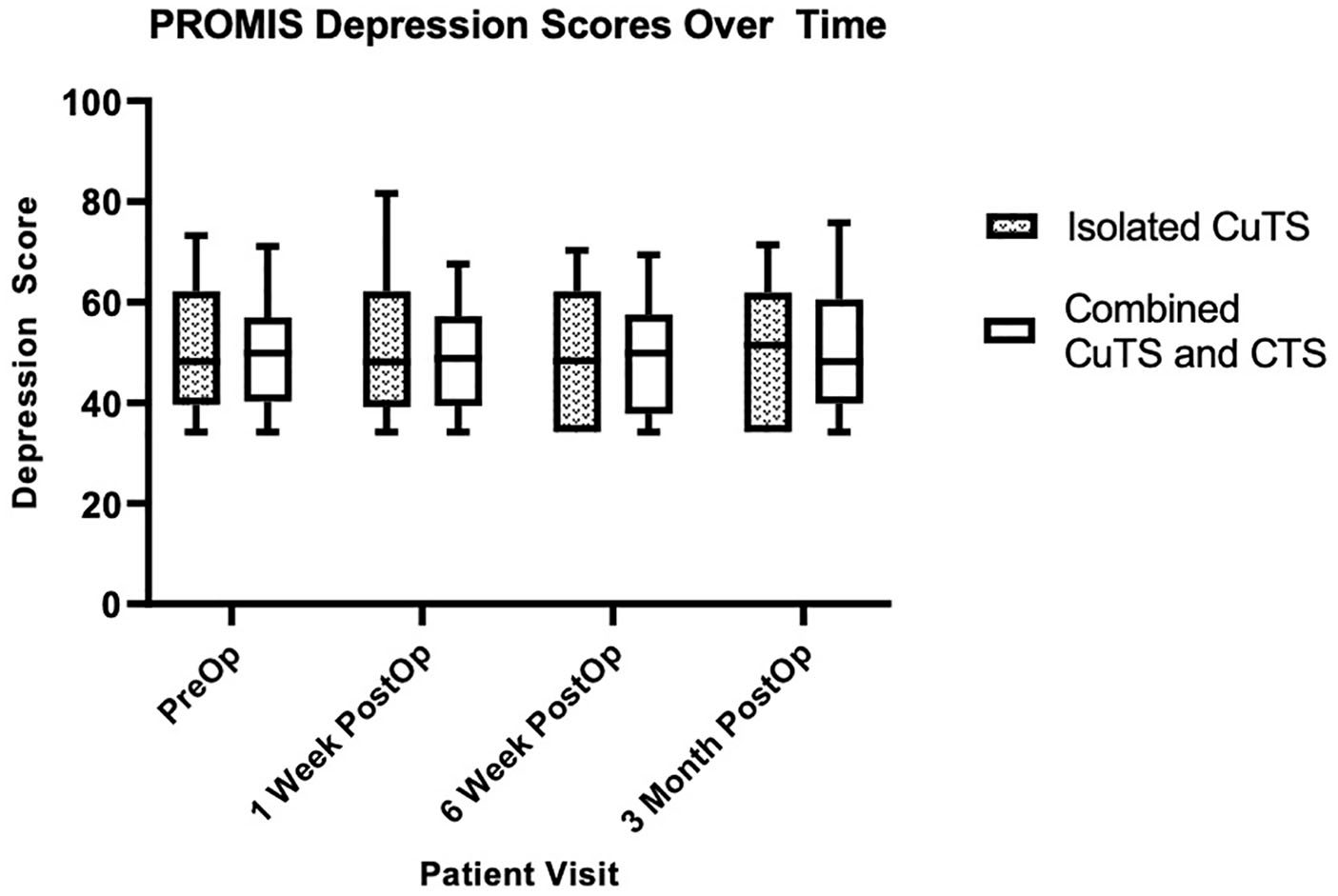
This figure illustrates the trajectory of PROMIS Depression outcomes for both the isolated CuTS and for the combined CuTS and CTS groups preoperatively to 3 months postoperatively.
