
Abstract
Background:
Multiple options exist for reconstruction of the interosseous membrane (IOM) including biologic and nonbiologic materials. In this study, we present the biomechanical properties of reconstruction of the IOM using suture button suspension with and without pronator teres (PT) tendon rerouting.
Methods:
Using 8 cadaveric specimens, radioulnar displacement was tested for the following successive conditions: intact specimen, IOM release with radial head (RH) resection, IOM reconstruction with PT tendon transfer alone, and PT transfer augmented with a suture button suspension construct with and without RH replacement. Specimens were cyclically loaded with 3 compression cycles to 130 N using a uniaxial materials test apparatus. Radioulnar displacement was the primary endpoint measured by the crosshead displacement. A repeated measure 1-way analysis of variance (ANOVA) and Tukey test was used for statistical analysis using P < .05.
Results:
Interosseous membrane reconstruction with a PT soft-tissue graft supplemented with a suture button suspension construct with concomitant RH arthroplasty did not significantly decrease mean radioulnar displacement (PT Recon w/ RH: 2.99 ± 1.92 mm, TightRope w/ RH (2.88 ± 1.56 mm, P > .05). The use of suture button suspension augmentation did not significantly increase the stiffness of the PT IOM reconstruction construct when used concomitantly with an RH arthroplasty (PT Recon w/ RH: 82.48 N/mm, TightRope w RH: 71.51 N/mm, P > .05).
Conclusions:
Pronator teres transfer with suture button augmentation effectively restores radioulnar stability. No significant differences in stability were observed between PT transfer with and without suture button suspension augmentation.
Keywords
Introduction
Instability of the forearm occurs most often as a result of axial loading of the outstretched upper extremity with the forearm in pronation. 1 Load transmission through the wrist, interosseous membrane (IOM), and proximally through the ulnohumeral and radiocapitellar joints results in varying degrees of disruption of the static and dynamic stabilization of the forearm axis. Disruption of the distal radioulnar joint (DRUJ), IOM rupture, and radial head (RH) fracture have each been previously implicated in the tendency toward longitudinal and transverse instability of the forearm.2,3 Of particular importance is the central band of the IOM, which plays a critical role in facilitation of load transmission proximally along the forearm axis.4 -6
Failure to promptly diagnose and manage acute forearm instability may portend less-favorable functional and quality-of-life outcomes than those observed in patients who undergo appropriate management acutely for their injuries. 7 Long-term sequelae of untreated, or inadequately treated, forearm instability include long-term ulnar-sided wrist pain, elbow pain, and decreased grip strength. 8 Repair or replacement arthroplasty of RH fractures in the setting of suspected forearm instability provides a buttress against further proximal migration of the radius. Despite this physical restraint to proximal radial migration, treatment of the RH alone is not sufficient in restoring more physiologic load transmission across of the forearm axis. 2 The addition of an IOM reconstruction does, however, add to the biomechanical stiffness of the forearm axis, and allows for restoration of both longitudinal and transverse load distribution in the forearm.9,10 While several authors have investigated the opportunity for acute repair of the IOM, the results of these procedures have largely been unsatisfactory.11,12 Reconstruction of the IOM provides the opportunity for more physiologic load transference to occur between the distal and proximal forearm. Multiple reconstruction options have been described including the use of autologous tendon or bone-tendon-bone grafts, allograft tissue, and more recently suture button suspension fixation.13,14
The use of suture button suspension constructs for the reconstruction of acute or long-term IOM disruption provides immediate stability to the forearm axis via a minimally invasive surgical approach. The relatively small anatomic footprint of the suture button device also allows for less soft-tissue disruption relative to that of traditional plate and screw or bone-block and screw constructs. 15 Biomechanical data suggest that reconstruction of the IOM using both single- and double-suture-button constructs provides for near anatomic tensile and load distribution forces to be restored to the forearm.15,16 Short-term clinical follow-up of suture-button IOM reconstruction constructs also demonstrates improvements in elbow, forearm, and wrist range of motion, ulnar variance, and patient-reported outcomes postoperatively. While suture-button suspension does allow for immediate restoration of stability to the forearm, the long-term results of this operation are not currently available in the literature. One inherent downside of this construct is its reliance entirely upon hardware without the addition of biologic tissue available for healing to help augment or, in the case of hardware failure, substitute for the hardware construct. We therefore sought to compare the biomechanical properties of suture-button IOM reconstruction with and without the addition of a rerouted pronator teres (PT) autograft. We hypothesized that the addition of the PT rerouting to the suture-button reconstruction would provide for an overall increase in stiffness of the construct and lead to greater resistance to longitudinal radioulnar displacement.
Materials and Methods
Specimen Preparation
Eight fresh-frozen cadaveric upper limb specimens were allowed to slowly thaw to ambient temperature prior to biomechanical preparation and testing. Preparation of each test specimen involved sectioning at the mid-humeral level, approximately 15 cm proximal to the medial epicondyle. The soft tissue was meticulously dissected to expose 10 cm of humerus with screws placed through the exposed bone for embedding each upper extremity into gripping fixtures using Smooth-Cast 320 resin (ultra-low viscosity casting resin manufactured by Smooth-On, Easton, PA) (Figure 1). Each embedded test specimen was supported in a perpendicular position during the curing of the resin (Figure 2).
