
Abstract
Background:
Although ulnar nerve cross-sectional area (CSA) can be used to diagnose cubital tunnel syndrome, the predictive value of preoperative CSA for postoperative outcomes remains uncertain. This study’s primary aim was to assess the relationship between preoperative ulnar nerve CSA and postoperative changes in Patient-Reported Outcomes Measurement Information System (PROMIS) scores in the early postoperative period.
Methods:
A retrospective review was conducted of all cubital tunnel surgeries performed by the senior authors from January 2015 to May 2023. Demographics, preoperative study results, and PROMIS scores were obtained from patient charts. Bivariate and multivariable statistical testing was used to determine statistical significance. After a threshold effect of CSA was observed at 12 weeks post-operation, a Youden analysis was performed to determine the threshold value.
Results:
At 12 weeks post-operation, patients with preoperative CSA > 16 mm2 had an average change in PROMIS physical function (PF) score of −0.95, which was significantly lower than the 3.41-point improvement experienced by patients with a CSA ≤ 16 mm2. Preoperative CSA and postoperative PROMIS scores did not demonstrate a significant linear relationship, either before or after accounting for advanced patient age and type II diabetes mellitus diagnosis.
Conclusions:
A preoperative ulnar nerve CSA > 16 mm2 was predictive of significantly less improvement in PF at 12 weeks post-operation compared to the progress experienced by patients with smaller ulnar nerve CSA. These findings may aid in preoperative counseling regarding expectations for improvement in hand function during the early postoperative period.
Keywords
Introduction
Entrapment neuropathies are defined by peripheral nerve compression, leading to pain, inflammation, and loss of function of the affected nerve. Like other entrapment neuropathies, cubital tunnel syndrome (CuTS) is characterized by both mechanical and inflammatory-mediated nerve degeneration. 1 This prolonged inflammation eventually results in fibrosis and thickening of the perineurium and external epineurium. 2 Owing to this fibrous tissue growth and inflammatory-mediated edema, the cross-sectional area (CSA) of the affected nerve increases. 3 Numerous studies have demonstrated the utility of the CSA of the ulnar nerve in diagnosing CuTS.4-7 Nerve CSA is measured using gray scale ultrasound (US), which holds significant appeal as a diagnostic tool for peripheral nerve compression 8 due to its cost-effectiveness and noninvasiveness. 9
In contrast to its role in aiding diagnosis, the utility of the CSA as a prognostic indicator is less clear and varies based on the outcome measured. Beekman et al demonstrated that an increased preoperative ulnar nerve diameter corresponded to a higher likelihood of refractory symptoms at 14 months post-operation. 10 However, Duetzmann et al found no correlation between preoperative ulnar nerve CSA or change in CSA and change in Bishop scores at 46 months post-operation. 11 Lucchina et al 12 and Limbekar et al 13 reported a lack of association between postoperative change in ulnar nerve CSA and Quick Disabilities of the Arm, Shoulder, and Hand (QuickDASH scores) 12 or American Shoulder and Elbow Surgeons—Elbow questionnaire scores, 13 respectively. Thus, there is no consensus on the utility of preoperative CSA in predicting postoperative outcomes.
This relationship remains particularly unclear in the early postoperative period, as the correlation between preoperative ulnar nerve CSA and postoperative outcomes has not yet been evaluated at a time point as early as 3 months post-operation. Although not studied in relation to CSA, postoperative improvements in both patient-reported outcomes and objective measurements of hand function such as grip strength and motor conduction velocity have been shown to occur within this time frame.14,15 In addition, preoperative median nerve CSA has been shown to correlate with improvement in Boston Carpal Tunnel Questionnaire (BCTQ) scores at 3 months following carpal tunnel release. 16
This study aimed to assess the relationship between preoperative ulnar nerve CSA and postoperative changes in Patient-Reported Outcomes Measurement Information System (PROMIS) scores in the early postoperative period. We hypothesized that improvement in PROMIS scores at 6- and 12-weeks post-operation would demonstrate an inverse correlation with preoperative CSA.
Methods
Data Collection
After determination of exemption from our institutional review board, this retrospective study examined all cubital tunnel surgeries completed by the senior authors from January 2015 to May 2023. All adult patients who underwent surgery for CuTS, had an ulnar nerve US before cubital tunnel surgery, and completed PROMIS questionnaires both preoperatively and postoperatively were included. Exclusion criteria included patients with incomplete PROMIS questionnaires, as well as those who experienced a postoperative complication. For the purpose of this study, we defined a postoperative complication as an infection of the surgical site or a revision surgery within 6 months of the original surgery. Demographic data, type of surgery (i.e., decompression, transposition), and medical comorbidities (i.e., diabetes, pain syndrome diagnoses, and long-term opioid use) as well as nerve conduction velocity (NCV), electromyography (EMG), and US data were obtained from the medical record. Nerve USs and CSA measurements were performed by experienced Physical Medicine and Rehabilitation physicians. Per our standard practice, PROMIS anxiety, upper extremity (UE), depression, physical function (PF), and pain interference (PI) questionnaires were completed by all patients preoperatively and at their scheduled postoperative visits. These data were retrieved from our institutional Research Electronic Data Capture (REDCap) database. Postoperative PROMIS scores were recorded within the first 6 weeks following surgery and again between 6- and 12-weeks post-operation.
Statistical Analysis
Differences in means between groups were analyzed using 2-sample t-tests or Mann-Whitney U tests. Paired t-tests were used to compare changes in PROMIS scores from preoperation to post-operation; for all other analyses, 2-sample t-tests were used.
