
Abstract
Background:
The scaphoid height-to-length (H/L) ratio assesses reduction quality, with lower values indicating better anatomic restoration and reduced malunion risk. We hypothesized that dorsal percutaneous fixation of acute, unstable distal oblique fractures yields a lower postoperative H/L ratio compared with volar fixation.
Methods:
We retrospectively reviewed all Herbert B1 fractures treated with percutaneous screw fixation at a single, tertiary referral center over 10 years. Dorsal and volar approaches followed standardized protocols, with guidewire placement under fluoroscopy and headless compression screw fixation. Postoperative computed tomography (CT) assessed the H/L ratio, intrascaphoid angle (ISA), and dorsal cortical angle (DCA), reformatted along the long axis of the scaphoid. Demographics, injury/operative characteristics, CT-based metrics, and clinical outcomes were compared between approaches.
Results:
A total of 18 patients met inclusion criteria (dorsal n = 10, volar n = 8), with an average follow-up of 7.3 months. The cohorts did not significantly differ in demographic, injury, or operative covariates. Computed tomography assessment showed similar ISA and DCA, but a lower H/L ratio in the dorsal approach cohort (0.64 vs 0.70, P = .040). While functional outcomes were mostly comparable, dorsal approach patients reported lower Disability of the Arm, Shoulder, and Hand scores at final follow-up (17.7 vs 45.5, P = .019). Two of the 18 patients developed nonunion; both were treated via a dorsal approach.
Conclusions:
A dorsal approach may achieve more anatomic reduction in percutaneous screw fixation of distal oblique scaphoid fractures, though it remains unclear whether the approach has any meaningful, relative influence on functional outcome and bone union.
Keywords
Introduction
Scaphoid fractures account for over half of all carpal fractures, predominantly affecting younger, active individuals.1,2 In high-energy mechanisms, such as falls onto an outstretched hand (FOOSH), the scaphoid bears much of the axial load transferred through the wrist, making it particularly susceptible to fracture. 3 The scaphoid exhibits unique anatomy, as the majority of the bone’s surface is covered by cartilage, and its vascular contribution is primarily retrograde from the radial artery entering at the dorsal capsular ridge. 4 These factors render the scaphoid particularly vulnerable to nonunion and avascular necrosis (AVN) after fracture. Given this structural complexity, recent literature reflects a growing interest in the use of objective imaging parameters in the evaluation of scaphoid fracture fixation. The sagittal height-to-length (H/L) ratio of the scaphoid, the lateral intrascaphoid angle (ISA), and the dorsal cortical angle (DCA) offer quantitative assessment of fracture alignment and reduction. 5 Prior work has demonstrated that H/L ratios derived from sagittal computed tomography (CT) scans reliably reflect quality of reduction, with lower ratios associated with a reduced risk of malunion. 6
Historically, most scaphoid fractures have been treated nonoperatively using cast immobilization.7,8 The development of the compression screw by Herbert and Fisher in 1984, along with Streli’s innovation of percutaneous fixation, marked a shift toward operative intervention, driven by efforts to improve union rates and optimize functional outcomes.9,10 Since its development, the Herbert screw has evolved into various forms of cannulated, headless compression screws that have allowed for the refinement of percutaneous fixation. Both dorsal and volar percutaneous fixation techniques for scaphoid fractures have been described in the literature, with studies reporting similarly minimal complication rates between the two approaches.11,12 With the dorsal approach, it is believed that introducing the screw into the narrower proximal pole will provide easier fixation in the central aspect of the scaphoid. This results in a screw placed more parallel to the long axis of the scaphoid and more orthogonal to the fracture line.2,11 The volar approach, however, is thought to be particularly well-suited for distal fractures. This approach permits entry closer to the fracture line and easy reduction in extension, reducing tendency for humpback deformity. 13 The complexity of Herbert B1 fractures (ie, limited bone stock, fragment orientation, proximity to the articular surface) presents significant challenge in achieving proper screw alignment and fixation stability, making approach selection an important consideration.14,15 It remains unclear whether one approach offers any particular benefit over the other.
