
Abstract
Background:
Severe proximal interphalangeal (PIP) contractures in Dupuytren disease significantly impair hand function and quality of life. Surgical correction is common, but the relationship between improved joint mobility and patient-reported outcomes remains unclear. This study evaluated surgical outcomes for severe PIP contractures and assessed patient-reported function using Patient-Reported Outcomes Measurement Information System (PROMIS).
Methods:
A retrospective chart review included patients with severe PIP contractures treated surgically. Contractures were categorized by severity: group 1 (<29°), group 2 (30°-59°), group 3 (60°-89°), and group 4 (>90°). Objective outcomes were measured as contracture reduction at multiple time points (preoperative, immediate postoperative, and final follow-up) using a goniometer. The PROMIS scores for pain intensity, daily activity interference, and upper extremity function were collected preoperatively and at final follow-up. Statistical analyses included descriptive statistics, paired t tests, and analysis of variance with post hoc Tukey tests (P < .05).
Results:
The study included 60 digits from 48 patients. Significant contracture reductions were observed across all groups, averaging more than 60%. However, PROMIS scores did not consistently reflect improvements in pain, activity interference, or upper extremity function. A significant decrease in upper extremity function was noted in group 3 (60°-89°). No operative complications or reoperations occurred.
Conclusions:
Surgical correction markedly improves joint contracture but does not consistently enhance PROMIS-reported outcomes. These results question PROMIS applicability in this context and highlight the need for alternative assessment tools to better address functional recovery in patients with severe PIP contractures.
Introduction
Dupuytren disease is characterized by the formation and subsequent contraction of diseased cords in the palmar fascia, leading to fixed-flexion deformities in the metacarpophalangeal (MCP), proximal interphalangeal (PIP), and distal interphalangeal joints. Although PIP joints are less frequently affected than MCP joints, they tend to be more disabling, as many routine daily activities are impaired when these joints are contracted. 1 Research has shown that improvements in PIP joint contractures correlate positively with improved hand function.1,2 Proximal interphalangeal joint contractures are also more challenging to treat with corrective surgery or minimally invasive procedures such as percutaneous needle fasciotomy and collagenase Clostridium histolyticum injections.1,3
Current literature in the field has shown that surgeons often set a lower threshold for operating on PIP joint contractures compared with MCP joint contractures with many opting to intervene when contractures reach 20°. 4 However, the severity staging of PIP contractures is not clearly defined, with many surgeons relying on the “table top test” as a determinant tool, complicating diagnosis and treatment planning. 4 There is a noticeable gap in research exploring how the severity of PIP contractures specifically correlates with surgical outcomes. The persistent challenge of correcting PIP contractures and their significant impact on hand function underscores the need for improved understanding and management strategies. Assessing treatment success for PIP contractures extends beyond clinical measures to include patient-reported outcome measures (PROMs) such as Patient-Reported Outcomes Measurement Information System (PROMIS), which provide valuable insights into how patients perceive their hand function and how they feel. Integrating PROMs into clinical assessments enhances our understanding of treatment efficacy and patient perception of recovery.
The objectives of this study are to assess both patient-reported and objective clinical outcomes of surgical interventions for severe PIP contractures in Dupuytren disease, and to determine whether objective clinical outcomes correlate with PROMs following surgery. We hypothesize that although surgical procedures will result in substantial improvements in contracture correction, these improvements may not lead to significant enhancements in hand function or overall quality of life, as reflected by a lack of correlation with improved PROMIS scores. The study aims to provide insights into the effectiveness of surgical interventions for severe PIP contractures and their overall impact on patient outcomes.
Methods
Study Design
This study is a retrospective chart review of consecutive patients who underwent surgical correction for severe PIP contractures at a single academic medical center and was approved by our institutional review board (No. s23-01127).
Inclusion Criteria
Participants were selected through a chart review using the International Classification for Diseases, 10th Revision code M72.0 (palmar fascial fibromatosis), and Current Procedural Terminology codes (26040, 26045, 26121, 26123, 26125, and 26525) for fasciectomy, fasciotomy, or capsulotomy procedures, from database inception until 2024. Patients included had a diagnosis of Dupuytren disease with severe PIP joint contractures. Each finger with a qualifying PIP contracture was considered separately if multiple fingers met the inclusion criteria.
Exclusion Criteria
Patients with contractures attributed to other diagnoses such as posttraumatic contractures or contractures resulting from previous surgeries without the diagnosis of Dupuytren disease, were excluded.
Treatment Procedure
Surgical procedures for PIP contracture correction were performed based on clinical assessment and included fasciectomy, fasciotomy, or capsulotomy. The primary aim of the surgery was to achieve maximum contracture correction and restore functional range of motion (ROM). The procedures were performed under local, regional block, or general anesthesia.
Postoperatively, patients began immediate active ROM protocols and were provided with night splints for 2 weeks in an intrinsic-plus posture. Formal hand therapy was recommended if patients experienced stiffness or limited ROM.
Outcome Measures
The primary outcomes measured were the ROM and PROMs using the PROMIS data. Range of motion was assessed using a goniometer with data used from 3 time points: the preoperative visit, the immediate postoperative period, and the final follow-up visit.