Differences in frequencies between groups were analyzed using chi-squared tests or Fishers exact test. Correlation coefficients were determined through linear regression analysis. Prior to conducting multivariable analyses, patients were grouped according to age and type II diabetes mellitus (T2DM) diagnosis. Age and T2DM were specifically chosen due to their associations with decreased peripheral nerve regeneration ability.17,18 Age was dichotomized to allow for similar analysis to that of T2DM diagnosis. Patients were grouped based on whether they were younger than 60 or 60 and older to maintain continuity with other studies.19-22 Multivariable linear regression analysis or analysis of covariance (ANCOVA) were performed for continuous outcomes, and logistic regression analysis for binary outcomes. Interactions of interest were assessed in these models. A Youden analysis was conducted to determine the optimal CSA threshold value. All the statistical tests were 2-sided and significance was determined at P < .05.
Results
Preoperative Data
Out of the 387 patients who underwent cubital tunnel surgery by the senior authors within our specified time frame, 135 had a preoperative ulnar nerve US. Of these, 7 had incomplete or absent PROMIS questionnaires, and none had postoperative complications, resulting in a final sample size of 128 patients. Demographic data were collected on this cohort (Supplemental Table S1). Preoperative CSA demonstrated a significant linear relationship (P < .05) with each of the 14 preoperative electrophysiologic measures of nerve function that were analyzed (Table 1). These included significant correlations between preoperative CSA and compound motor action potential amplitude for the abductor digit minimi (r = −0.4, P < .01) and first dorsal interosseous (r = −0.38, P < .01) muscles.
Relationship Between Preoperative Ulnar Nerve CSA and Electrophysiologic Measures of Nerve Function Recorded Prior to Surgery.
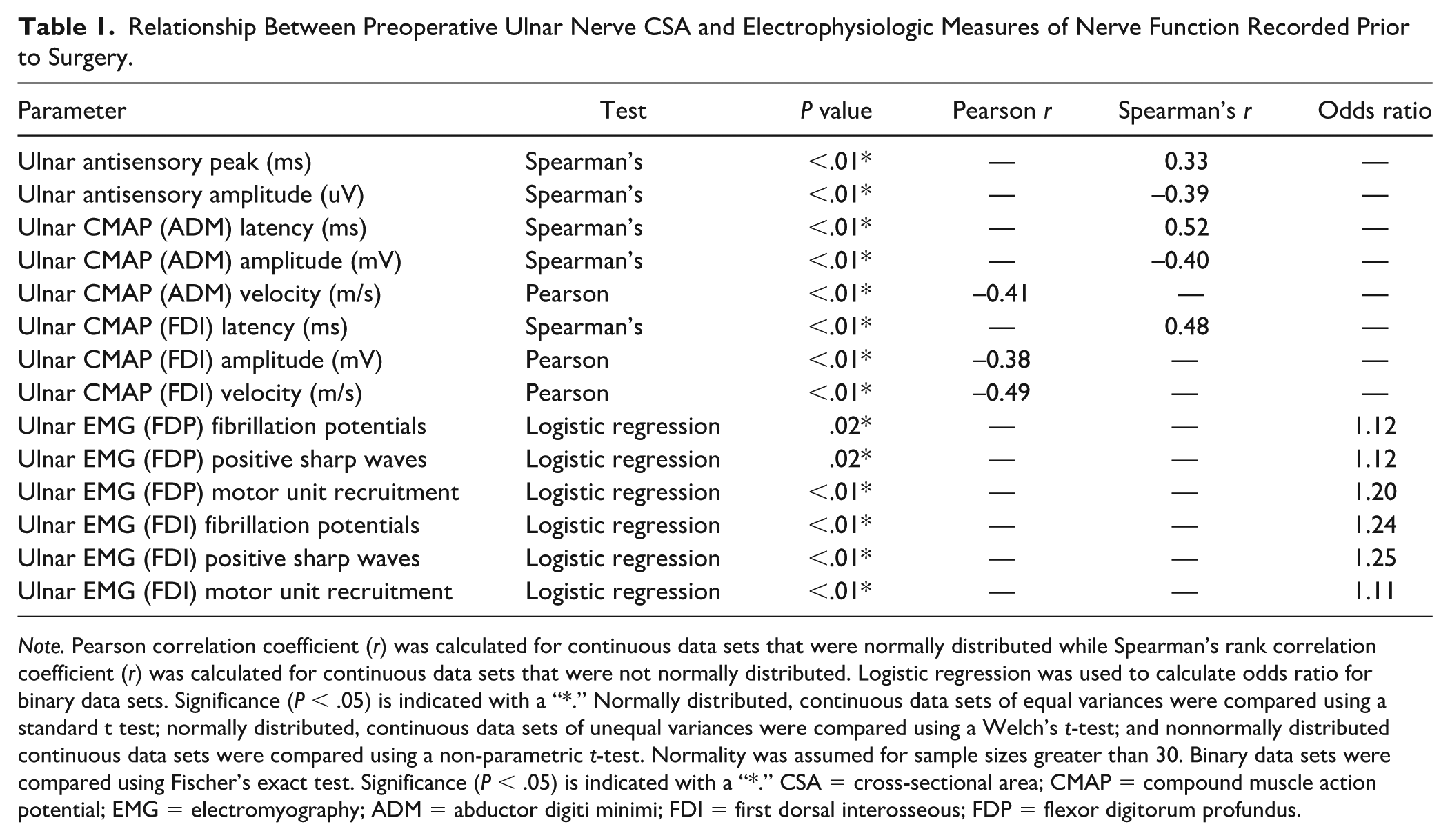
Note. Pearson correlation coefficient (r) was calculated for continuous data sets that were normally distributed while Spearman’s rank correlation coefficient (r) was calculated for continuous data sets that were not normally distributed. Logistic regression was used to calculate odds ratio for binary data sets. Significance (P < .05) is indicated with a “*.” Normally distributed, continuous data sets of equal variances were compared using a standard t test; normally distributed, continuous data sets of unequal variances were compared using a Welch’s t-test; and nonnormally distributed continuous data sets were compared using a non-parametric t-test. Normality was assumed for sample sizes greater than 30. Binary data sets were compared using Fischer’s exact test. Significance (P < .05) is indicated with a “*.” CSA = cross-sectional area; CMAP = compound muscle action potential; EMG = electromyography; ADM = abductor digiti minimi; FDI = first dorsal interosseous; FDP = flexor digitorum profundus.