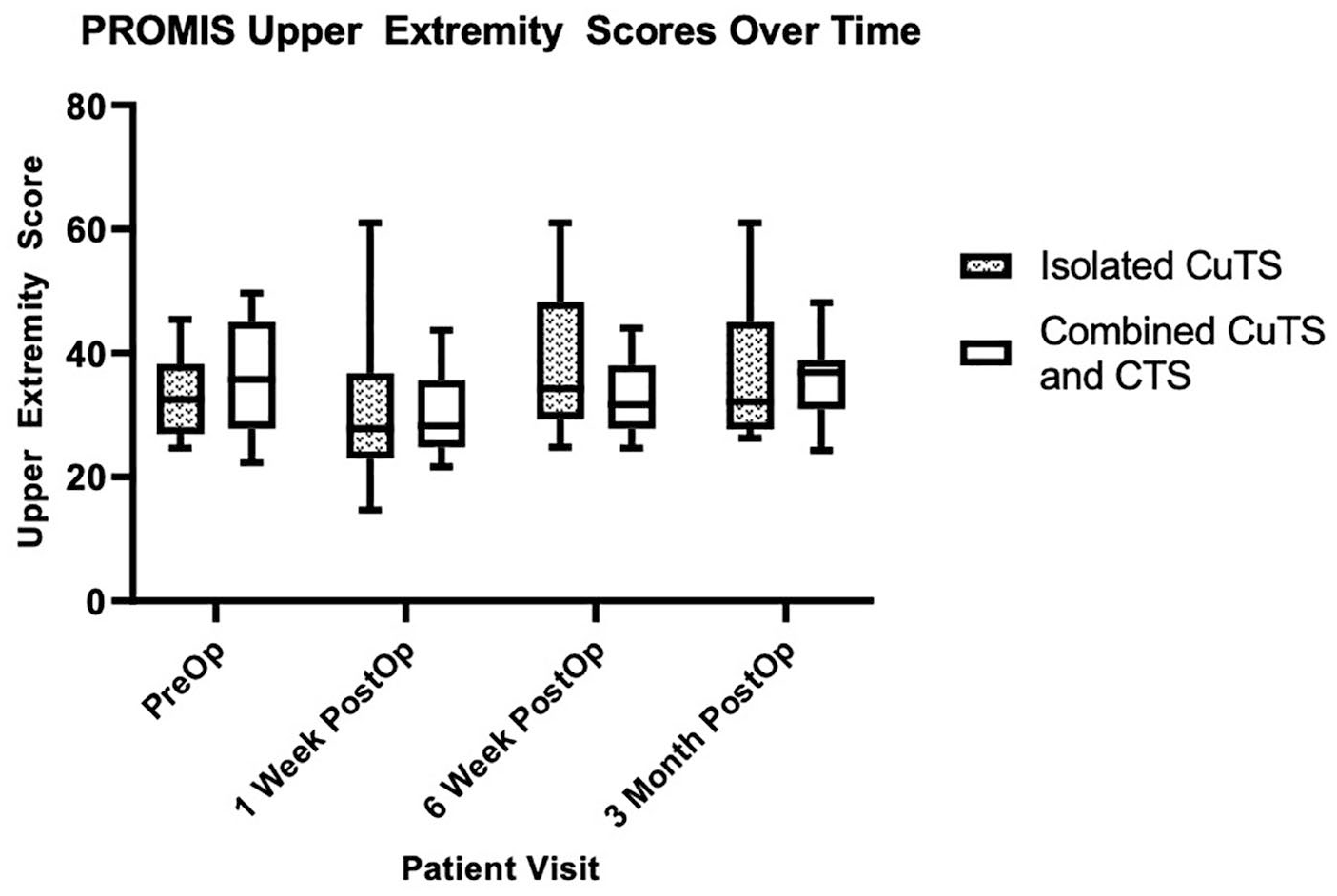
This figure illustrates the trajectory of PROMIS Upper Extremity outcomes for both the isolated CuTS and combined CuTS and CTS groups preoperatively to 3 months postoperatively.
PROMIS Outcomes for Isolated CuTS
In the isolated CuTS group, there was a significant increase in PF from 1-week to 6-weeks postoperatively (36.82 and 42.08; P = .002). From 6-weeks to 3-months postoperatively, there was a small decrease in PF that did not reach statistical significance (42.08 and 41.91, P = .91). Patients with isolated CuTS showed a significant increase in PI from the preoperative to 1-week postoperative visit (61.37-64.09; P = .04), and a significant decrease from 1-week to 6-weeks postoperatively (64.09-59.50; P = .0002). There was no significant difference in PI for this group from 6-weeks to 3-months postoperatively (59.50-60.12; P = .67). Furthermore, the isolated CuTS group showed a significant increase in the PROMIS UE from 1-week to 6-weeks postoperatively (31.42-38.36; P = .02), and a slight decrease from 6-weeks to 3-months (38.36-36.87; P = .78).