This study compares the dorsal and volar approach to percutaneous fixation in Herbert B1 fractures. We hypothesized that the dorsal approach would result in a lower postoperative H/L ratio on CT compared with the volar approach. Secondarily, we hypothesized that the dorsal approach would be associated with superior clinical and patient-reported outcomes.
Materials and Methods
Study Design
We retrospectively reviewed all patients ≥18 years of age who underwent percutaneous fixation of Herbert B1 scaphoid fractures over a 10-year period at a large, academic tertiary referral center. Patients with scaphoid fractures were identified with International Classification of Diseases, 9th and 10th Revision codes (814.01, S62.0X). Radiographs were screened to select for those with distal oblique fracture patterns. A single rater evaluated preoperative radiographs to determine degree of instability. Only unstable fractures were included, defined by the presence of any of the following characteristics: displacement >1 mm, dorsal intercalated segment instability (DISI) pattern, comminution, or ISA > 35°. Any patients with concomitant proximal pole involvement or associated fracture of the distal radius or other carpal bones were excluded. 16 Remaining patients were isolated by Current Procedural Terminology code 25628, and operative notes were manually reviewed to select for those who underwent primary percutaneous fixation within 6 weeks of initial injury. All patients meeting these inclusion criteria had record of postoperative CT imaging and completion of recommended follow-up; follow-up duration requirements varied between provider from 3 to 12 months. This population comprised the final study cohort.
Data were collected via manual chart review. Demographic data included age at time of injury, sex, and hand dominance. Injury characteristic data included injury date, laterality, mechanism, incidence of polytrauma, prior closed treatment, and time to surgery. As displacement, significant volar angulation (humpback deformity), and comminution are among the strongest predictors of poor union and functional outcome, 17 presence of any of these features on preoperative imaging (CT or radiograph) was also documented. Operative data included approach (dorsal/volar), attending surgeon, number of screws, use of temporary derotational Kirschner wires (K-wires), and tourniquet time. Key anatomic measurements were evaluated via postoperative CT assessment. Secondary clinical outcomes included complications (nonunion, hardware removal, and AVN), time to splint removal, time to union, time to return to full activity, Visual Analog Scale (VAS) pain score, Disability of the Arm, Shoulder, and Hand (DASH) score, Single Assessment Numeric Evaluation (SANE) score, and range of maximal active wrist flexion/extension. Postoperative imaging was used to determine union status. Standard protocol included radiographs at 6 weeks and CT at 3 months postoperatively, although there was variation based on the date of patient visits. Union was defined as visible trabecular continuity across the fracture line on radiographs or >50% osseous bridging on CT.18,19 Patients without union on CT were evaluated with serial radiographs. Nonunion was defined as persistent fracture lucency without interval healing at >12 months postoperatively. 19 Range of motion (ROM) data were measured with a goniometer. Patient-reported outcome measures and ROM data were collected from final follow-up visits.
Surgical Technique
Selection of the surgical approach was determined based on surgeon preference, fracture pattern, and perceived stability. In some cases, both dorsal and volar exposure were evaluated intraoperatively to visualize the scaphoid in both flexion and extension prior to final approach selection. All percutaneous fixations were performed under appropriate anesthesia using a standardized protocol. The dorsal approach began with a small incision just ulnar to Lister’s tubercle under wrist flexion. Blunt dissection was carried through the soft tissue to the extensor retinaculum, which was incised in line with the skin incision. The extensor pollicis longus was protected. The proximal pole of the scaphoid was exposed. The volar approach began with a small longitudinal incision radial to the flexor carpi radialis at the thenar base over the palpable distal pole of the scaphoid; the wrist was held in extension and longitudinal thumb traction was applied. Blunt dissection was carried through the soft tissue to the level of the volar scaphotrapeziotrapezoidal (STT) joint capsule. Following scaphoid exposure, subsequent operative steps were similar for both approaches. With a reduced fracture, 1.1 to 1.2 mm guidewire(s) were advanced under fluoroscopic guidance dorsally/volarly into the scaphoid, with optional provisional fixation using derotational K-wires (Figure 1a-c). One or more cannulated headless compression screws were inserted over the guidewire to achieve stable fracture fixation (Figure 1d). Wounds were irrigated and closed. Thumb spica splints were applied postoperatively, with the duration of splinting subject to provider preference.
