
Abstract
Background:
The purpose of this study was to evaluate differences in 90-day clinical outcomes between patients treated with generic volar locking plates (VLPs) and conventional VLPs in distal radius fractures. Secondary aims included assessing for differences in surgical characteristics and cost between the groups.
Methods:
From November 2022 to April 2023, a prospective block-randomized study was undertaken in which surgeons alternated between using a generic VLP and a conventional VLP each month. The institution’s chargemaster database was cross-referenced for implant cost. Primary outcomes were 90-day readmission, reoperation, and mortality rates. Secondary outcomes included estimated blood loss, tourniquet time, and implant cost.
Results:
A total of 66 patients were included. Most were women (n = 61, 92.4%), with an average age of 61.0 ± 11.5 years. There were no significant differences in age, sex, smoking status, AO Foundation/Orthopaedic Trauma Association classification, or tourniquet time between patients who received generic and conventional implants. The average total cost was higher with conventional implants than generic implants($1348.61 ± 100.77 and $702.38 ± 47.83, respectively; P < .001). The largest difference in cost came from pegs and screws that were used ($640.77 ± 90.93 vs $268.47 ± 45.93, P < .001). No patients experienced complications such as readmission, reoperation, or death within 90 days.
Conclusions:
Total implant cost was lower for procedures where generic VLPs were used. Cost differences between generic and conventional implants are driven by the variable selection of pegs and screws. With no differences in 90-day outcomes, surgeons may consider using generic implants as a way of increasing the value of care delivery.
Keywords
Introduction
Healthcare costs continue to rise in the United States while Medicare reimbursement rates are declining. 1 With that, orthopedic surgery is becoming a common target of cost containment strategies as musculoskeletal-related procedures account for approximately one-quarter of surgical procedures performed in the United States. 2 In addition, Medicare reimburses for roughly one-third of all orthopedic procedures. 3 One of the largest contributors to the overall cost of orthopedic procedures is implant cost. On average, implants attribute to 43% to 50% of procedure costs, and in some cases up to 87% of costs. 4 Implant selection is also largely influenced by surgeons, although many are not aware of implant cost.5,6 With implants accounting for a large proportion of overall cost, and being heavily determined by surgeons, implant-related cost reduction strategies such as using generic implants are critical to lowering costs in orthopedic surgery.
Generic implant use has been shown to generate an average cost savings of 49%, and in some cases up to 73% in orthopedic trauma procedures. 7 Despite the reduction in cost related to generic implant use, it appears that there is still some concern among surgeons and patients over their quality and safety. One survey reported that 52% of the public see the value of generic implants; however, only 26% would want them used in their surgery. 8 Regarding surgeons, an Orthopaedic Trauma Association (OTA) member survey found that many are aware of generic implants (73%), but only 26% use them in practice. 9 Prior literature has compared generic cephalomedullary nails (CMNs) to brand name CMNs and found no difference in 6-month clinical and radiographic outcomes.10,11 Although this has been demonstrated in other injury patterns, there is a paucity of literature surrounding differences in cost and clinical outcomes associated with generic implant use in distal radius fracture (DRF) open reduction and internal fixation (ORIF).
The DRFs are a prime target for generic implant implementation due to the relatively high incidence of DRFs (634 000 annually) 12 and the substantial amount spent by Medicare each year on DRF management ($385-$535 million).13,14 The purpose of this study was to assess for differences in 90-day clinical outcomes between patients treated with generic volar locking plates (VLPs) and conventional VLPs in the setting of a DRF. We hypothesized that there would be no difference in clinical outcomes (eg, reoperation); however, there would be reduced cost in the generic VLP group. Secondary aims include evaluating for group differences in surgical characteristics (eg, tourniquet times) and implant cost.
Materials and Methods
A prospective randomized controlled study was conducted at the study institution from November 2022 to April 2023. The local institutional review board approved this study and was registered at http://www.clinicaltrials.gov/ (NCT06343467). Six surgeons who regularly perform DRF ORIF were included (5 hand and 1 orthopedic trauma fellowship-trained). These surgeons alternated between using generic and conventional VLPs each month, while maintaining all other perioperative protocols the same (Figures 1-3). Ultimately, the decision to use a generic VLP was left up to surgeon discretion. Patients were included if they experienced an isolated DRF that was treated surgically with a standard VLP. Patients were excluded if a VLP was not used, there was metaphyseal extension, additional fixation was used, the injury was nonisolated, <18 years old, or they sustained an open fracture (Figure 4).