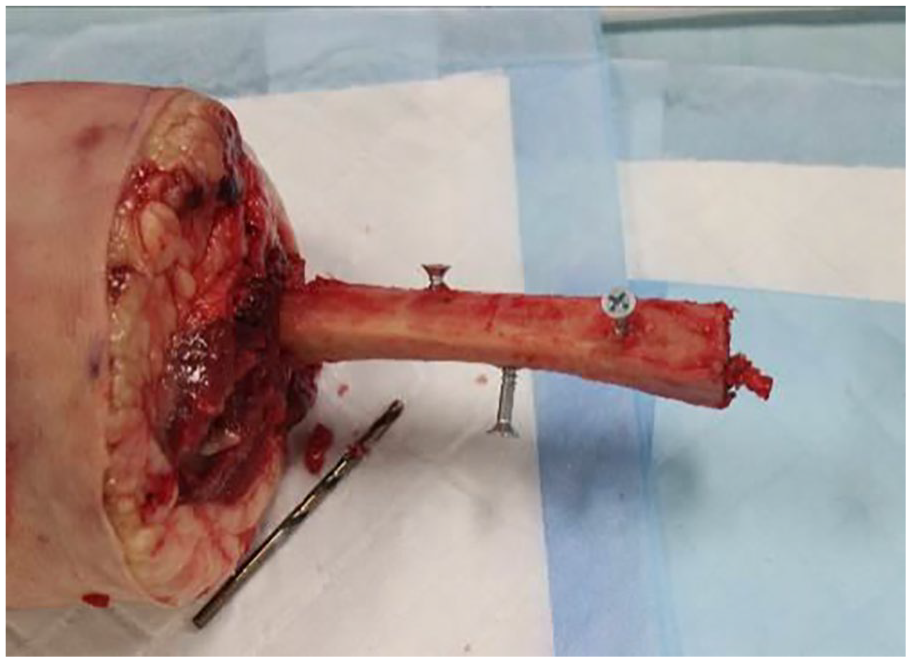
Prepared humerus with reinforcement screws prior to embedding into gripping fixtures.
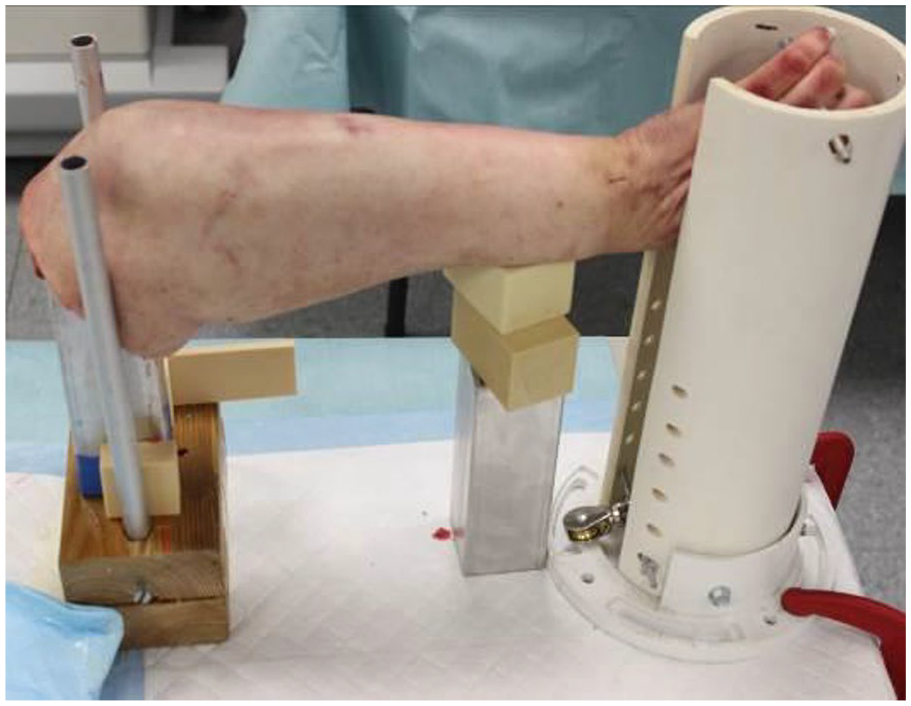
Aluminum embedding fixture for the humerus with the hand gripped perpendicular to humerus.