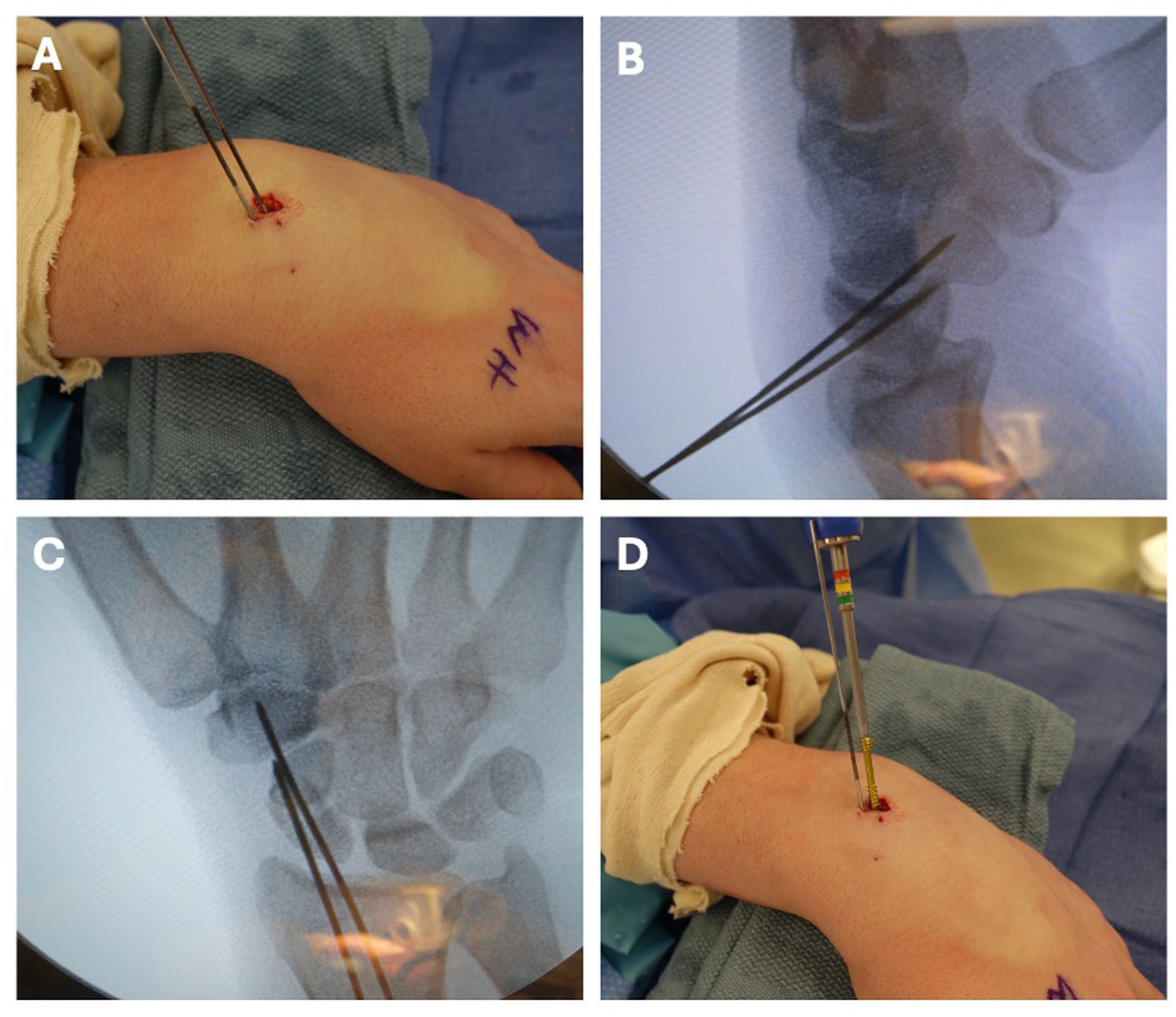
Dorsal percutaneous fixation of distal oblique scaphoid fracture.