Preoperative CSA exhibited a significant but highly variable relationship with patient age (r = 0.2, P < .01), indicating that while CSA and patient age are generally correlated, individual variability is substantial. Patients above 60 years of age demonstrated significantly worse electrophysiologic nerve function compared to younger patients (Table 2). Despite this, preoperative PROMIS scores were not significantly different between patients of advanced age and their younger counterparts (P = [.20-.80]). Patients with T2DM did not demonstrate significantly worse preoperative nerve function compared to patients without T2DM (P = [.06-.94]). Patients with T2DM demonstrated significantly worse preoperative PROMIS PF scores (P = .04), though all other preoperative PROMIS scores were not significantly different between groups (P = [.19-.85]).
Comparison of Preoperative Nerve Function Between Patients Younger Than 60 and Patients Aged 60 and Older.
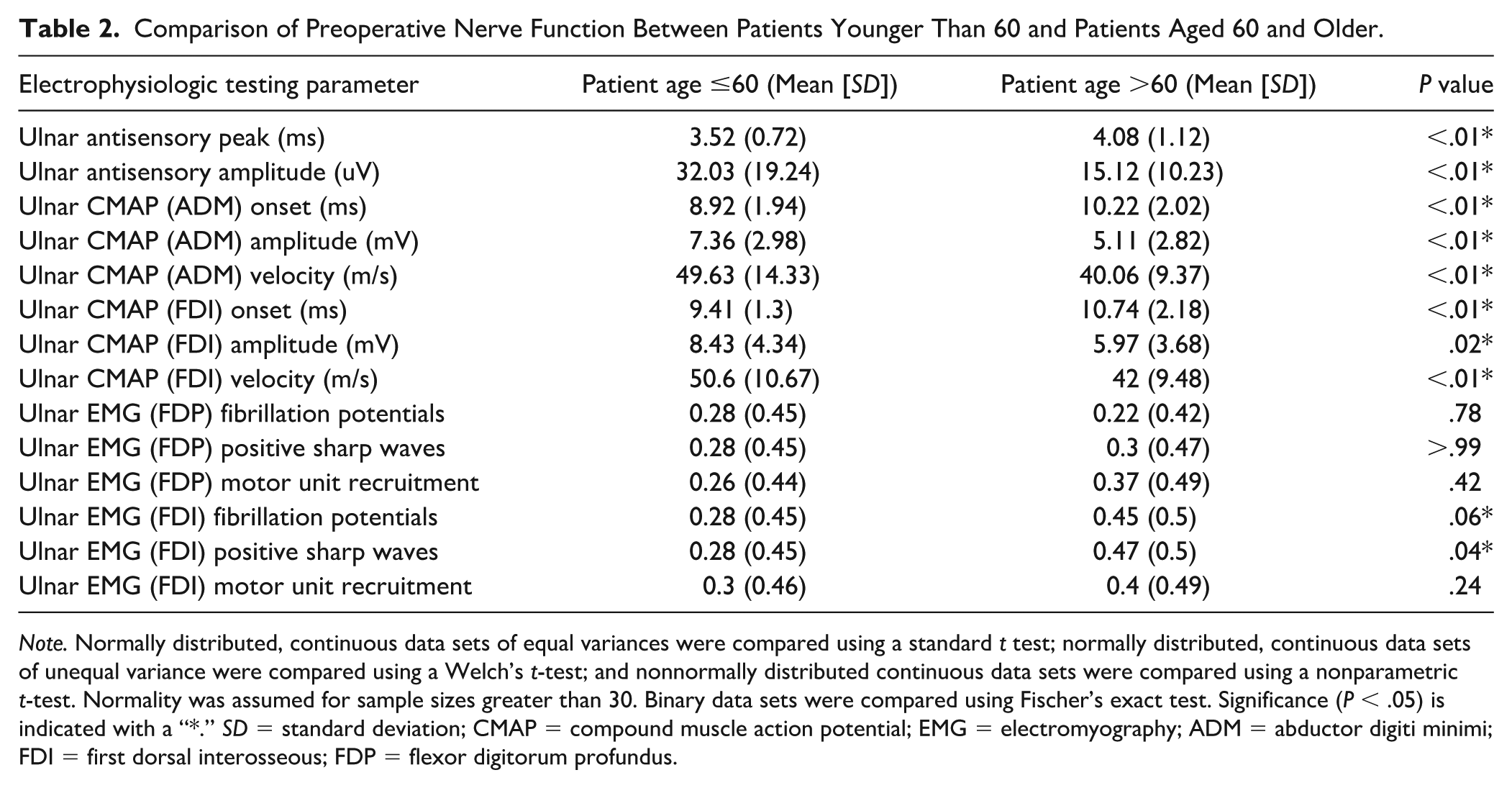
Note. Normally distributed, continuous data sets of equal variances were compared using a standard t test; normally distributed, continuous data sets of unequal variance were compared using a Welch’s t-test; and nonnormally distributed continuous data sets were compared using a nonparametric t-test. Normality was assumed for sample sizes greater than 30. Binary data sets were compared using Fischer’s exact test. Significance (P < .05) is indicated with a “*.” SD = standard deviation; CMAP = compound muscle action potential; EMG = electromyography; ADM = abductor digiti minimi; FDI = first dorsal interosseous; FDP = flexor digitorum profundus.
Postoperative Data
Within the first 6 weeks of surgery, PROMIS anxiety and PI scores improved significantly (P < .01) while PROMIS UE scores worsened significantly (P = .03) (Table 3). No significant changes in PROMIS depression and PF scores were observed at this time point. However, at 12 weeks post-operation, scores from all 5 PROMIS domains exhibited significant within-patient improvement (P < .05) (Table 4).