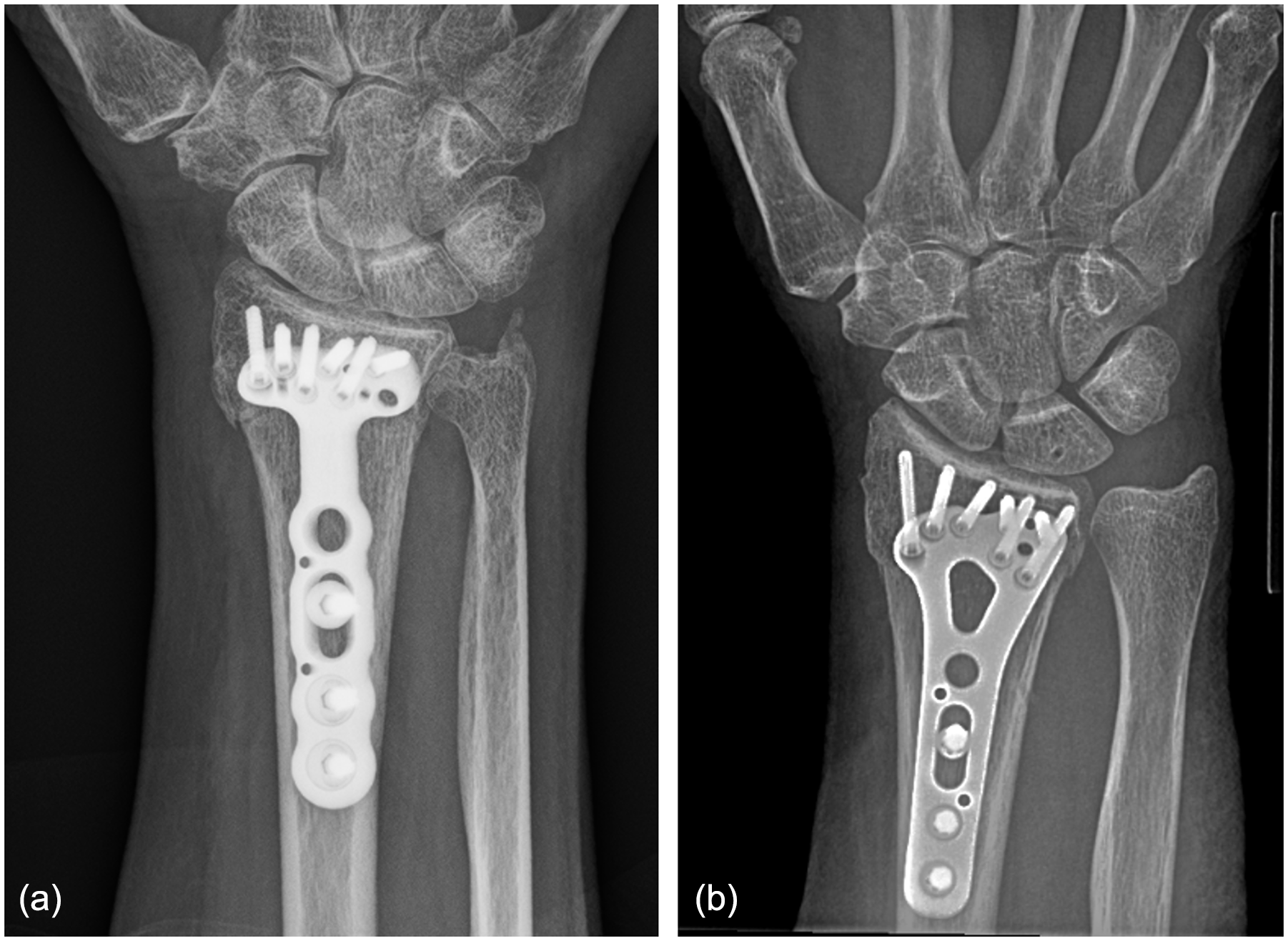
Postoperative radiographs of conventional versus generic volar locking plates. (a) Represents a conventional volar locking plate system. (b) Represents a generic volar locking plate system.