Postoperative CT Evaluation
Postoperative sagittal CT scans were reconstructed along the long axis of the scaphoid within the institutional Picture Archiving and Communication System (PACS) software. A central image was selected, where the scaphoid was the longest. The H/L ratio, lateral ISA, and DCA were measured by a single rater within PACS. 5 Length was measured as the distance between the most proximal and distal aspects of the scaphoid, along the anterior facet. Height was measured as the maximum orthogonal distance from the “length” vector to the dorsal surface (Figure 2a). The lateral ISA was calculated by drawing perpendicular lines through the proximal and distal articulating surfaces and measuring the acute angle between these intersecting lines (Figure 2b). The DCA was calculated by drawing tangential lines along two flattest portions of the dorsal aspect of the scaphoid and measuring the obtuse angle between these intersecting lines (Figure 2c).
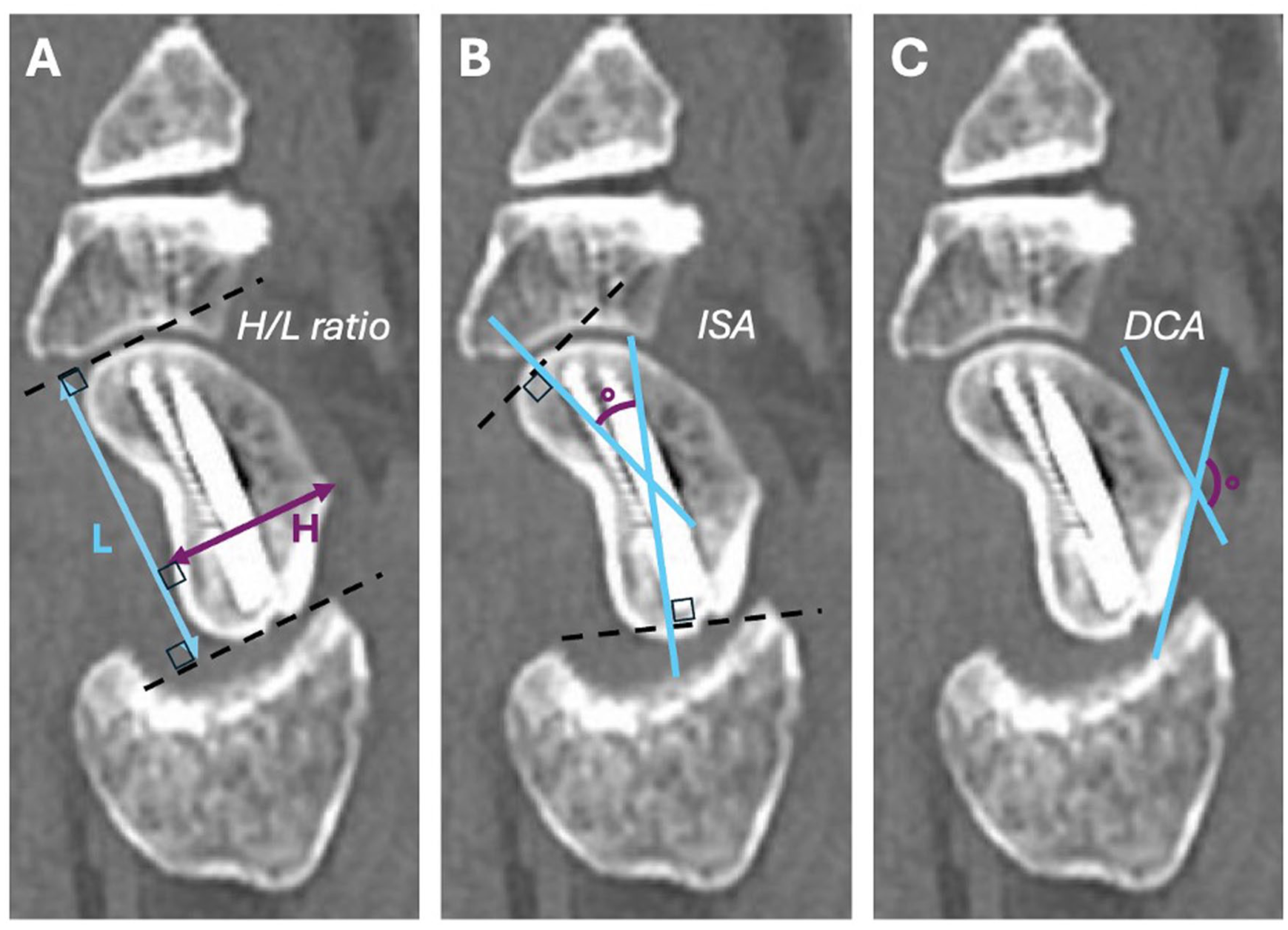
Postoperative computed tomography (CT) measurements along the long axis of the left scaphoid for a representative patient who underwent double-screw percutaneous fixation via a dorsal approach.
Statistical Analysis
All statistical analyses and data visualization were completed in MATLAB (R2024b, The MathWorks Inc., Natick, Massachusetts). Continuous variables were described using mean values (± standard deviation). Categorical variables were described using proportions. Continuous variables were compared between cohorts via Wilcoxon rank-sum tests. Categorical variables were compared via Fisher’s exact tests. To account for nonunion, time to union data were characterized by medians (interquartile range [IQR]) and compared via Cox proportional hazard models, with results presented a hazard ratio (HR) and 95% confidence interval (CI) for dorsal versus approach cohorts. This model analyses union as the final end point, thus values < 1 indicate later union with the dorsal approach, while values >1 indicate earlier union. All tests were two-tailed with a significance threshold of P < .05. The H/L ratio was defined a priori as the primary outcome, as a sensitive marker of fracture reduction quality wherein differences might be detected with limited cohort sizes. 6 Cohort characteristics and secondary outcomes were analyzed with reported P-values but interpreted in context, given the increased risk of type I error with multiple outcome testing and insufficient power to detect clinically meaningful differences in dichotomous outcome measures.
Results
Among the 18 patients with Herbert B1 fractures meeting final criteria for study inclusion, 10 underwent dorsal percutaneous fixation, while 8 underwent volar percutaneous fixation. The dorsal approach cohort exhibited a mean follow up of 8.4 ± 7.8 months, similar to the volar approach cohort (5.9 ± 6.0 months). Cohorts did not significantly differ in key demographics or injury characteristics (Table 1). Four attending surgeons comprised this study. Approach distribution did not vary by surgeon. The proportion of fractures with preoperative displacement and humpback deformity were similar between cohorts. There was a higher frequency of mild comminution about the fracture line in the volar approach cohort (3/8 vs 0/10), though this difference was not statistically significant. Double-screw fixation rate and tourniquet time were similar between cohorts. Temporary derotational K-wires were used more frequently in the dorsal approach cohort (6/10 vs 1/8), though this difference was not statistically significant.
Demographics, Injury Characteristics, and Operative Details of Dorsal and Volar Approach Cohorts.