The PROMIS is a validated system designed to assess various health domains relevant to the patient’s quality of life, including physical, mental, and social health. In this study, the specific PROMIS domains evaluated were pain intensity, daily activity interference, and upper extremity function, as these were the domains available in the collected data. The pain intensity domain measures the patient’s perception of pain severity over a specific time frame (typically the past 7 days), using a scale from 1 (no pain) to 10 (worst imaginable pain). The daily activity interference domain evaluates the extent to which pain and hand dysfunction affect a patient’s ability to perform everyday tasks such as personal care, household activities, or work-related duties, with higher scores indicating greater impairment. The upper extremity function domain assesses the patient’s ability to carry out tasks requiring hand, wrist, or arm function such as opening jars, writing, or lifting objects, with higher scores reflecting better functional performance. 5
The PROMIS data were collected during clinic visits at multiple time points, including the preoperative visit, the immediate postoperative period, and final follow-up, and these scores were used to evaluate patient-perceived outcomes following surgical correction of PIP contractures. Secondary outcomes included documenting any complications such as infection, postsurgical deformity, fracture, nerve injury, or the need for repeat surgery.
Statistical Analysis
Descriptive statistics were used to summarize the demographic and clinical characteristics of the study cohort, including means, standard deviations, and percentages. Comparisons of contracture degrees and PROMIS scores were performed across different severity groups and time points.
Contracture Degrees
Contracture degrees were analyzed for each severity group at preoperative, immediately postoperative, and final follow-up time points. The mean contracture degrees were compared within each group using paired t tests to determine the statistical significance of changes over time. Distribution of digits among the severity classifications preoperatively and at final follow-up were compared using a χ2 test. For between-group comparisons from preoperative to final follow-up, an unpaired t test was used to determine the statistical significance between the severity of groups 1-2 and groups 3-4. In addition, for the between-group comparison of contracture, 1-way analysis of variance (ANOVA) was used to assess the differences among severity groups 1 to 3, excluding group 4 due to the small sample size. Post hoc pairwise comparisons were conducted using Tukey Honestly Significant Difference (HSD) test when significant differences were found.
PROMIS Scores
The PROMIS scores for pain intensity, daily activity interference, and upper extremity function were evaluated across different severity groups. Preoperative, immediately postoperative, and final follow-up scores were compared using paired t tests to detect significant changes within each group. For between-group comparisons from preoperative to final follow-up, an unpaired t test was used to determine the statistical significance between severity groups 1-2 and groups 3-4. In addition, for the between-group comparison of contracture, 1-way ANOVA was used to assess the differences among severity groups 1 to 3, excluding group 4 due to the small sample size. Post hoc pairwise comparisons were conducted using Tukey HSD test when significant differences were found.
Statistical Significance
A P value of less than .05 was considered statistically significant for all analyses. For changes in contracture degrees, P values were reported as exact values for clarity. The PROMIS score changes were assessed with near-significant thresholds (P values close to .05) reported to indicate trends.
Time to Follow-up
The average time from surgery to final follow-up was compared among severity groups using 1-way ANOVA. If significant findings were observed, post hoc analyses were conducted to determine specific group differences.
Statistical analyses were performed using R Studio, and results are presented as means ± standard deviations unless otherwise stated.
Results
A total of 60 digits in 48 patients (37 men and 11 women, mean age of 65.2 ± 9.8 years) were included in the final analysis (Table 1). Most patients had the disease affecting more than 1 digit (35, 72.92%). The most common affected digit was the small finger (35/60, 58.33%), followed by the ring finger (18/60, 30%) and the middle finger (7/60, 11.67%). The affected digits were evenly distributed between the hands, with 50% from the right hand and 50% from the left. In addition, 48.33% (29/60) of the digits affected the dominant hand, with 30% (18/60) affecting the nondominant hand and another 21.67% (13/60) not having a listed hand dominance. Only 3 digits (5%) had received previous surgical intervention, with 2 being a previous contracture release and 1 being a needle aponeurotomy. Among the digits in our study, the procedures performed included capsulotomy (1/60, 1.67%), capsulectomy (2/60, 3.33%), fasciotomy (27/60, 45%), fasciectomy (29/60, 48.33%), and digit widget placement (8/60, 13.33%). No operative complications or reoperations were noted among the patients.
Demographic and Condition Parameters.