PROMIS Outcomes for Combined CuTS and CTS
For both the isolated CuTS and the combined CuTS and CTS groups, there was a significant improvement from 1-week to 6-weeks postoperatively in PF. The combined CuTS and CTS group showed a significant decrease from preoperative to 1-week postoperatively (40.79-37.04, P = .006) and a significant increase in PF from the 1-week to 6-week postoperative visits (37.04-41.00, P = .001). Similar to the isolated CuTS group, there was small decrease in PF from the 6-week to 3-month postoperative assessment (41.00-40.65; P = .85) that failed to reach statistical significance. For both cohorts, there was a significant improvement from 1- to 6-weeks postoperatively in PI similarly to that seen with PF scores. The combined CuTS and CTS group showed a significant decrease in PI from 1-week to 6-weeks postoperatively (62.86-59.80; P = .02), and minimal improvement from 6-weeks to 3-months (59.80-59.52; P = .85). The PROMIS Depression instrument showed minimal variability in both groups across all timepoints. The combined CuTS and CTS group showed a significant increase in the PROMIS UE from 1-week to 6-weeks postoperatively (29.93-33.17; P = .04), and a modest increase in UE from 6-weeks to 3-months postoperatively (33.17-35.94; P = .27). The PROMIS UE at 6 weeks postoperatively for both the isolated CuTS group and combined CuTS and CTS group showed moderate to large responsiveness (SRM = 1.03 and 0.70, respectively).
Discussion
Despite the high frequency of surgical treatment for CuTS, comparison of outcomes of cubital tunnel release remains difficult due to the heterogeneity of PROMs used.17,18 A recent systematic review of 101 studies reported that 30 different patient or clinician reported instruments were used to assess surgical treatment for CuTS within the literature. 7 Popular existing questionnaires used for hand conditions include Michigan Hand Questionnaire (MHQ); Disabilities of the Arm, Shoulder, and Hand (DASH); and the Carpal Tunnel Questionnaire (CTQ).4,19,20 The purpose of our study was to evaluate how PROMIS instruments, which were created as a unified and complete health outcome system by the NIH, performed in assessing patients after surgical intervention for isolated CuTS and comparing them to a cohort with combined CuTS and CTS. During our study, we moved from PROMIS v1.2 to v 2.0 and this has been demonstrated to be comparable across versions. Our first data point for UE was after there was a change to version 2.0. This is relevant as UE is not comparable across versions without a specific conversion available through the assessment center, which is the PROMIS repository.
Our results of the PROMIS instruments after surgery for CuTS show that for both cohorts there is anticipated worsening of PF, PI, and UE from the preoperative to 1-week postoperative assessments. This is likely attributed to postoperative surgical pain and lack of time for improvement, particularly when compared to isolated carpal tunnel release patients. The PROMIS scores improve for both groups from 1-week to 6-weeks postoperatively, likely reflecting the often rapid improvement in pain and paresthesia from surgical treatment. 2 Interestingly, the PROMIS PF, PI, and UE then essentially plateau for patients for both cohorts from their 6-week to 3-month assessments. There is no significant improvement in any of the PROMIS domains when comparing the mean preoperative score to the final mean follow up at 3 months. Explanations for our findings may be attributed to the lack of condition specific symptoms such as numbness or hand weakness in the PROMIS instruments.