Prior to testing, an incision was made over the dorsoradial border of the radius at the junction of the middle and distal thirds of the forearm to allow for harvest of the PT tendon as described by Chloros et al, 17 as well as to allow for predrilling of holes for implantation of the TightRope fixation. The PT tendon was released from its insertion on the radial shaft, and a Krakow suture was placed in the tendon using #2 braided, nonabsorbable suture for later reconstruction (Figure 3). Care was taken to retain as much of the PT tendon as possible. After release of the PT, the length of the radius was measured. The radial and ulnar lengths were measured for each specimen to determine the most anatomic position for IOM reconstruction. 18 The radius of each specimen was marked at a level equivalent to 60% of the overall radial length measured from the distal-most portion of the radial styloid. Each ulna was marked at a length corresponding to 30% of the overall ulnar length as measured from the ulnar head.
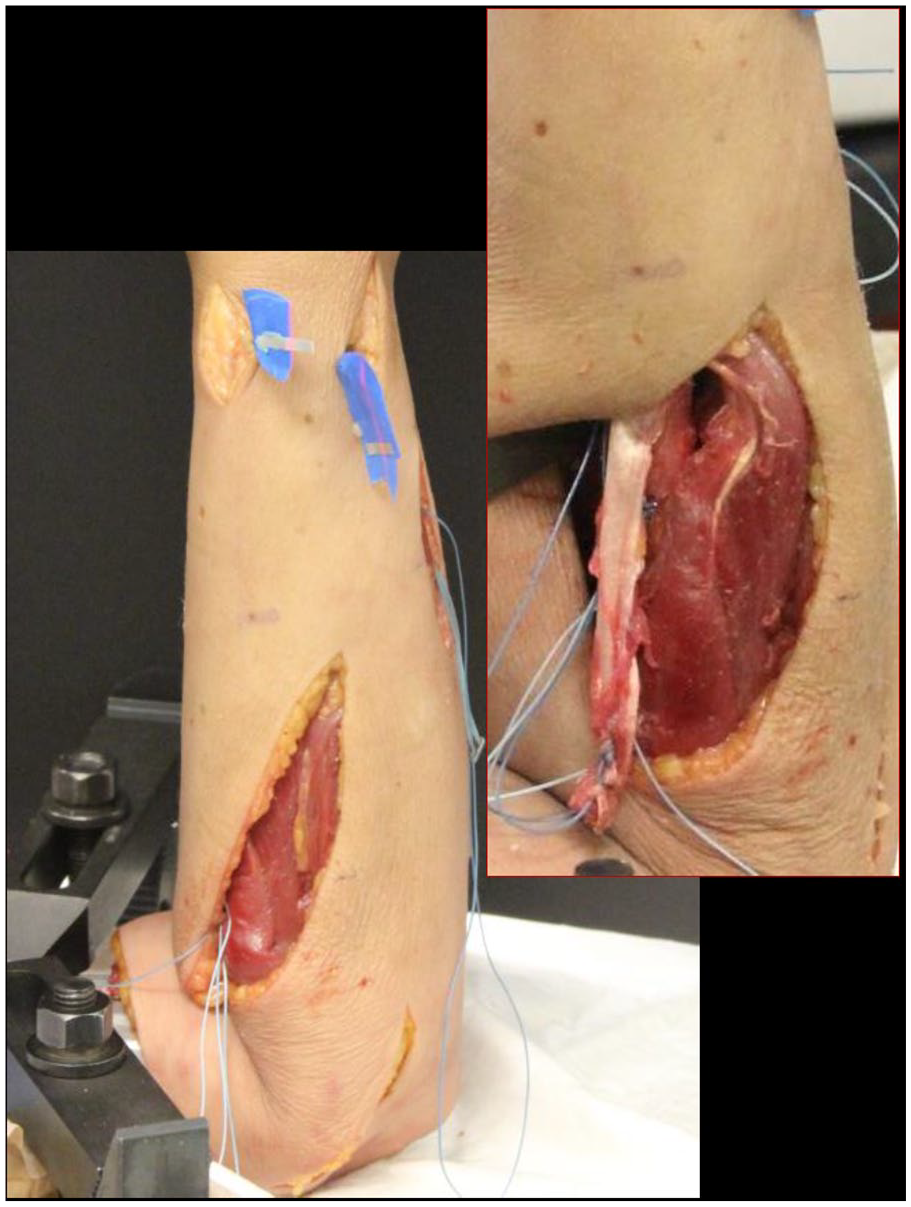
Exposed pronator teres with Krakow stitch placed into the tendon graft.
Under fluoroscopic guidance, a 0.045” Kirschner wire was passed across the radial diaphysis on a posterior-anterior fluoroscopic image at the previous mark corresponding to 60% of the radial length. An additional incision was made over the subcutaneous border of the ulna at the level of the previously marked distance corresponding to 30% of the ulnar length. The 0.045” Kirschner was passed across the ulnar diaphysis under imaging guidance on a posterior-anterior fluoroscopic projection. A suture button suspension device (TightRope, Arthrex Inc., Naples, FL) was then passed from the previously drilled radius hole and out the ulnar side of the previously drilled ulnar hole. The suture button suspension device was left in place but not tensioned until prior to biomechanical testing. The hand and wrist were then removed from each specimen, and 2 fully thread screws were inserted into the distal-most aspect of the exposed radius and were left prominent for attachment on the testing machine. Two additional 1-cm incisions were made in the distal third of the forearm to allow fully threaded cortical screws to be inserted into the radial and ulnar shafts. A final incision was made in the standard Kaplan approach to the RH allowing for removal of the RH during deconstructive testing. All surgical procedures were performed on each specimen while mounted to the testing frame to minimize variables. Calibrated fluoroscopic images were taken of each test specimen for each test configuration. Fluoroscopic images were taken of the DRUJ initially and after the completion of each testing condition.