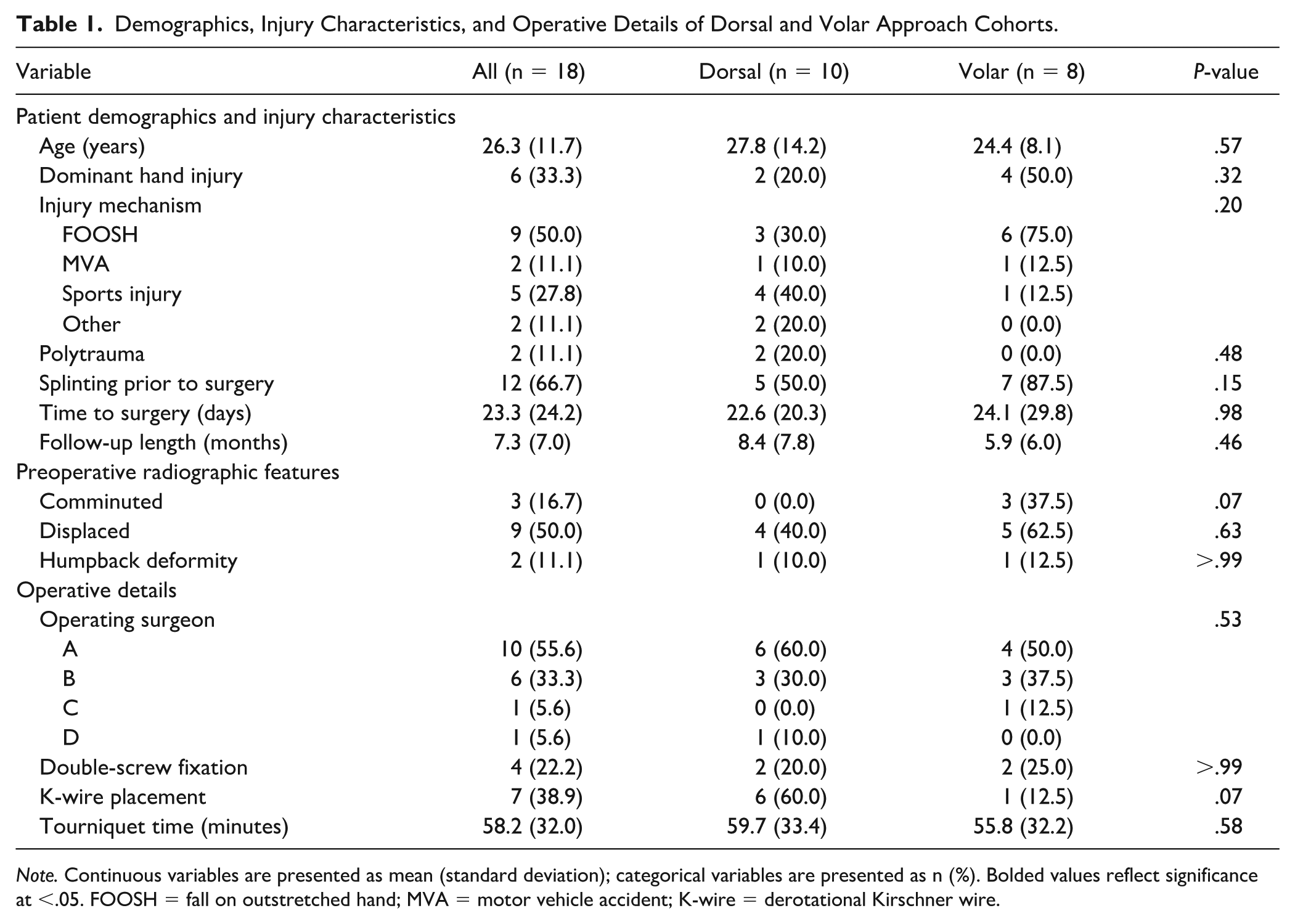
Note. Continuous variables are presented as mean (standard deviation); categorical variables are presented as n (%). Bolded values reflect significance at <.05. FOOSH = fall on outstretched hand; MVA = motor vehicle accident; K-wire = derotational Kirschner wire.