Previous studies have used a multitude of PROMs when reporting outcomes and trends following cubital tunnel release. Song and colleagues from the SUN (Surgery of Ulnar Nerve) group concluded the MHQ and CTQ were more responsive than the DASH for ulnar neuropathy at the elbow. 16 This investigation demonstrated that patients following ulnar nerve decompression showed significant improvement in CTQ, DASH, and MHQ at the 1 year assessment compared to their preoperative scores. 16 Previous literature has compared the PROMs of surgery for isolated CuTS and combined CuTS and CTS. Ebersole et al demonstrated that the DASH was a valid measure of CuTS, and it is moderately responsive to change beyond 3-month follow-up. 2 Within their study, the isolated CuTS group showed improvement in the DASH up to 3 months postoperatively. 2 Meanwhile, the combined CuTS and CTS group demonstrated continued improvement up to 12 months postoperatively in the DASH and pain Visual Analogue Scale (VAS). 2
The timing of recovery after simple decompression for ulnar neuropathy at the elbow has been previously investigated. Using the MHQ, CTQ, and DASH, Giladi et al highlighted significant patient-reported symptomatic and functional recovery in the first 6 weeks postoperatively and a plateau in PROMs after 3 months. 21 The results of our study, in contrast, demonstrate that for both the isolated CuTS group and the combined CuTS and CTS group, the PROMIS instruments plateau around the 6-week postoperative period. In addition, for both groups, these instruments failed to capture significant improvement at the latest follow up of 3 months compared to baseline. This trajectory suggests that the PROMIS instruments are able to detect improvement up to 6 weeks postoperatively, but may not be sensitive enough to detect continued improvement past 6 weeks. These conclusions are reiterated when examining the SRMs of the PROMIS instruments, which were overall minimal. The PROMIS UE of this study shows higher SRMs (range: 0.11-1.03) compared to other PROMIS domains for both cohorts, but the lower completion rate for the UE should also be considered. These results are in comparison to the moderate to strong responsiveness of the CTQ, MHQ, and DASH reported within the literature. 16 We anticipated patients with combined carpal and cubital tunnel might have earlier and greater subjective improvement due to resolution of nighttime awakening, which is typical following carpal tunnel release, but did not find a difference when comparing those with isolated CTS to those with combined carpal and CTS. This may be due to none of the studied PROMIS domains being sensitive enough to detect sleep disturbances and PROMIS sleep disturbance domain may be a suitable alternative.
Our study has several limitations. This study is retrospective in nature, and outcomes measurements for each PROMIS domain were available for most, but not at every postoperative time point. We have evaluated the subjective outcomes as measured by PROMIS, but not compared to other outcome instruments or to objective measurements such as grip strength or 2-point discrimination. In addition, there is variability in severity of nerve compressions and clinical symptoms do not always correlate with severity based on electrodiagnostic studies. Our study also includes a limited sample size for each cohort. It should also be considered that patients with sufficient symptom severity might be more likely to return for their postoperative visits. Therefore, these cohorts of patients may represent a slight selection bias of those with more severe or persistent symptoms. This may be one explanation for the plateaued or marginally worse scores for PF, PI, and UE after 6 weeks postoperatively. For ulnar neuropathy at the elbow, patients were treated surgically with cubital tunnel release or simple decompression, anterior transposition, or medial epicondylectomy; all surgeries were performed by 9 orthopedic or hand surgeons. These may be factors that led to different surgical outcomes but reflect the reality of a department’s experience and treatment of CuTS. In addition, previous literature has not demonstrated a surgical technique for CuTS surgery with universal superiority above all others. 22 For the purposes of this study, we focused our goals to temporal comparisons of scores from the different PROMIS domains. Furthermore, our study reports results through the early postoperative period (3 months), while previous studies have reported sustained improvement after surgery for CuTS at the 6-month and 12-month follow-up.2,3,16 Finally, we had fewer UE data points as we began collecting this data later and was initially not uniformly used among those treating patients with ulnar neuropathy.
Conclusion
PROMs are essential to assess effectiveness and disability after surgical treatment of the upper extremity and are important endpoints to explore. Recent reviews continue to emphasize the lack of a common standard in PROMs to assess surgical outcomes for CuTS, but it would be prudent to investigate existing questionnaires before developing a standardized set of core outcomes. 7 Our study highlights that the PROMIS instruments are able to capture improvement in the immediate postoperative period to 6 weeks, but fails to show significant improvement beyond 6-weeks, nor do they demonstrate improvement from our latest follow-up at 3 months compared to baseline. PROMIS instruments demonstrate that patients with combined nerve compressions have similar recovery patterns to those with isolated CuTS after surgical treatment. This allowed partial acceptance of our null hypothesis as there was significant early postoperative improvement in both cohorts, but there was not a difference between cohorts.
Footnotes
Ethical Approval
This study was approved by our institutional review board.
Statement of Human Rights
All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2008 (5).
Statement of Informed Consent
A waiver of consent was granted for this study by the University of Rochester’s Institutional Review Board (IRB) as it was of minimal risk to patients. IRB Approval Number: 00004499.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.