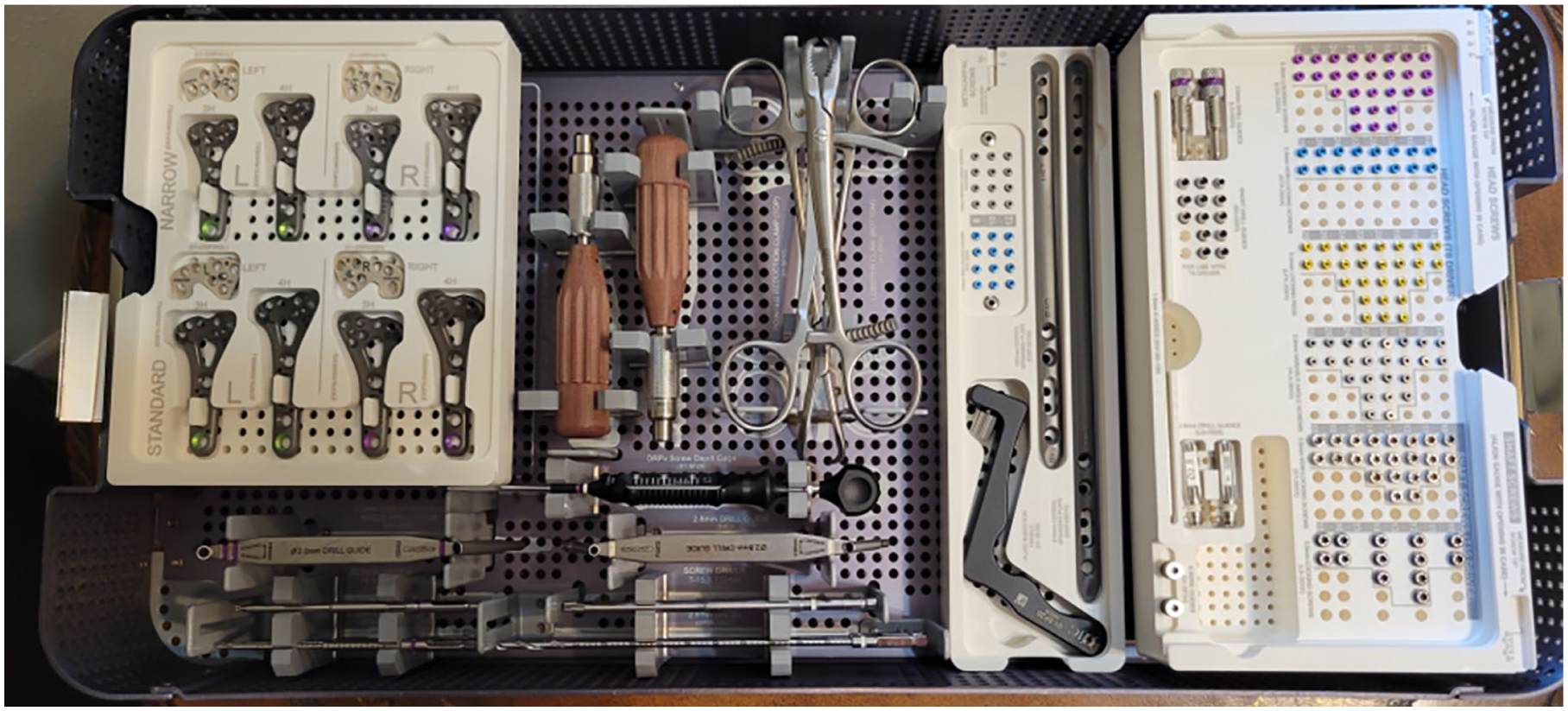
Photograph of the generic volar locking plate tray.