Biomechanical Testing
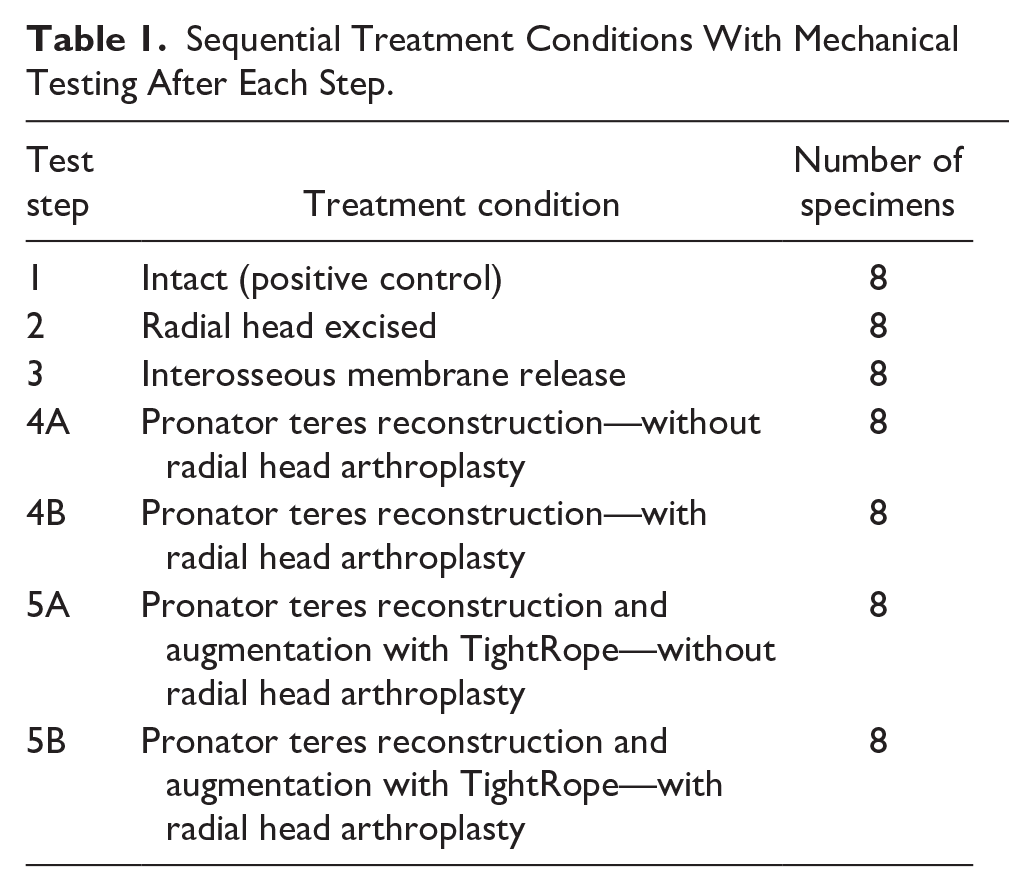
Each embedded specimen was mounted to the electromechanical test machine (MTS Insight, MTS Systems, Eden Prarie, MN) with the humerus affixed to the test table and the forearm in neutral rotation (Figure 4). The superior actuator was anchored to the distal radius via a clamping fixture. A cyclic compressive load was applied to each specimen under force control at a rate of 0.5 mm/s. Specimens were cycled 3 times from 0 to 134 N for each test condition, with the last cycle continuously recorded. The sequential treatment conditions evaluated are outlined in Table 1 with testing conducted after each treatment iteration. Load and displacement data were recorded at a relevant sampling rate (100 Hz). All testing was conducted in ambient air at room temperature.