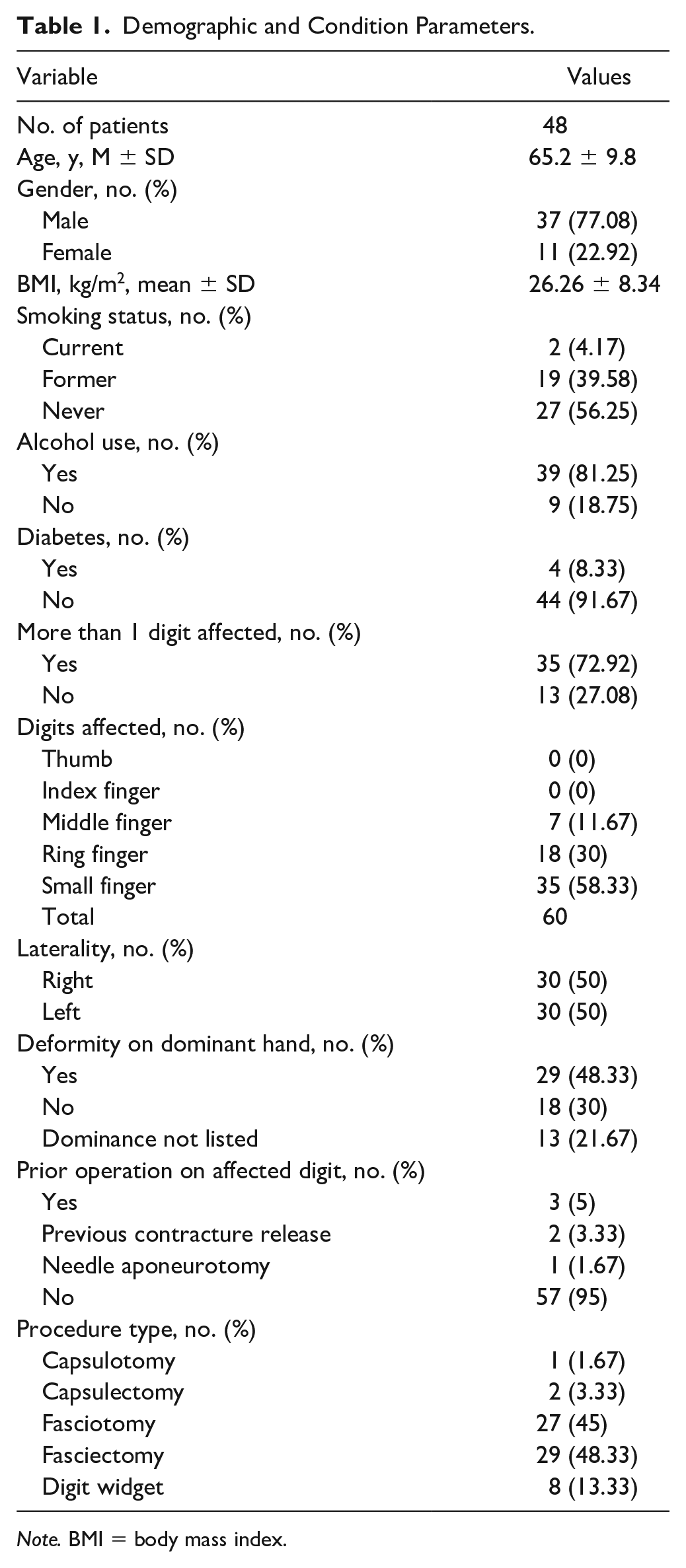
Note. BMI = body mass index.
Digits were categorized into severity groups according to the degree of their preoperative contractures. Group 1 (<29°, n = 13) began preoperatively at 19.54° ± 4.86°, decreased to 0.38° ± 1.39° immediately postoperatively (P < .001), and increased to 4.92° ± 7.16° at the final follow-up (P = .05; Table 2; Figure 1). Group 2 (30°-59°, n = 21) began preoperatively at 44.48° ± 8.50°, decreased to 5.62° ± 8.05° immediately postoperatively (P < .001), and increased to 11.43° ± 13.23° at the final follow-up (P = .11). Group 3 (60°-89°, n = 21) began preoperatively at 69.76° ± 10.58°, decreased to 27.6° ± 20.89° immediately postoperatively (P < .001), and decreased to 25.90° ± 19.07° at the final follow-up (P = .63). Last, group 4 (>90°, n = 5) began preoperatively at 94° ± 4.18°, decreased to 40° ± 41.23° immediately postoperatively (P = .03), and decreased to 23° ± 12.04° at final follow-up (P = .40). From preoperative to final follow-up contracture, the groups demonstrated a 75.29% ± 38.65% (P < .001), 74.42% ± 28.97% (P < .001), 62.83% ± 27.96% (P < .001), and 75.52% ± 13.18% (P < .001) decrease in average contracture, respectively (Table 2). Overall, there was a significant change in the PIP joint severity from preoperative to final follow-up classification (P < .001). In addition, the groups’ average times from surgery to final follow-up were 71.92 ± 35.84, 121.81 ± 104.11, 176.38 ± 144.11, and 74.8 ± 44.5 days, respectively (P = .04), with a significant difference between groups 1 and 3 (P = .04).
Comparison of PIP Joint Contractures Preoperatively to Final Follow-up.