Comparison of PROMIS Scores From Before Cubital Tunnel Surgery to 6 Weeks Post-Operation.
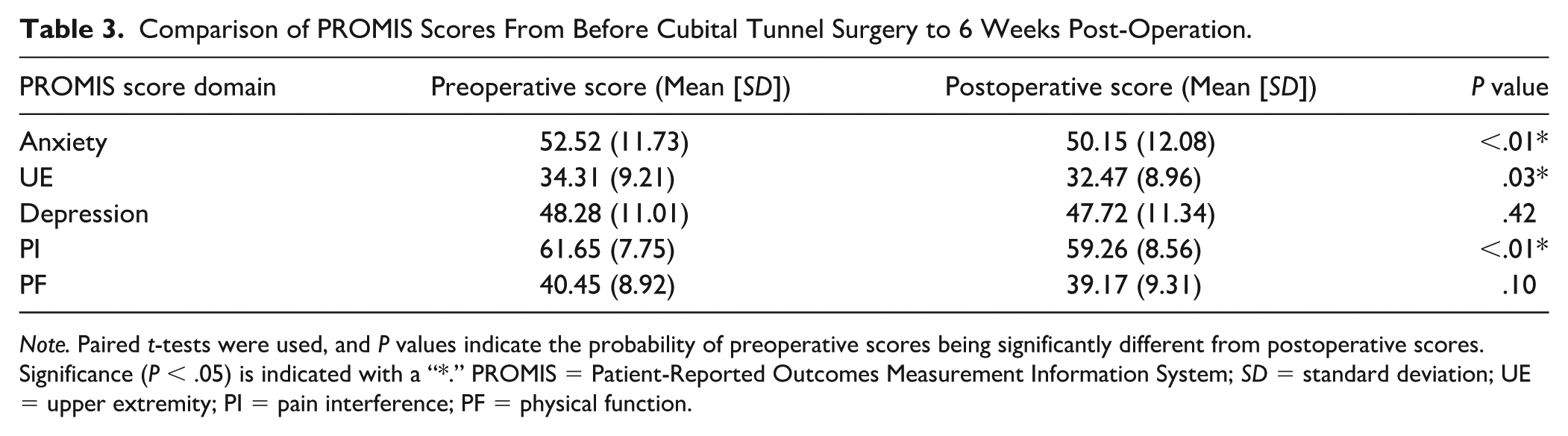
Note. Paired t-tests were used, and P values indicate the probability of preoperative scores being significantly different from postoperative scores. Significance (P < .05) is indicated with a “*.” PROMIS = Patient-Reported Outcomes Measurement Information System; SD = standard deviation; UE = upper extremity; PI = pain interference; PF = physical function.
Comparison of PROMIS Scores From Before Cubital Tunnel Surgery to 12 Weeks Post-Operation.
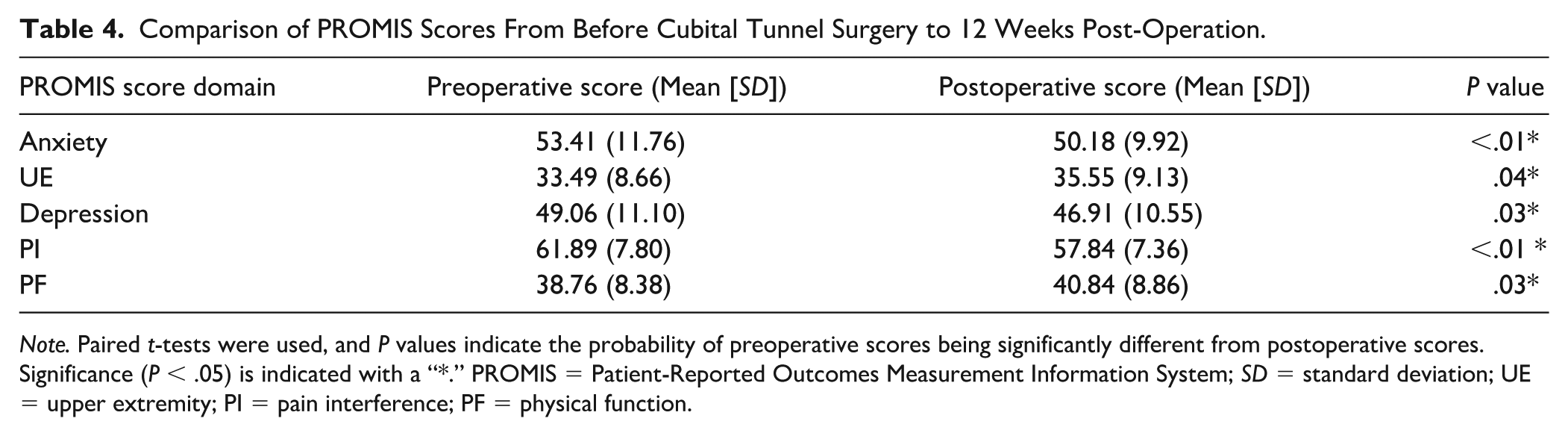
Note. Paired t-tests were used, and P values indicate the probability of preoperative scores being significantly different from postoperative scores. Significance (P < .05) is indicated with a “*.” PROMIS = Patient-Reported Outcomes Measurement Information System; SD = standard deviation; UE = upper extremity; PI = pain interference; PF = physical function.
At both 6- and 12-week post-operation, no significant differences were observed in postoperative PROMIS scores or changes in PROMIS scores between patients of advanced age and younger patients (P = [.12-.67]), or between patients with T2DM and those without T2DM (P = [.11-.90]).
At both 6- and 12-week post-operation, there were no significant linear correlations between preoperative CSA and postoperative PROMIS scores, either before or after factoring for advanced patient age (P = [.19-.96]) and T2DM diagnosis (P = [.09-.21]).