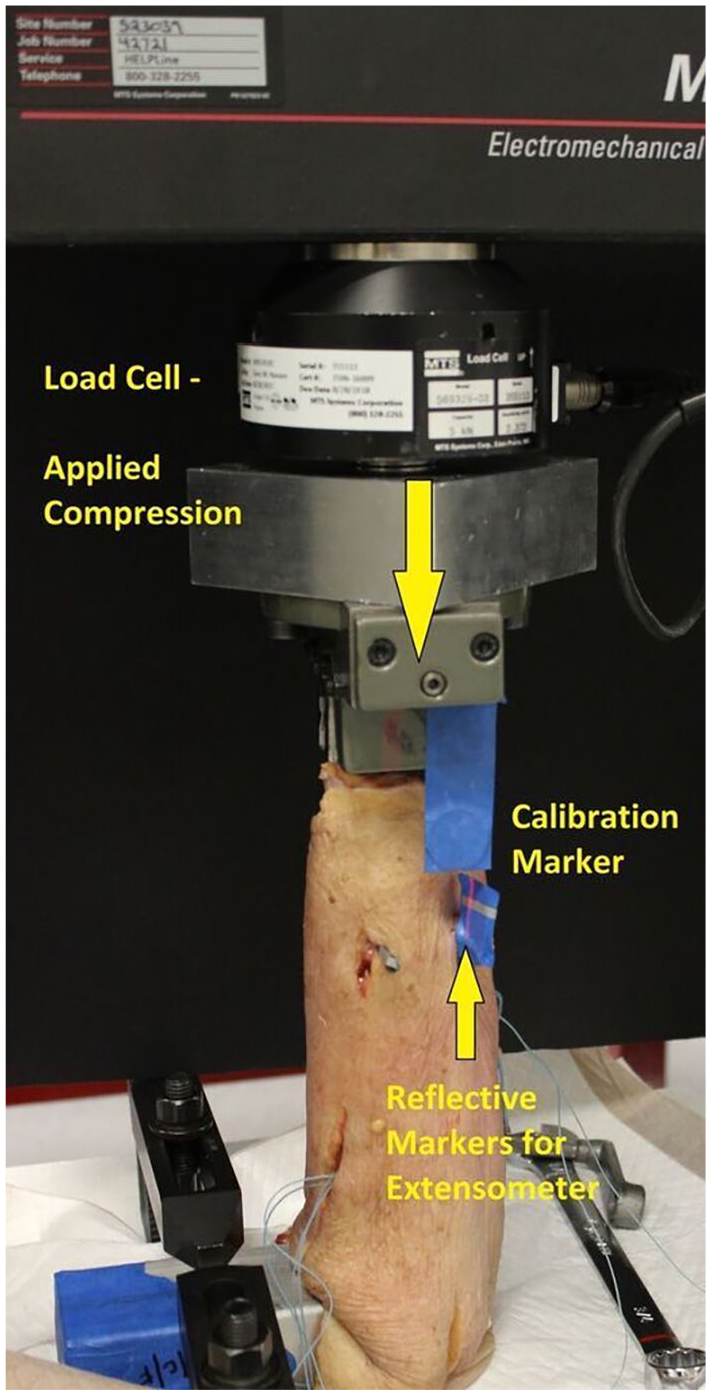
Biomechanical testing construct with mounted specimen.
Sequential Treatment Conditions With Mechanical Testing After Each Step.
Data Analysis
The load (N), crosshead displacement (mm), and stiffness (N/mm), were continuously recorded for each sample tested for each upper limb tested.
Statistical Analysis
A 1-way analysis of variance (ANOVA) with a repeated measures analysis at an alpha of 0.5 was conducted using Prism, Version 6 statistical software (GraphPad Software, San Diego, CA) to provide a comparison between treatment groups with respect to the stiffness and crosshead displacement. The crosshead displacement represented the motion of the radioulnar complex, as it was directly attached via the actuator and clamped to the distal radius. A Tukey’s multiple comparison was run to compare between treatment groups.
Results
Mean longitudinal radioulnar displacement of the intact specimens was 1.32 ± 0.55 mm. The mean longitudinal radioulnar displacements of each specimen condition are summarized in Table 2. Resection of the RH alone led to a significant increase in mean radioulnar displacement (2.86 ± 0.90 mm, 1.32 ± 0.55 mm, P = .0001). Release of the IOM following RH resection led to a significant increase in mean longitudinal radioulnar displacement relative to that of intact specimens (4.45 ± 2.17 mm, 1.32 ± 0.55 mm, P < .0020), as well an increase relative to the specimens with RH resections only (4.45 ± 2.17 mm, 2.86 ± 0.90 mm, P = .0137). Reconstruction of the IOM with a PT soft-tissue graft without replacement of the RH did not provide for a significant decrease in mean radioulnar longitudinal displacement compared to the completely deconstructed state (4.38 ± 2.52 mm, 4.45 ± 2.17 mm, P = .6862). The addition of an RH implant to the PT IOM reconstruction provided for a significant decrease in mean radioulnar displacement (2.99 ± 1.92 mm, P = .0061) compared to both the IOM release and PT reconstruction without RH conditions (P = .0018). Similarly, RH replacement and reconstruction of the IOM with a PT graft with the addition of a TightRope construct (2.88 ± 1.56 mm) provided for a significant decrease in mean longitudinal radioulnar displacement compared to both the IOM release and PT reconstruction without RH conditions (P = .0129 and P = .0320, respectively). Reconstruction of the IOM with PT and a TightRope construct without replacement of the RH significantly decreased mean longitudinal radioulnar displacement compared to the IOM release state (TightRope w/o RH 3.36 ± 1.27 mm, IOM Release 4.45 ± 2.17 mm, P = .0796). No difference in mean longitudinal radioulnar displacement was observed between PT reconstruction with a TightRope construct with an RH replacement or without an RH replacement (TightRope w/ RH 2.88 ± 1.56 mm, TightRope w/o RH 3.36 ± 1.27 mm, P = .3707). The addition of 1 TightRope to the PT IOM reconstruction with an RH replacement in place did not lead to a significant decrease in mean longitudinal radioulnar displacement (TightRope w/ RH 2.88 ± 1.56 mm, PT Recon w/ RH 2.99 ± 1.92 mm, P = .6781).