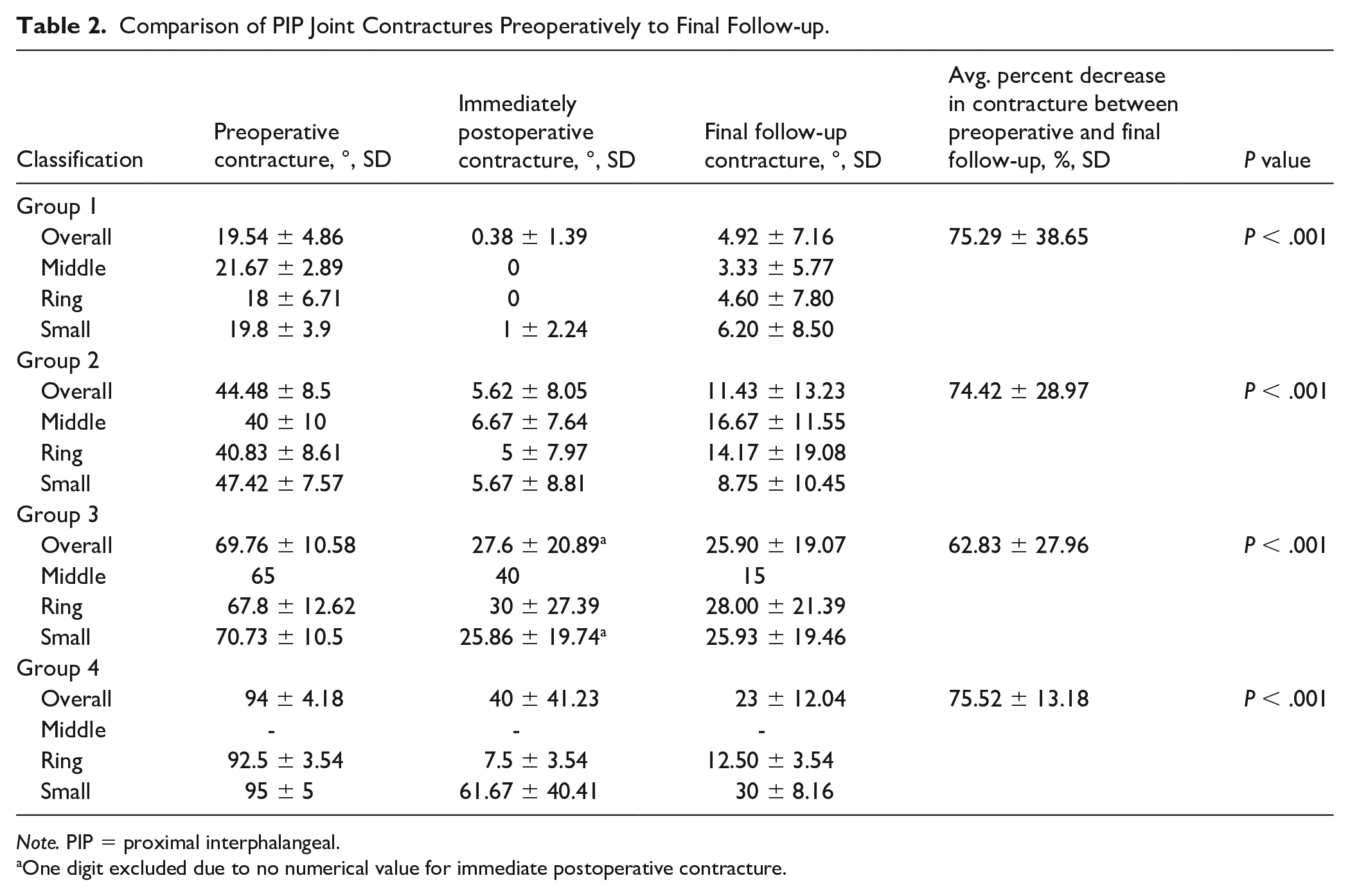
Note. PIP = proximal interphalangeal.
One digit excluded due to no numerical value for immediate postoperative contracture.
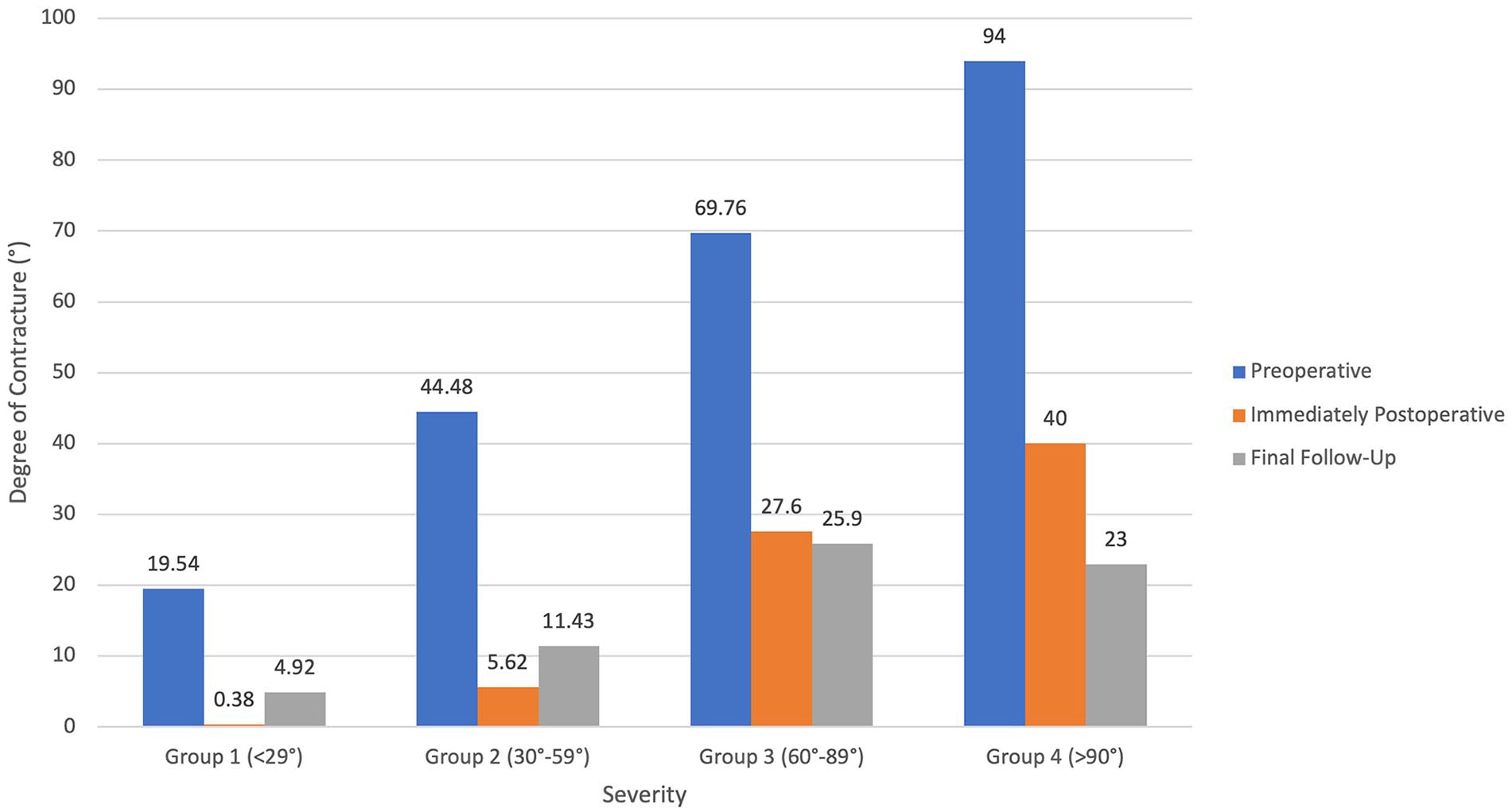
The average proximal interphalangeal joint contractures (°) in all 4 severity groups for before operation, immediately after operation, and final follow-up (y-axis: contracture degree [°]; x-axis: preoperative, immediately postoperative, and final follow-up in all 4 severity groups).
For pain intensity, there were no significant differences found between preoperative, immediately postoperative, or final follow-up PROMIS scores (Supplemental Table 1). However, group 4’s pain intensity from preoperatively at 37.68 ± 5.59 to final follow-up at 43.59 ± 8.46 (P = .06) trended to an increased score, although not statistically significant.
For daily activity interference, in groups 1 to 3, there were no significant differences found between preoperative, immediately postoperative, and final follow-up PROMIS scores (Table 3). For group 4, there was an increase in daily activity interference