Establishing a CSA Threshold for Effect on Outcomes
While no significant correlation was noted between CSA and PROMIS scores at 12 weeks post-operation, careful analysis of our data revealed a threshold effect of CSA. To better understand this, we conducted a Youden analysis that included CSA values of 14 mm2 through 18 mm2. This analysis indicated that 16 mm2 was the optimal threshold value (P = .03). Thus, patients were subdivided into 2 groups, those with a CSA ≤16 mm2 and those with a CSA >16 mm2.
There was no statistically significant difference in age, sex, surgery type, surgery side, additional surgeries, long-term opioid use, T2DM diagnosis, pain syndrome diagnosis, or preoperative PROMIS scores between patients with a CSA ≤16 mm2 and those with a CSA > 16 mm2 (P = [.16-.99]).
Preoperatively, patients with a CSA >16 mm2 demonstrated significantly worse nerve function on 12 out of the 14 EMG/NCV parameters, including all 9 that tested the intrinsic musculature of the hand (Table 5).
P values Indicate the Probability of a Significant Difference in Preoperative Measures of Nerve Function Between Patients With an Ulnar Nerve CSA ≤16 mm2 and Patients With a CSA >16 mm2.
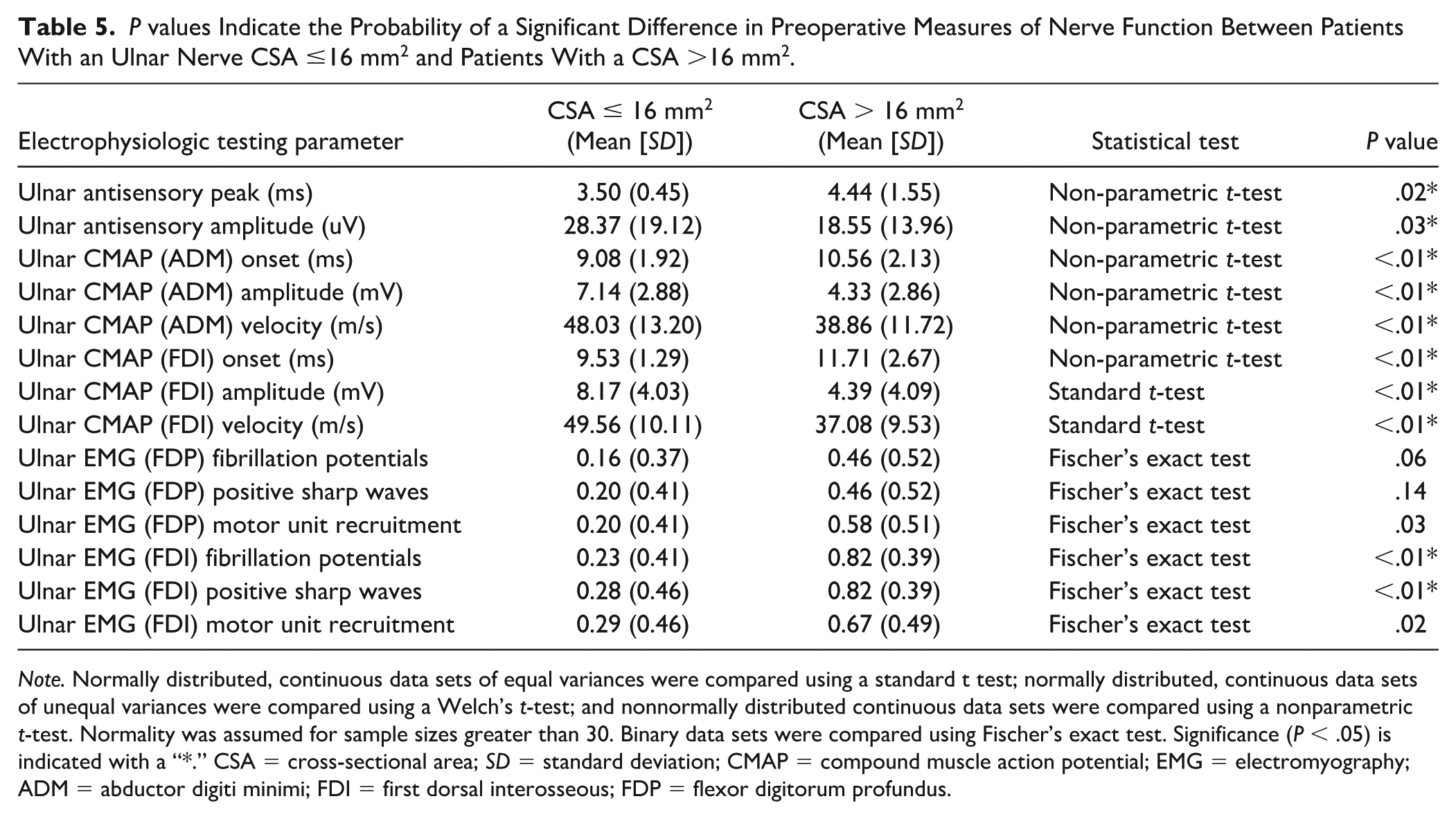
Note. Normally distributed, continuous data sets of equal variances were compared using a standard t test; normally distributed, continuous data sets of unequal variances were compared using a Welch’s t-test; and nonnormally distributed continuous data sets were compared using a nonparametric t-test. Normality was assumed for sample sizes greater than 30. Binary data sets were compared using Fischer’s exact test. Significance (P < .05) is indicated with a “*.” CSA = cross-sectional area; SD = standard deviation; CMAP = compound muscle action potential; EMG = electromyography; ADM = abductor digiti minimi; FDI = first dorsal interosseous; FDP = flexor digitorum profundus.
At 6 weeks post-operation, there was no significant difference in percent change in PROMIS scores between patients with a preoperative CSA ≤16 mm2, and patients with a preoperative ulnar nerve CSA >16 mm2 (P = [.07-.78]).