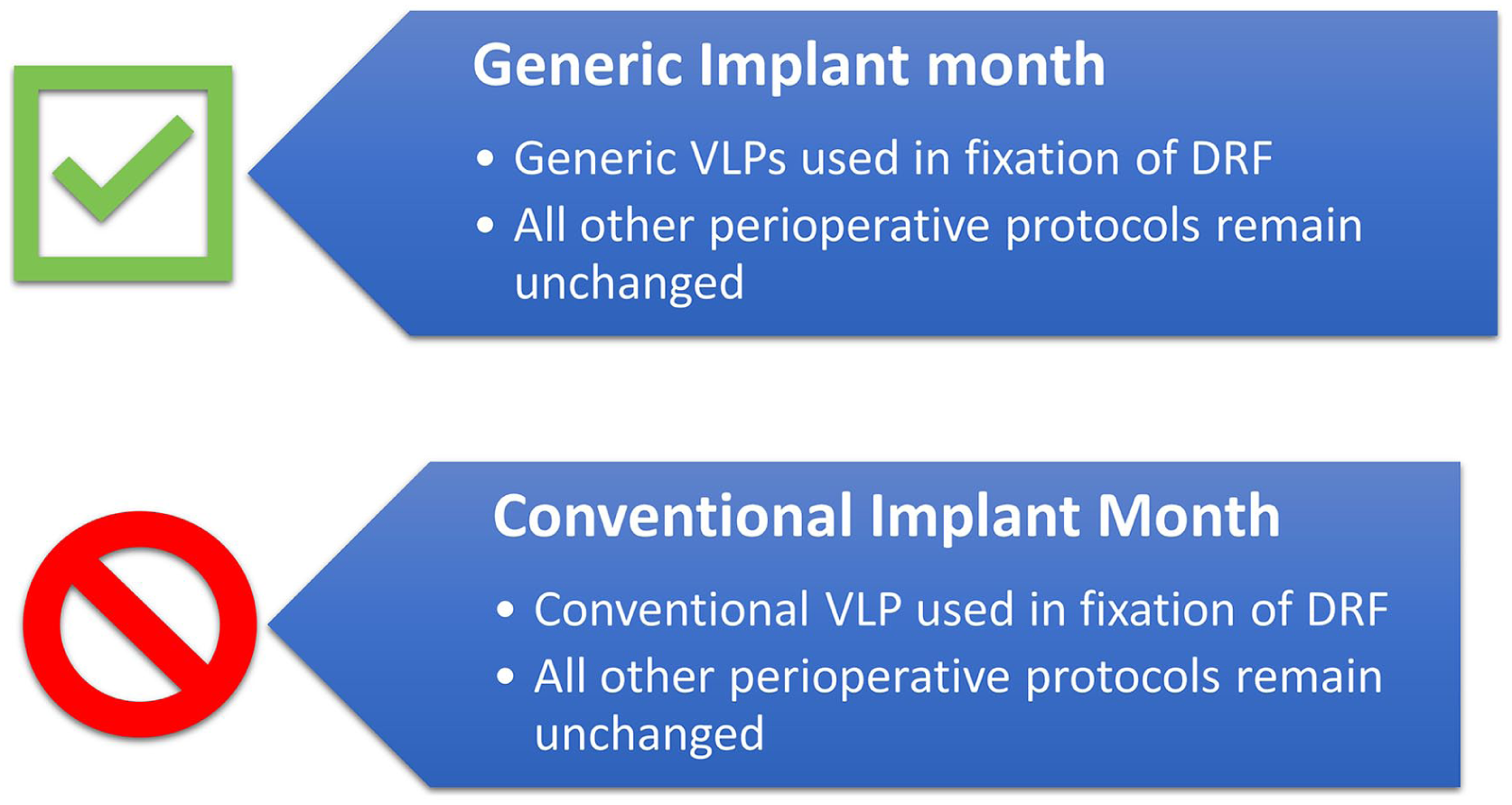
A simplified version of the study protocol.