from 50.25 ± 2.52 preoperatively to 59 ± 4.36 immediately postoperatively (P = .04) with a decrease to 52.3 ± 8.71 at the final follow-up (P = .049). However, for group 4, there was also no significant difference overall between preoperative and final follow-up daily activity interference PROMIS scores.
Daily Activity Interference PROMIS Scores by Severity Classification.
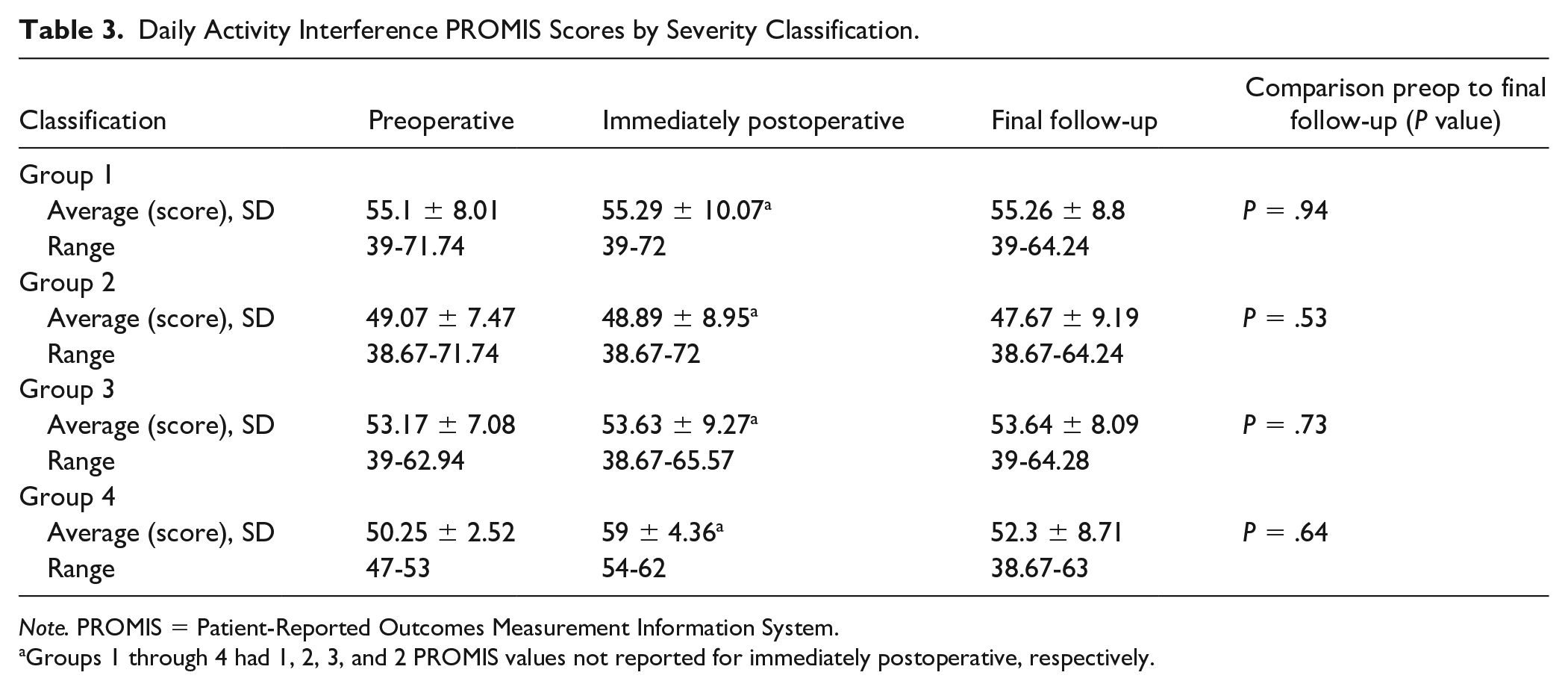
Note. PROMIS = Patient-Reported Outcomes Measurement Information System.
Groups 1 through 4 had 1, 2, 3, and 2 PROMIS values not reported for immediately postoperative, respectively.
For upper extremity function PROMIS scores, group 1 began at 39.98 ± 12.6 preoperatively, decreased to 34.24 ± 8.93 immediately postoperatively (P = .049), and increased to 42.68 ± 13.18 at final follow-up (P = .029; Supplemental Table 2). There was no significant difference in upper extremity function between preoperative and final follow-up for group 1. Group 2 began at 49.44 ± 9.98 preoperatively, decreased to 36.61 ± 11.2 immediately postoperatively (P < .001), and increased to 45.12 ± 12.92 at final follow-up (P = .03). Group 3 began at 44.53 ± 11.38 preoperatively, decreased to 32.87 ± 10.35 immediately postoperatively (P < .001), and increased to 38.58 ± 11.01 (P = .02). There was a significant decrease in upper extremity function between preoperative and final follow-up for group 3 (P = .02). For group 4, there was a decrease in upper extremity function from 53.72 ± 11.25 preoperatively to 40.39 ± 10.61 at final follow-up (P = .05).
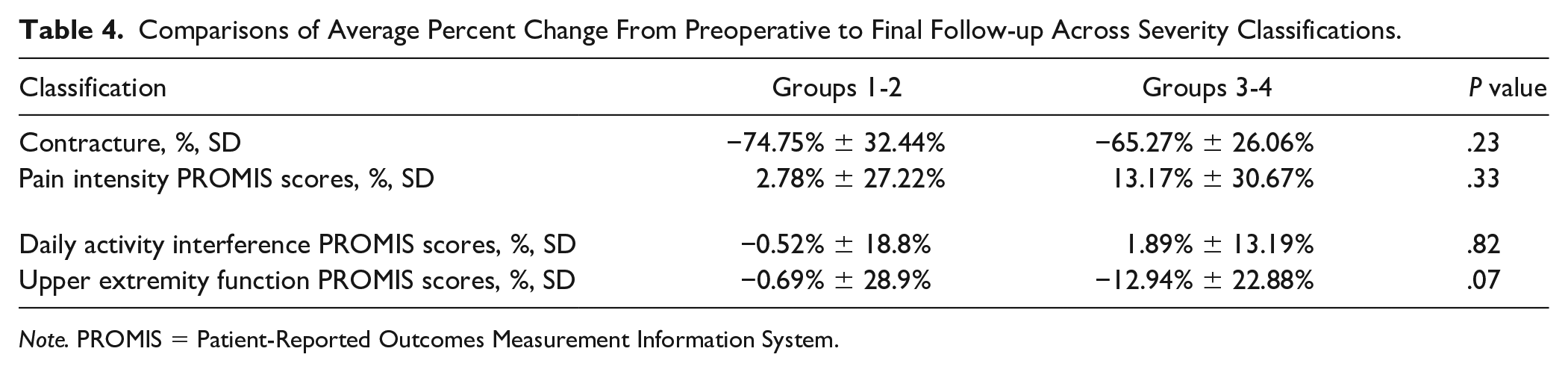
Severity groups 1 and 2 were combined for comparison with the combined groups 3 and 4 (Table 4). There were no significant differences found in the percentage change from preoperative to final follow-up for contracture (P = .23), pain intensity PROMIS scores (P = .33), or daily interference PROMIS scores (P = .82). There was a difference in percent change of upper extremity function PROMIS scores, although not statistically significant, from preoperative to final follow-up (P = .07) with groups 1 and 2 having a –0.69% ± 28.9% change and groups 3 and 4 having a –12.94% ± 22.88% change.