Radioulnar Complex Displacement.
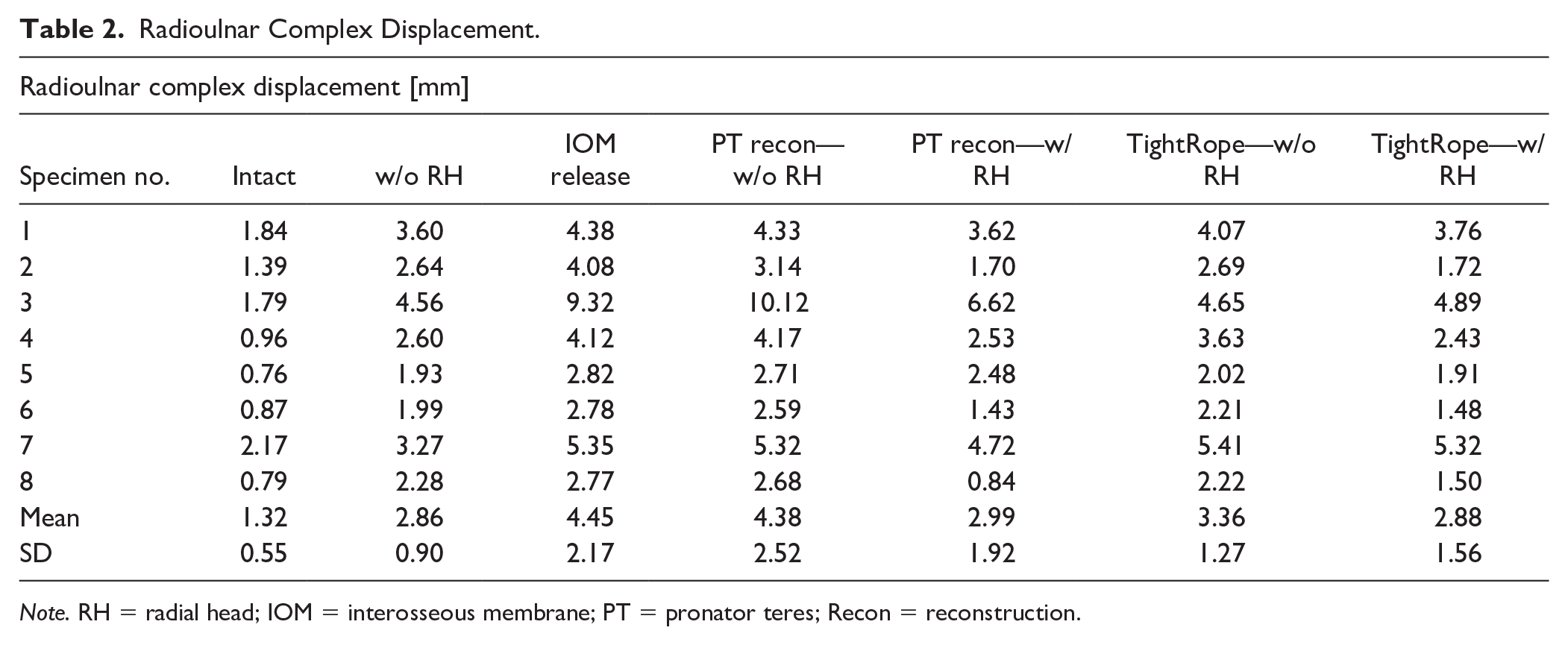
Note. RH = radial head; IOM = interosseous membrane; PT = pronator teres; Recon = reconstruction.
The intact specimen condition was noted to exhibit significantly greater mean stiffness (N/m) than each deconstructive and reconstructed condition. The stiffness values for each specimen condition are summarized in Table 3. Sequential deconstruction of the forearm axis was notable for statistically significant decreases in mean stiffness in the intact state compared to the resection of the RH (135.73 ± 52.57 N/mm, 60.31 ± 17.22 N/mm, P = .0006). However, subsequent division of the IOM following RH resection did not lead to a significant decrease in forearm stiffness (60.31 ± 17.22 mm, 41.88 ± 11.78 N/mm, P > .05). Reconstruction of the IOM without the addition of an RH arthroplasty implant did not confer a significant increase in stiffness relative to the IOM release state regardless of the reconstruction construct used (PT w/o RH 43.34 ± 12.63 N/mm, 1 TightRope w/o RH 49.45 + 19.41 N/mm, P = .4697). The addition of an RH arthroplasty following PT IOM reconstruction provided for a significant increase in stiffness (82.48 ± 49.03 N/mm, 43.34 ± 12.63 N/mm, P = .0328). The addition of an RH arthroplasty implant to the TightRope reconstruction construct was not associated with a significant increase in mean stiffness relative to the w/o RH state (P = .1940).