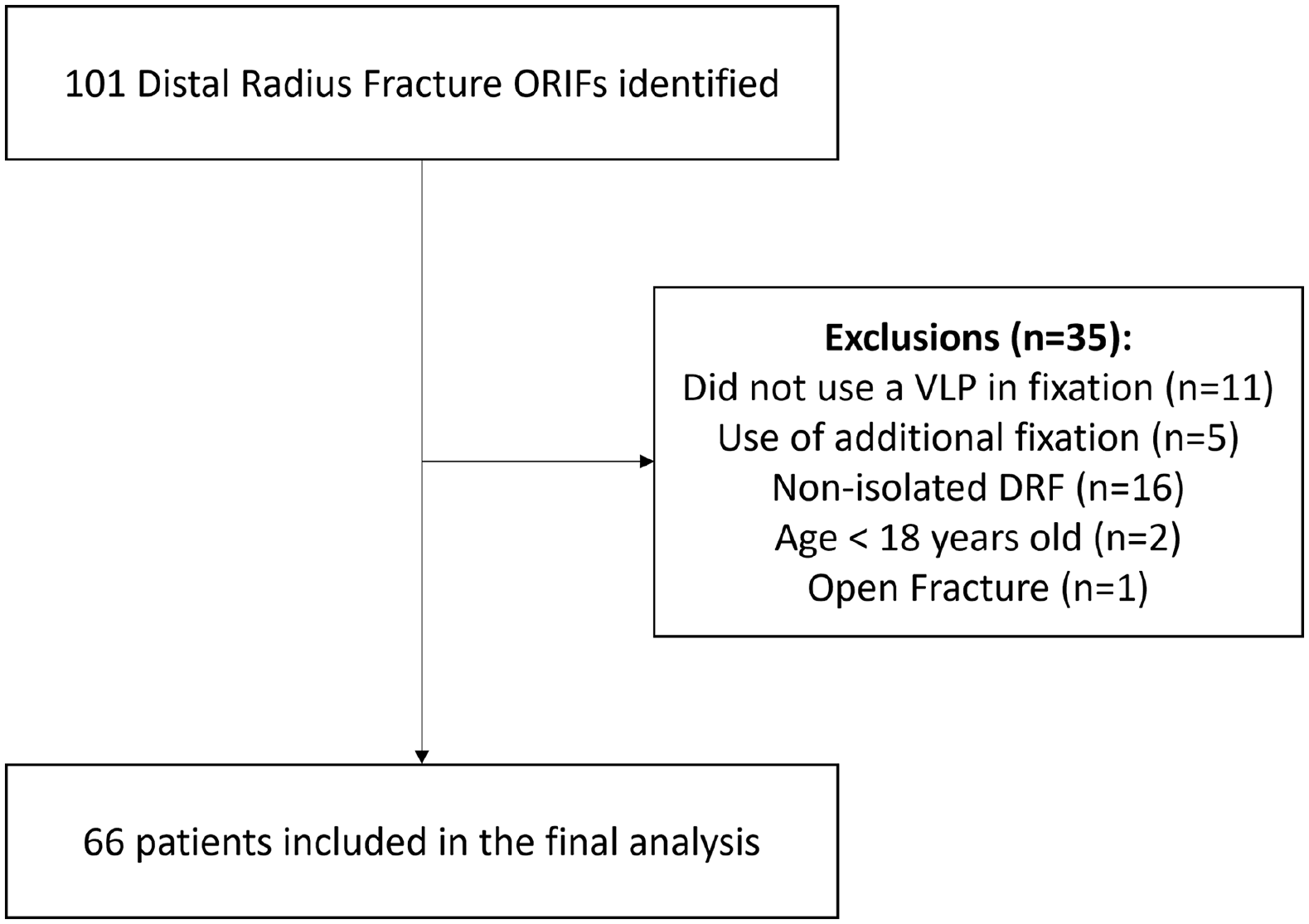
Flow diagram of included patients.
Patient demographics, surgical characteristics, and postoperative complications were collected from the electronic medical record. Demographics consisted of age, sex, body mass index (BMI), smoking history, American Society of Anesthesiologists (ASA) score, injury to dominant wrist, and AO Foundation/Orthopaedic Trauma Association (AO/OTA) classification. Radiographs were reviewed by the senior author. Surgical characteristics included estimated blood loss (EBL), tourniquet time, cost of implants (total, plate, screws/pegs, disposable implants), number of screws/pegs used, and empty holes left in the plate. The primary outcomes included 90-day postoperative outcomes (readmissions, reoperations, and mortality rates) by implant vendor type (generic vs conventional). Secondary outcomes consisted of EBL, tourniquet time, and total implant cost.
All statistical analysis was conducted using Intellectus Statistics (Clearwater, Florida). Fisher exact, chi-square, and independent sample t-tests were used to evaluate for group differences. An a priori power analysis was conducted to estimate the minimum sample size needed to adequately detect a difference in reoperation rates with a large effect size (Cohen d = 0.8). At a type I error rate of 0.05, a power of 80%, and a 1:1 group allocation, the estimated sample size was 36 patients (18 generic VLPs vs 18 conventional VLPs). Statistical significance was set to P ≤ .05.