Comparisons of Average Percent Change From Preoperative to Final Follow-up Across Severity Classifications.
Note. PROMIS = Patient-Reported Outcomes Measurement Information System.
In addition, comparisons were conducted across groups 1 to 3 (Table 5). There was no significant difference found in the percentage change from preoperative to final follow-up for contracture (P = .40), pain intensity PROMIS scores (P = .40), or daily activity interference PROMIS scores between groups 1 and 3 (P = .90).
Comparisons of Average Percent Change From Preoperative to Final Follow-up Across Severity Groups 1 to 3.

Note. PROMIS = Patient-Reported Outcomes Measurement Information System.
Discussion
Severe PIP contractures in Dupuytren disease pose significant challenges in both surgical correction and long-term management. Although surgical intervention has proven effective for MCP contractures, PIP contractures are notoriously difficult to treat and have less predictable outcomes. 6 Given their impact on hand function, it is crucial to elucidate clinical measures and PROMs for this specific joint pathology. This study aimed to address this gap in the literature by providing data on objective contracture correction and patient-perceived outcomes through the PROMIS scoring system based on the severity of PIP contractures.
Our results demonstrated significant improvements in contracture correction across all severity groups, with an average reduction in contracture degrees of more than 60%. This underscores the effectiveness of surgical interventions in restoring ROM for patients with Dupuytren disease. Despite these objective improvements in contracture correction, the PROMs (PROMIS) did not consistently correlate with these clinical results. Surprisingly, the only significant change in PROMIS outcomes observed was in group 3 (60°-89°), which showed decreased upper extremity function at the final follow-up visit. The remaining analyses showed no statistically significant changes in PROMIS scores for pain intensity, daily activity interference, or upper extremity function between preoperative and final follow-up visits, nor when comparing them between severity groups. These unexpected findings raise the question of whether PROMIS is an adequate tool to assess patient function and experiences in the context of specific joint contractures such as severe PIP contractures. Although PROMIS is a standardized and validated system, it may not capture the nuances of hand function improvements as perceived by patients undergoing surgical correction of PIP contractures.
Previous studies have alluded to several factors that may influence surgical success such as preoperative deformity, intraoperative decisions, involvement of the small finger, and multiple ray involvement.6 -8 In fact, Donaldson et al noted that greater intraoperative correction at the PIP often leads to residual contractures within 6 months, which may explain the variability seen in patient outcomes. Despite the difficulty in achieving full correction, studies have generally shown that even partial reduction in deformity leads to improved hand function.2,9,10 Sinha et al 10 emphasized the negative correlation between the severity of preoperative deformity and hand dexterity, highlighting that any reduction in deformity should yield better function. However, other reports, such as those by Zyluk et al, 11 suggest that some patients report little change in function postoperatively, possibly due to long-standing adaptations to the deformity. This discrepancy highlights the importance of characterizing the effects of surgical intervention on both objective outcomes and patient-perceived function, as some patients may not experience the expected improvements despite successful contracture correction.
The wide range of available PROMs in orthopedic practice and research leads to confusion among providers regarding which tool is most suitable for specific patient populations. 12 In addition, understanding how to interpret these scores effectively to improve treatment recommendations can be challenging. A systematic review by Horn et al found that PROMIS measures varied across orthopedic surgery populations, with 37% of studies focusing on lower extremity conditions, followed by upper extremity (28%) and spine (19%). Despite the increasing popularity, they emphasize the importance of selecting PROMIS measures based on the most relevant constructs for each population and determining whether PROMIS tools are sufficient on their own or if traditional measures should be used to supplement them for more comprehensive assessments. 12 In line with this, despite the objective surgical success of our cohort in contracture correction, our study found a lack of alignment with the subjective outcomes, as seen by PROMIS scores for pain intensity, daily activity interference, and upper extremity function not showing consistent improvements at the final follow-up. Although the use of PROMIS scores has increased in clinical practice and orthopedic research over the past years, there has not been specific validation of this assessment tool for Dupuytren disease, especially in the context of PIP contractures. This lack of validation raises questions about its effectiveness in fully capturing the functional and subjective experiences of patients with these specific joint deformities. Nevertheless, this study’s findings align with the literature, where similar discrepancies between objective measures and PROMs have been observed. For instance, Jerosch-Herold et al 13 found that Disabilities of the Arm, Shoulder, and Hand (DASH) scores, another commonly used tool, did not always correlate with the severity of contractures, suggesting that subjective measurement tools may not fully capture the impact of the disease on hand function. This may be due to the specific nature of tasks assessed in these questionnaires, which may overlook the nuanced limitations experienced by patients with ulnar digit involvement. 13 Gilat et al 14 discussed the floor and ceiling effects in PROMs, which can reduce sensitivity, especially in patients at the extremes of health. Hence, PROMIS may not be sensitive enough to detect the intricate functional challenges faced by patients with severe PIP contractures, potentially leading to an underestimation of their recovery.