At 12 weeks post-operation, patients with a preoperative ulnar nerve CSA ≤16 mm2 had an average improvement in PROMIS PF score of 3.4 which was significantly greater than the −0.95 average improvement experienced by patients with a preoperative CSA > 16 mm2 (P = .03) (Figure 1, Supplemental Table S1). Patients with a CSA ≤16 mm2 also demonstrated significantly more improvement in anxiety compared to those with a larger CSA (P = .04). In addition, patients with a CSA ≤ 16 mm2 achieved higher postoperative UE scores compared to those with a larger CSA (P = .02) (Figure 2, Supplemental Table S2).
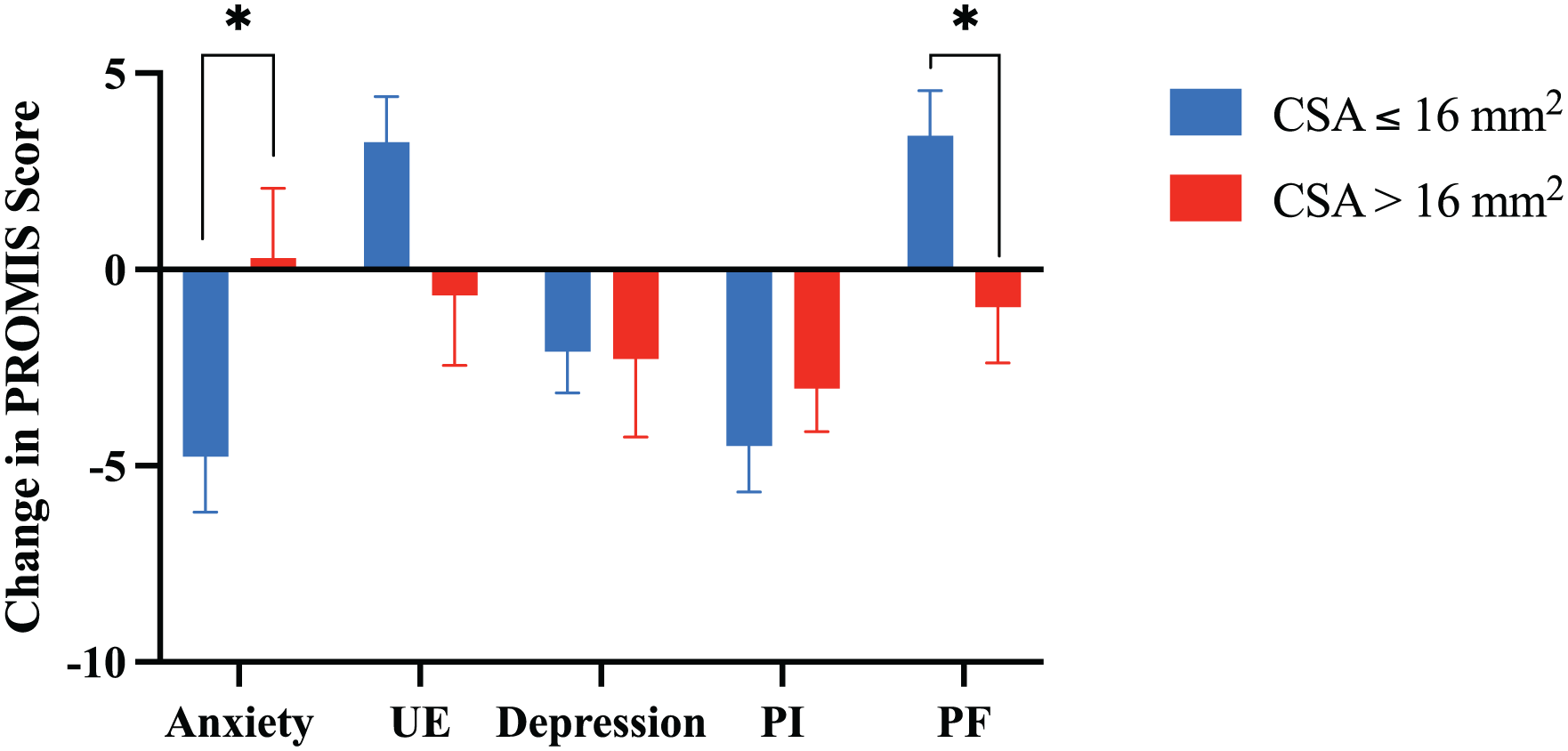
Mean ± standard error of the mean for change in PROMIS scores at 12 weeks post-operation for patients with a CSA ≤16 mm2 and those with a CSA >16 mm2. PROMIS PF and anxiety scores are significantly different between groups.