Results
A total of 66 patients met inclusion criteria for analysis with 47 in the conventional VLP group and 19 in the generic VLP group. The average age for the overall cohort was 61.0 ± 11.5 with most being women (n = 61, 92.4%). Most had an ASA score of 2 (n = 49, 74.2%) with an average BMI of 25.8 ± 5.3. The most common AO/OTA fracture classification was 23 C (n = 43, 65.2%). The average age did not differ between those who received a conventional plate compared with those who did not (60.7 ± 11.4 [57.4, 64.0] vs 61.8 ± 12.1 [56.4, 67.2], P = .749). There were more women than men in the conventional VLP group (n = 43, 91.5%) as well as the generic VLP group (n = 18, 94.7%) (P = 1.000). Smoking history, BMI, and ASA score did not differ between the groups (P > .245). Similarly, the proportion of patients who injured their dominant wrist did not differ between the groups (40.4% vs 26.3%, P = .398). The distribution of DRFs within the AO/OTA classification did not differ by implant vendor (P = .735) (Table 1).
Demographics of Patients by Implant Vendor (N = 66).

Note. Continuous data reported as mean ± standard deviation [95% confidence interval]. Categorical data reported as N/n (%). BMI = body mass index; ASA = American Society of Anesthesiologists; AO/OTA = AO Foundation/Orthopaedic Trauma Association.
The EBL was similar between the groups (13.1 ± 6.8 [11.2, 15.0] mL vs 13.3 ± 10.2 [8.7, 17.9] mL, P = .934). Tourniquet time was also not found to be significantly different regardless of VLP type (45.1 ± 12.8 [41.4, 48.8] minutes vs 49.1 ± 19.2 [40.5, 57.7] minutes, P = .329). The total implant cost for the generic VLP group ($702.38 ± 47.83 [679.34, 725.42]) was found to be significantly lower than the conventional group ($1348.61 ± 100.77 [1319.80, 1377.42], P < .001) (Figure 5). Costs were also significantly lower for the generic VLP group compared with the conventional VLP group for each individual component including plates ($334.47 ± 10.79 [329.27, 339.67] vs $550.64 ± 4.38 [549.39, 551.89], P < .001), screws/pegs ($268.47 ± 45.93 [246.34, 290.60] vs $640.77 ± 90.93 [614.77, 666.77], P < .001), and disposable implants ($99.43 ± 22.96 [88.37, 110.49] vs $157.20 ± 28.93 [148.93, 165.47], P < .001). There were less screws/pegs used in the generic group (8.7 ± 1.0 [8.2, 9.2]) compared with the conventional group (9.6 ± 1.5 [9.2, 10.0], P = .026); however, there was no difference in the number of empty screw holes left in the plate (1.6 ± 0.9 [1.1, 2.0] vs 1.0 ± 1.4 [0.6, 1.4], P = .070). There were no 90-day readmissions, reoperations, or deaths in either group (n = 0, 0.0%) (Table 2).
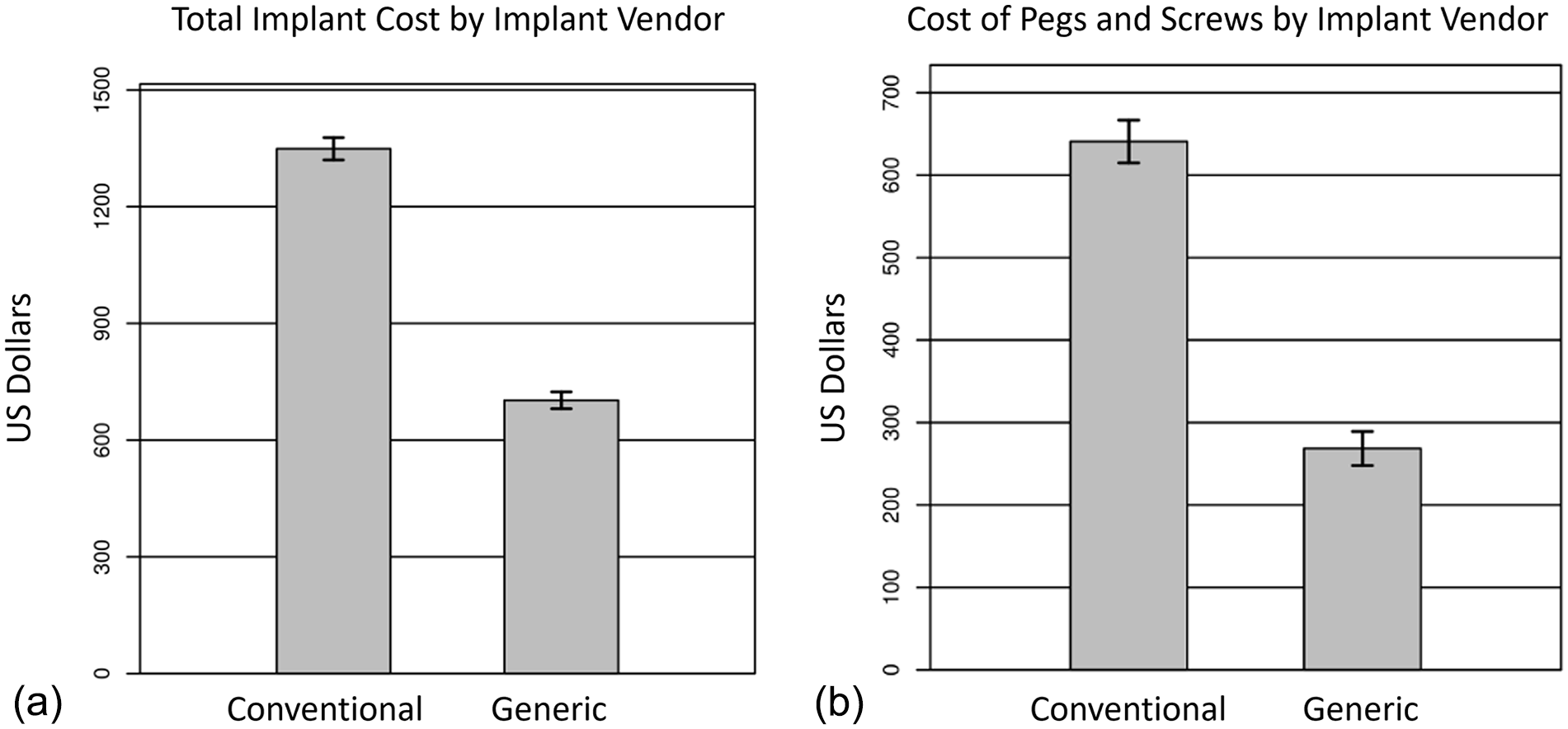