Radioulnar Complex Stiffness.
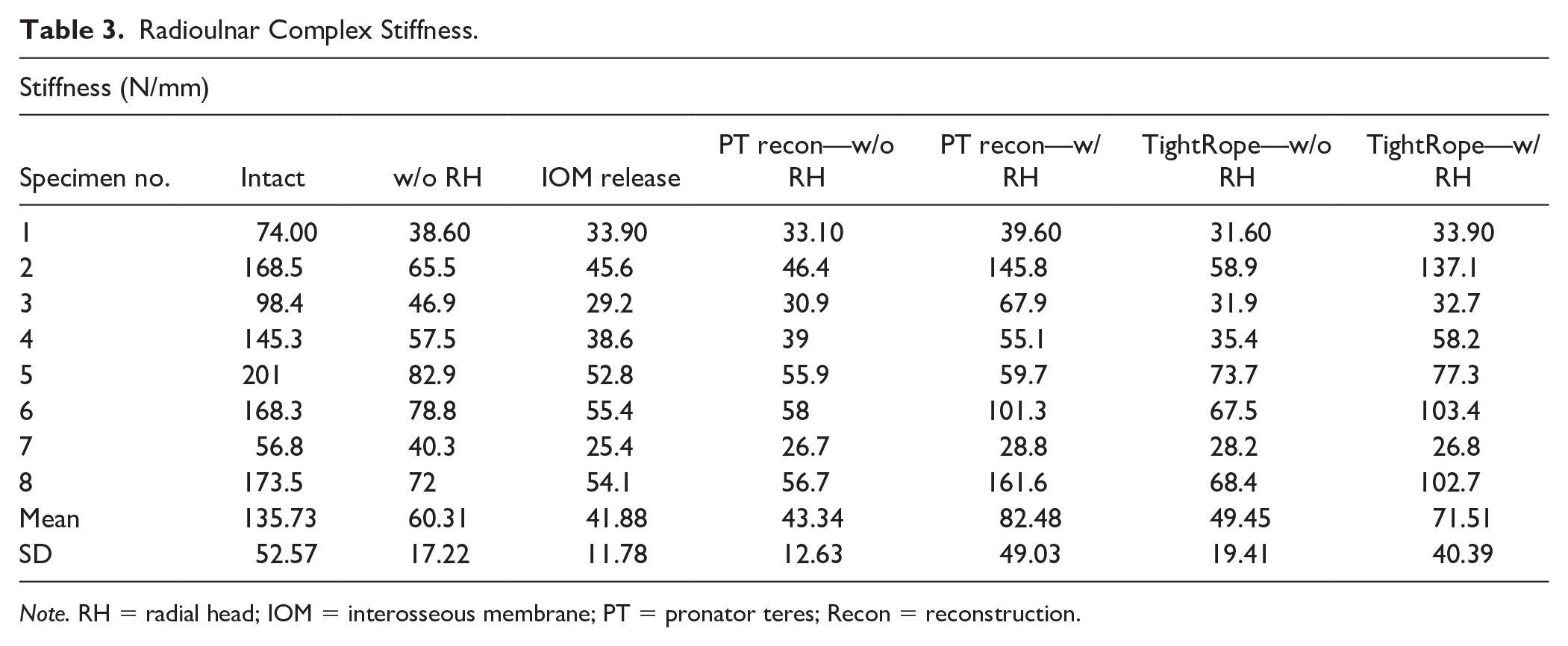
Note. RH = radial head; IOM = interosseous membrane; PT = pronator teres; Recon = reconstruction.
Discussion
Maintenance of axial stability of the forearm is predicated upon the integrity of multiple structures including the RH, IOM, and triangular fibrocartilage complex. 3 Disruption of either the static or dynamic stabilizers of the forearm axis can result in longitudinal instability of the forearm, altered load transmission about the wrist and elbow, and significant disability of the affected extremity. 4 Prompt identification and management of longitudinal forearm instability in the acute setting provides for the best opportunity to avoid the long-term sequalae of untreated instability. 8
Management of longitudinal forearm instability requires attention to each radiocapitellar articulation, IOM, and DRUJ. 13 While some surgeons opt for only percutaneous fixation across the radius and ulna for stabilization of the forearm axis in the setting of longitudinal forearm instability, there is no biomechanical evidence available to support the use of this fixation alone. The authors feel that transosseous fixation alone is likely insufficient in providing long-term reduction and stabilization of the forearm axis. Reconstruction of the IOM has been described using multiple autogenous and allograft tissues including the PT, flexor carpi radialis, semitendinosus, palmaris longus, Achilles tendon, and patellar tendon. 19 Recent interest in nonbiologic options for reconstruction of the IOM has shown promising results in the literature with respect to restoration of stiffness of the forearm axis. 15 Our results suggest that reconstruction of the IOM with both a PT autograft tendon reconstruction with the addition of a suture button suspension construct does not provide for increase in immediate stiffness of the forearm axis or resistance to translational motion of the forearm in the ex-vivo state. This lack of overall increased biomechanical stability remained true both in the presence and absence of an RH arthroplasty implant. While these results do not suggest a significant additive benefit to use of both a soft-tissue reconstruction and a suture button reconstruction construct, the overall benefit of such a construct may be better appreciated in vivo.