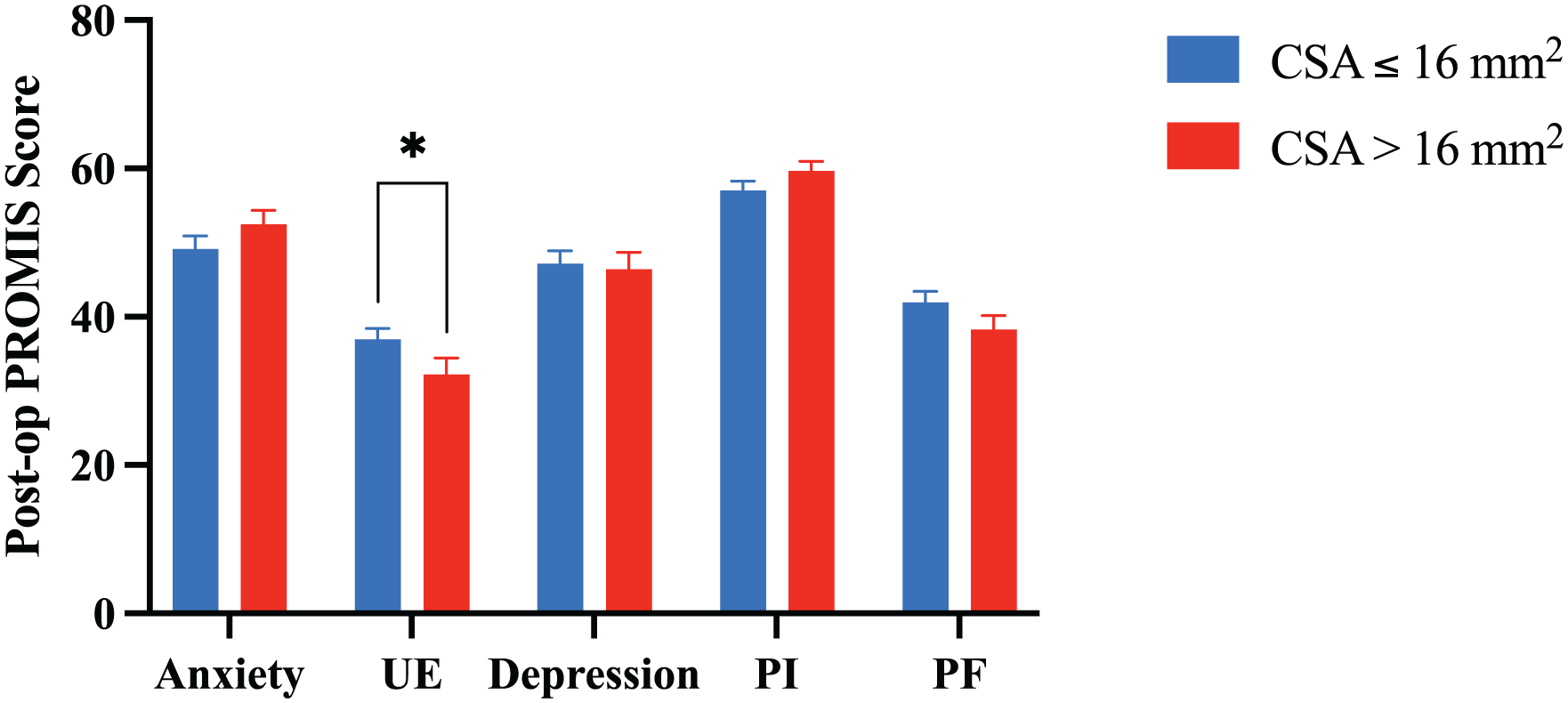
Mean ± standard error of the mean for PROMIS scores recorded at 12 weeks post-operation for patients with a CSA ≤ 16 mm2 and those with a CSA > 16 mm2. PROMIS UE scores are significantly different between the 2 groups.
At 12 weeks post-operation, there were no statistically significant differences in changes in PROMIS scores or postoperative PROMIS scores among patients who underwent transposition, decompression, or transposition revision (P = [.06-.89]), except for postoperative change in anxiety (P = .03). Patients who underwent revision transposition demonstrated a 3.81-point increase in anxiety compared to their preoperative levels, while patients who underwent primary transposition or decompression experienced a 3.97-point or 7.03-point decrease in anxiety, respectively.
Discussion
Our results demonstrate that a preoperative ulnar nerve CSA >16 mm2 predicts greater disease severity preoperatively and a higher likelihood of symptoms refractory to surgery over the first 12 postoperative weeks. Specifically, in the early postoperative period, patients with a CSA >16 mm2 demonstrated significantly less improvement in PROMIS PF and anxiety scores and significantly worse postoperative PROMIS UE scores compared to those with a CSA ≤16 mm2. As PF scores assess overall functionality, they can be influenced by numerous factors unrelated to hand function. Therefore, changes in PF scores are more likely to reflect the impact of the surgery compared to postoperative PF scores alone. However, as UE scores exclusively assess hand functionality, postoperative UE scores can offer valuable insights into the level of hand function attained by patients regardless of their initial condition. Taken together, these results suggest that a preoperative CSA >16 mm2 may indicate a decrease in both the potential for early improvement in overall function and the level of hand function achieved at 12 weeks following cubital tunnel surgery.
These results hold implications for both the diagnosis and management of patients presenting with suspected CuTS. Patients with an ulnar nerve CSA >16 mm2 are unlikely to experience improvement in PROMIS PF scores in the first 12 weeks after surgery. This is an important consideration for surgical counseling, as many patients are eager to regain hand function and return to their work and home responsibilities as soon as possible. As the 4.4 point average difference in PROMIS PF scores between patients with a CSA ≤16 mm2 and those with a CSA >16 mm2 is clinically relevant,23,24 our findings could aid in counseling patients about their expected postoperative course and setting reasonable goals. In addition, these findings could inform surgical planning by providing a less expensive and uncomfortable strategy for stratifying the severity and surgical responsiveness of CuTS compared to EMG and NCV data, perhaps even helping to inform which surgical approach or adjunct procedures may be most useful.
Despite patients with a CSA >16 mm2 exhibiting severe EMG and NCV findings, preoperative PROMIS scores were not significantly different between patients with a CSA >16 mm2 and those with a smaller CSA. Interestingly, this suggests that despite differences in initial nerve conduction studies, patients with a CSA >16 mm2 may not report more severe impairment of PF compared to those with a smaller CSA and less severe disease. This observation may be attributed to the possibility that patients with more pronounced functional impairments at an earlier stage of their disease course seek medical attention sooner, or it may suggest that patients with more severe disease implement compensatory strategies to retain functionality.