Cost differences between conventional and generic volar locking plate systems. (a) Represents total implant costs. (b) Represents costs of pegs and screws by vendor type.
Surgical Characteristics and Outcomes of Patients by Implant Vendor (N = 66).

Note. Continuous data reported as mean ± standard deviation [95% confidence interval]. Categorical data reported as N/n (%). Bold text indicates statistical significance as defined by a P value ≤ .05.
Discussion
As health care costs continue to rise in North America, it is vital to find and implement effective value-based care strategies. The purpose of this study was to evaluate for differences in clinical outcomes between patients who underwent DRF ORIF with a generic VLP compared with those treated with a conventional VLP. This study demonstrated that there were no significant differences in 90-day clinical outcomes, including patient readmission, reoperation, or mortality (0.0%). Interestingly, tourniquet times were also similar between the groups even though none of the surgeons had used the generic VLP prior to the start of the study. Moreover, there was a significant difference in costs with generic VLP systems costing on average $640 less than conventional plating systems (47.9% cost savings). The largest difference in cost came from screws/pegs with the generic group costing $268 versus $640 on average. These results suggest that generic implant use in DRF ORIF is a viable cost containment strategy that will reduce the cost of care while not hindering patient outcomes, thereby increasing the overall value of the procedure.
Although the method of treatment is controversial in DRF management, when treated surgically, many opt for the VLP. To maximize the value of this procedure, one can reduce costs or improve patient-reported outcomes (PROs). 15 Prior literature has shown that there is minimal variation in implant cost when a VLP is chosen for fixation which may limit the implant cost reduction lever arm when using brand-name implants. 16 It has also been demonstrated that increased VLP implant costs are not associated with increased patient-reported wrist evaluation scores at 6 or 12 weeks postoperatively. 17 The same study also found that construct cost does not vary with injury pattern with VLPs (23A vs 23B vs 23 C). 17 These findings suggest that patients do not benefit from more expensive implants, even with increasing injury severity. The current study demonstrated that there was no difference in 90-day clinical outcomes further confirming that less costly implants such as generic implants can still allow for reductions in the cost of care without hindering patient outcomes. Future studies should seek to evaluate generic VLPs and postoperative PROs to assess the patient perspective more fully on treatment and recovery.