Reconstruction of the IOM with biologic tissues such as tendon or bone-tendon grafts does provide for some degree of initial inherent stability; however, the maximal stability of such a construct may not be appreciated until this biologic tissue has incorporated which may take between 6 and 12 weeks. During this time period, there is a risk of graft elongation or failure which may render the reconstruction construct unable to provide the necessary degree of stability to the forearm axis. The use of both an autogenous tendon graft reconstruction (in this case the PT) and a nonbiologic reconstruction provides the theoretical benefit of allowing for conference of immediate stability via a construct which is not dependent upon local biologic factors for long-term stability. The suture button construct serves as an internal splint to maintain the desired relative position of the forearm axis and resist translation forces between the radius and ulna in the interval while the biologic tissue graft begins to incorporate. Maintenance of the desired forearm alignment in the early postoperative period may allow for more rapid mobilization of the patient with a decreased risk of attenuation or failure of the biologic graft used.
Our results regarding the degree of observed radioulnar displacement in the suture button construct with the addition of an RH arthroplasty (2.88 ± 1.56 mm) are slightly greater than those previously observed in the literature (2.2 ± 0.9 mm, 1.1 ± 0.6 mm).15,20 There are several technical differences in the testing paradigm used which may contribute to differences in the observed results. Hackl et al 20 evaluated the biomechanical stiffness of each a single- and double-suture-button IOM reconstruction construct in a cadaveric model using 8 specimens. In this model, all of the soft tissues about the forearm axis were removed except for the IOM, proximal radioulnar joint ligamentous complex, and DRUJ ligamentous complex. The cadaveric forearms were loaded such that the proximal portion of the cadaveric limb was positioned on the testing table, similar to our study; however, the differences in the relative degree of tissue dissected and selected anatomic locations for fixation of the cadaveric limbs to the testing frame may account for the differences in stiffness and radioulnar displacement observed. Kam et al 15 evaluated a single suture button IOM reconstruction construct in a cadaveric model using 8 specimens. In this biomechanical testing model, the soft tissues about the cadaveric limb distal to the mid-humerus were retained, similar to the protocol used in our cadaveric model. One notable difference in our study is the disarticulation through the rest rather than maintenance of the tissue distal to the radiocarpal articulation during biomechanical testing. The cadaveric limbs in Kam et al’s testing paradigm were mounted vertically downward such that the hand was positioned closest to the base of the testing frame, the inverse of what was performed in our testing model. This relative change in positioning of the limb for loading, extent of tissues distal to the radiocarpal joint present in the cadaveric limb during testing, as well as the differences in the anatomic location of the sensors used to measure the observe displacement may account for the observed differences in results.
Limitations of this study include the relatively small number of anatomic specimens used for testing. A total of 8 specimens were tested for each treatment condition, similar to the number of specimens used for similar biomechanical testing protocols in the literature for suture button reconstruction of the IOM.15,20 Future studies should seek to expand upon the number of specimens tested and test different specimens individually for each degree of deconstruction of the forearm axis independently rather than serially sectioning the same specimen for each level of deconstruction and reconstruction. One additional limitation is the cadaveric nature of the study which may underappreciate the relative contributions of the dynamic stabilizers of the forearm axis in vivo.
Reconstruction of the central band of the IOM can be conducted via multiple biologic and nonbiologic means. The use of a suture button construct for reconstruction of the IOM has previously been shown to effectively stabilize the forearm axis and provide for favorable results both in cadaveric models as well as a limited clinical case reports. In this study, we sought to further describe the biomechanical properties of a combined biologic and nonbiologic reconstruction of the central band of the IOM. The use of both biologic and nonbiologic materials for reconstruction of the IOM may provide the benefit of both immediate inherent stability of the forearm axis, while providing protection against early elongation and failure of the biologic tissues used for reconstruction. Further studies regarding the clinical results of this reconstruction paradigm may provide for a better understanding of the role of the described reconstruction construct in the management of both acute and long-term longitudinal forearm instability.
Footnotes
Ethical Approval
This study was approved by our Institutional Review Board.
Statement of Human and Animal Rights
The article does not contain any studies with human or animal subjects.
Statement of Informed Consent
The article does not contain any studies with human or animal subjects, and as such no informed consent was required prior to study completion.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: LF received a research grant from OrthoCarolina to cover the costs of testing and materials. BL received donations from Arthrex for suture button constructs and radial heads from Wright Medical (Stryker). The remaining authors have nothing to disclose.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.