At 6 weeks post-operation, only PI and anxiety scores showed significant improvement compared to preoperation. By 12 weeks post-operation, patients demonstrated improvement in PROMIS scores across all 4 domains. The observed changes in PROMIS scores at 6 weeks post-operation may reflect pain relief associated with decompression, while changes in scores at 12 weeks could indicate true nerve recovery. One potential explanation for this finding is that patients with a smaller CSA have lower-grade neurapraxia and thus increased early recovery potential compared to those with a larger CSA. Specifically, if a smaller CSA represents less severe injury with a lower percentage of axon damage, collateral branching may be the primary mechanism of recovery, compared to more severe injuries with a larger percentage of neurons damaged, where the slower process of regeneration must occur for recovery. 25 We did not identify a CSA threshold effect on pain relief, suggesting that patients experience effective pain relief early in their postoperative course regardless of disease severity. However, a preoperative CSA threshold may be useful in predicting early nerve recovery ability, which would explain the separation in PROMIS PF scores at 12 weeks between patients with a CSA ≤16 mm2 and those with a CSA >16 mm2.
Our results also revealed that although patients older than 60 were more prone to have severe disease, as indicated by both a larger CSA and worse EMG and NCV results, their preoperative, postoperative, and changes in PROMIS scores did not show significant differences compared to younger patients. Patients with T2DM demonstrated lower preoperative PF scores compared to patients without T2DM; however, their EMG and NCV results, CSA, postoperative PROMIS scores, and changes in PROMIS scores did not exhibit significant differences. These findings may offer reassurance to older patients and patients with T2DM who are considering surgery. Despite potentially more severe disease or preoperative functional impairment, they are still likely to experience similar early postoperative improvements to their younger and nondiabetic counterparts.
Strengths of this study include the large sample size and the utilization of common and validated patient-reported outcome measures (PROMIS scores). PROMIS UE scores demonstrate high sensitivity for change in CuTS symptoms, with the MCID of 3.1 to 3.7 able to detect even a mild change in symptoms. 26 In addition, PROMIS PF and UE scores have been shown to exhibit significant, moderate to strong correlations with several other patient-reported outcome measurement systems, including the Patient-Rated Ulnar Nerve Evaluation, BCTQ, and Impact of a Hand Nerve Disorders in patients with carpal or CuTS. 27 However, our study also has several limitations. One limitation was the potential variance introduced by differences in surgery type and additional surgeries, but these factors were not significantly different between patients with a CSA ≤16 mm2 and those with a CSA >16 mm2, which suggests that any confounding effects of these variables are minimal. In addition, aside from anxiety, postoperative outcomes were not statistically different between patients who underwent transposition, decompression, or revision transposition, which suggest that the inclusion of multiple surgical techniques does not compromise the validity of our findings. Although we do note that methodologically, it would be simpler to only include primary cubital tunnel decompressions or transpositions, we felt that a more heterogeneous surgical group would better reflect standard practice. Our study is also limited by the potential impact of unaccounted-for comorbid conditions (such as obesity or other injuries) on PROMIS scores and by possible nonresponse bias due to the inclusion of only those patients who completed both preoperative and postoperative PROMIS questionnaires. Thus, while the broad demographic scope of our study increases its external validity, the generalizability of our findings may be limited for patients with comorbid conditions or barriers in returning to clinic to complete postoperative questionnaires, such as limited access to transportation, childcare, or time off work. In addition, our results offer an early assessment of postoperative recovery, which likely does not fully capture total recovery, as hand function continues to improve up to 1-year post-operation. 28
In summary, patients with an ulnar nerve CSA >16 mm2 may experience decreased recovery of in the early postoperative period compared to other patients. These findings hold significance for surgical decision making and postoperative goal setting. Future studies could explore whether a larger preoperative CSA predicts a smaller change in CSA postoperatively and whether a similar threshold exists to predict postoperative function based on preoperative CSA for carpal tunnel syndrome.
Supplemental Material
sj-docx-1-han-10.1177_15589447251374230 – Supplemental material for The Utility of Ulnar Nerve Cross-Sectional Area in Predicting Patient Outcomes in the Early Postoperative Period
Supplemental material, sj-docx-1-han-10.1177_15589447251374230 for The Utility of Ulnar Nerve Cross-Sectional Area in Predicting Patient Outcomes in the Early Postoperative Period by Gabrielle K. Marushack, Christopher J. Dy, Ryan Calfee, Ling Chen and David M. Brogan in HAND
Supplemental Material
sj-docx-2-han-10.1177_15589447251374230 – Supplemental material for The Utility of Ulnar Nerve Cross-Sectional Area in Predicting Patient Outcomes in the Early Postoperative Period
Supplemental material, sj-docx-2-han-10.1177_15589447251374230 for The Utility of Ulnar Nerve Cross-Sectional Area in Predicting Patient Outcomes in the Early Postoperative Period by Gabrielle K. Marushack, Christopher J. Dy, Ryan Calfee, Ling Chen and David M. Brogan in HAND
Supplemental Material
sj-docx-3-han-10.1177_15589447251374230 – Supplemental material for The Utility of Ulnar Nerve Cross-Sectional Area in Predicting Patient Outcomes in the Early Postoperative Period
Supplemental material, sj-docx-3-han-10.1177_15589447251374230 for The Utility of Ulnar Nerve Cross-Sectional Area in Predicting Patient Outcomes in the Early Postoperative Period by Gabrielle K. Marushack, Christopher J. Dy, Ryan Calfee, Ling Chen and David M. Brogan in HAND
Footnotes
Ethical Approval
This study received ethical approval from the Washington University School of Medicine IRB (approval #202308080) on 8/5/2023.
Statement of Human and Animal Rights
The study was conducted in accordance with the Declaration of Helsinki and was approved by the IRB of Washington University School of Medicine, with the need for written informed consent waived.
Statement of Informed Consent
This study is a retrospective analysis conducted using existing medical records. The research has been reviewed and approved by the Washington University School of Medicine IRB and a waiver of informed consent has been granted.
Statement of Data Access
Data can be requested by contacting corresponding author.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: DMB’s time is supported by an NIH K08 Career Development Award (grant no. K08AR080260-01). LC is a consultant whose time is supported by the Center for Biostatistics and Data Science. The other authors did not receive funding for this project.
Supplemental material is available in the online version of the article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.