Generic implant implementation in orthopedic surgery provides an opportunity for substantial cost savings. One single-surgeon study found cost savings of more than $250 000 by implementing generic implants at their institution. 7 Another study was able to realize a 56% reduction in implant costs and a total savings of $458 000. 18 This study similarly found a cost reduction of 47.9% using generic implants. As stated previously, implants on average represent 43% to 50% of surgical procedure costs. 4 With inpatient procedures, such as DRF ORIF, any cost savings generated from generic implants will directly impact the margins of the case per the diagnostic-related group. Regarding generic medications, prior studies have demonstrated their application in the United States to have generated $33 billion in savings in 2007.10,19 Further savings have been realized since then, with more recent literature indicating annual savings amounting to $254 billion. 20 Assuming a similar integration pattern for generic implants in orthopedics, the potential savings would be considerable.
The largest difference in driver of cost differences between the generic and conventional VLP systems came from screws/pegs. Other than vendor choice, screw type has also been implicated in cost with multidirectional/variable angle screws and pegs being more costly than nonlocking or nonvariable angle locking screws/pegs. 16 The effect of screw type on cost has also been demonstrated in other injury patterns (ankle and humeral shaft fractures), with locking screws, and cannulated screws being more costly.21,22 Surgeons have the ability to affect cost by selecting not only the implant vendor, but also the number and types of screws as well. The overall number of screws used in the VLP may be another way to mitigate cost in DRF management. In spine surgery, one study evaluated patients with a low density of screws compared with a high density and found no differences in patient outcomes; however, the costs were significantly decreased in the low-density group compared with the high-density group ($10 819 vs $13 272). 23 Previous biomechanical literature suggests that alternating 4 locking screws distally may be sufficient for fixation of DRFs.24 -26 The current study demonstrated that on average there was approximately one less screw used in the generic group, and there were more open holes left in the plate although the later only trended toward significance. This difference may have contributed to the overall cost difference although it only played a small part, with generic locking screws costing $40 each in this study. Future studies should endeavor to evaluate the number and type of screws necessary for fixation in DRFs by correlating constructs with PROs, clinical, and radiographic outcomes to maximize the value in DRF ORIF.
This study had a number of strengths and weaknesses. One strength was the use of a prospective, block-randomized protocol to limit any selection bias. All surgeons included in the study regularly use VLPs for DRF ORIF as part of their practice. Procedures were performed at varying facility acuity levels (ambulatory surgery centers vs hospitals) allowing for generalizability to other health care systems. Implant prices can vary greatly by health care system that largely depends on contract negotiations with implant vendors. This can limit the direct applicability of the cost savings and prices reported in this study; however, these findings can provide a better understanding of potential cost savings health care systems can realize with generic implant use. Future studies with generic implants should endeavor to use PRO measures to further evaluate the relationship between implant vendor and quality of care provided. The power analysis for this study was based on the primary outcome of cost and may not be sufficiently powered to evaluate for differences in some of the other findings such as with the number of pegs/screws used or empty holes left in the VLP. Finally, this study is limited to only 90 days of follow-up which hinders any evaluation of potential postoperative differences that may exist between the VLP vendors with longer follow-up.
Generic VLP systems were associated with no significant differences in clinical outcomes, EBL, and tourniquet times, while providing significantly lower costs than conventional plating systems. The largest difference in cost came from pegs/screw costs ($372). In a health care climate with increasing pressure to reduce health care expenditure, the use of generic VLPs in DRF ORIF can provide an opportunity for an average of 47.9% in cost savings. With implants being one of the largest cost drivers in orthopedics, surgeons should be cognizant of their implant choices as less costlier options may provide the same outcomes for their patients while minimizing costs.
Footnotes
Authors’ Note
Jeffrey B. Husband is also affiliated to Park Nicollet Methodist Hospital, St. Louis Park, MN, USA.
Ethical Approval
This study was approved by our institutional review board.
Statement of Human and Animal Rights
All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2008.
Statement of Informed Consent
No informed consent was obtained or required for this study.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: B.P.C’s spouse is the CEO and founder of CODE Technology. B.P.C. is a member of the AAOS Health Care Systems and Patient-reported Outcome Measures Committees as well as the chair of the OTA Practice Management Committee. He is also a member of the editorial board for the Journal of Orthopaedic Business. D.C.B. has stock in Bristol Myers Squibb, Eli Lilly, and Pfizer. The remaining authors have no conflicts of interest to disclose.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Trial Registration
ClinicalTrials.gov ID: NCT06343467