Surgical correction should remain a central treatment option when contractures exceed 20° to 30°. This threshold was associated with significant improvements in ROM and an absence of operative complications and reoperations, proving safe and effective. However, the disconnect between objective improvements and PROMIS scores highlights a critical consideration: Traditional clinical measures of success may not fully capture the patient’s perspective on functional recovery. The implications of these findings are critical for patient counseling. Surgeons must be cautious when setting expectations, as improvements in joint contracture may not always result in perceived functional recovery. This also highlights the need for further research into developing or refining PROMs better suited to assess the intricacies of hand function and specific challenges faced by patients with severe PIP contractures in Dupuytren disease. As current tools like PROMIS and DASH may not fully capture the patient experience, the development of more targeted assessment instruments could enhance both clinical decision-making and patient satisfaction in the future.
Future prospective studies could explore this hypothesis by assessing alternative tools such as the QuickDASH or Michigan Hand Outcomes Questionnaire alongside PROMIS to determine which measures better reflect patient recovery in hand function. In addition, investigating the psychosocial factors that may influence patient perceptions of recovery—such as pain, stiffness, or psychological adjustments to living with hand deformities—could provide valuable insights into the holistic experience of patients undergoing treatment for severe PIP contractures. Long-term studies are also needed to determine whether the observed improvements in contracture correction and patient-perceived outcomes are sustained over time. In particular, prospective studies collecting arc of motion after surgery as an objective measurement to correlate with patient-perceived outcomes would be of interest. Such studies could inform postoperative care strategies, refine rehabilitation protocols, and help to clarify the best methods for integrating both objective and patient-reported outcomes into the treatment of Dupuytren disease.
Limitations
This study has several limitations that must be acknowledged. First, as a retrospective chart review, the study is inherently subject to selection bias, as only patients who underwent surgical correction at a single academic center were included, limiting generalizability. In addition, the retrospective design limits our ability to control for confounding variables such as differences in surgical technique, patient adherence to rehabilitation protocols, and variations in disease chronicity and severity. As factors like stiffness and intrinsic values like self-motivation/compliance with hand exercises, among others, that can impact patient-reported outcomes were not assessed thoroughly in this study, it is unclear what the driver for our findings of decreased PROMIS scores in some groups compared with preoperative status were. However, the questioning of PROMIS as the appropriate assessment tool for this pathology remains a possible main contributor. Another limitation is the variability in follow-up duration among patients. Shorter follow-up times may underestimate late complications or the potential for contracture recurrence.
Conclusion
Objective clinical outcomes, particularly the improvement in ROM, were substantial across all severity groups, reinforcing the importance of surgical correction in managing severe PIP contractures. However, the lack of corresponding improvements in patient-reported outcomes, as measured by PROMIS scores, raises important questions about the utility of this tool for evaluating the intricacies of hand function and pain in the context of specific joint contractures. This study calls for the development of complementary patient-reported measures that are more sensitive to the particular functional challenges associated with joint-related hand deformities. By integrating both objective and appropriate patient-reported outcomes more effectively, future management strategies can be better tailored to address both the physical and psychological aspects of recovery, ultimately improving health care outcomes and the overall quality of care for patients with severe PIP contractures.
Supplemental Material
sj-docx-1-han-10.1177_15589447251357043 – Supplemental material for Objective Improvements, Subjective Uncertainty: Surgical Outcomes and the Role of PROMIS in Severe PIP Contractures
Supplemental material, sj-docx-1-han-10.1177_15589447251357043 for Objective Improvements, Subjective Uncertainty: Surgical Outcomes and the Role of PROMIS in Severe PIP Contractures by Gerardo E. Sanchez-Navarro, Archie Spindler, Victoria Comunale, Nadia Linton, Sophia Jacobi and Jacques H. Hacquebord in HAND
Supplemental Material
sj-docx-2-han-10.1177_15589447251357043 – Supplemental material for Objective Improvements, Subjective Uncertainty: Surgical Outcomes and the Role of PROMIS in Severe PIP Contractures
Supplemental material, sj-docx-2-han-10.1177_15589447251357043 for Objective Improvements, Subjective Uncertainty: Surgical Outcomes and the Role of PROMIS in Severe PIP Contractures by Gerardo E. Sanchez-Navarro, Archie Spindler, Victoria Comunale, Nadia Linton, Sophia Jacobi and Jacques H. Hacquebord in HAND
Footnotes
Ethical Review Committee Statement
This study was approved by the NYU School of Medicine’s Institutional Review Board (s23-01127).
Statement of Human and Animal Rights
This study was approved by the NYU Langone Health Institutional Review Board (IRB) Research Ethics Committee (approval no. s23-01127) on June 24, 2024.
Statement of Informed Consent
Informed consent was not required for this manuscript as it involved a retrospective analysis of anonymized data from a database. The study utilized preexisting data and did not involve direct interaction with human subjects, thus exempting it from the requirement of informed consent.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
ORCID iDs
Supplemental material is available in the online version of the article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.