Postoperative CT measurements were collected at an average of 105 ± 36 days following surgery. Time to CT imaging was similar between cohorts (Table 2). Lateral ISA and DCA did not significantly differ between cohorts. The dorsal approach cohort exhibited a lower H/L ratio than the volar approach cohort (0.64 vs 0.70, P = .040) on postoperative CT (Figure 3).
Postoperative CT Evaluation Metrics for Dorsal and Volar Approach Cohorts.
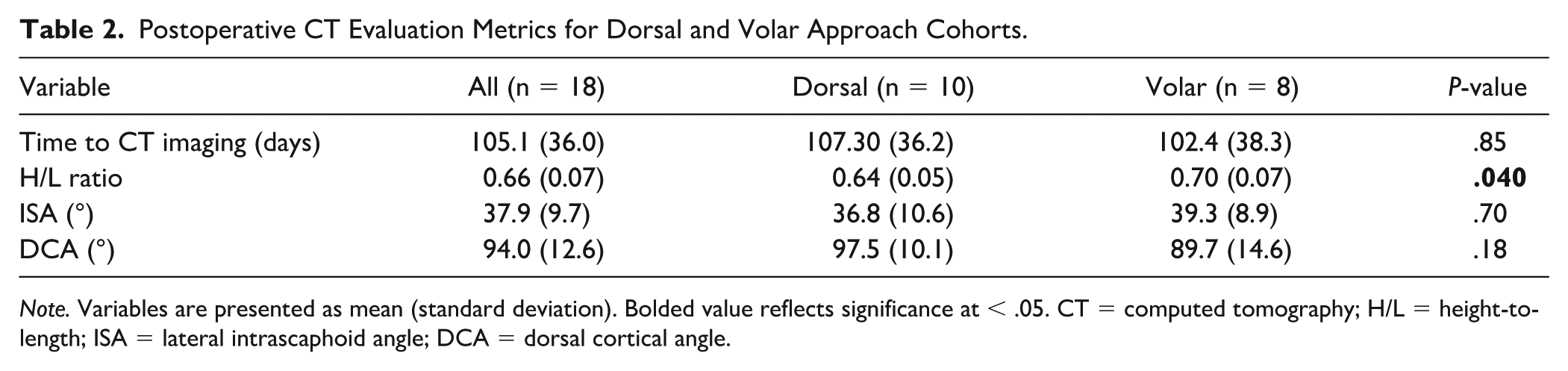
Note. Variables are presented as mean (standard deviation). Bolded value reflects significance at < .05. CT = computed tomography; H/L = height-to-length; ISA = lateral intrascaphoid angle; DCA = dorsal cortical angle.

Postoperative computer tomography (CT) assessment of dorsal and volar approaches. Key anatomic measurements (H/L ratio, ISA, DCA), in the plane of the long axis of the scaphoid, are plotted for each cohort.
Clinical outcomes were compared across cohorts (Table 3). There were 2 cases of nonunion among the 18 included patients. Both of these patients underwent percutaneous fixation via a dorsal approach (2/10). Survival analysis demonstrated a hazard ratio of 0.62 (95% CI [0.24-1.92], P = .47), indicating a statistically insignificant lower rate of union over time for dorsal versus volar approach cohorts. Among those who achieved union by final follow-up, the median time to union did not differ by approach. One patient in the volar approach cohort underwent hardware removal. Time to splint removal and time to return to full activity did not significantly differ by approach. Patient-reported outcome measures and ROM outcomes were collected at final follow-up. The dorsal approach cohort exhibited a lower mean DASH score compared with the volar cohort (17.7 vs 45.5, P = .019), indicating a lower reported functional disability. Although a higher mean SANE score (indicating greater function relative to baseline) was observed for the dorsal cohort (79.8 vs 61.0, P = .33), this result was not significant. Pain scores (VAS) and wrist flexion/extension ROM did not significantly differ by approach.
Clinical Outcomes of Dorsal and Volar Approach Cohorts.
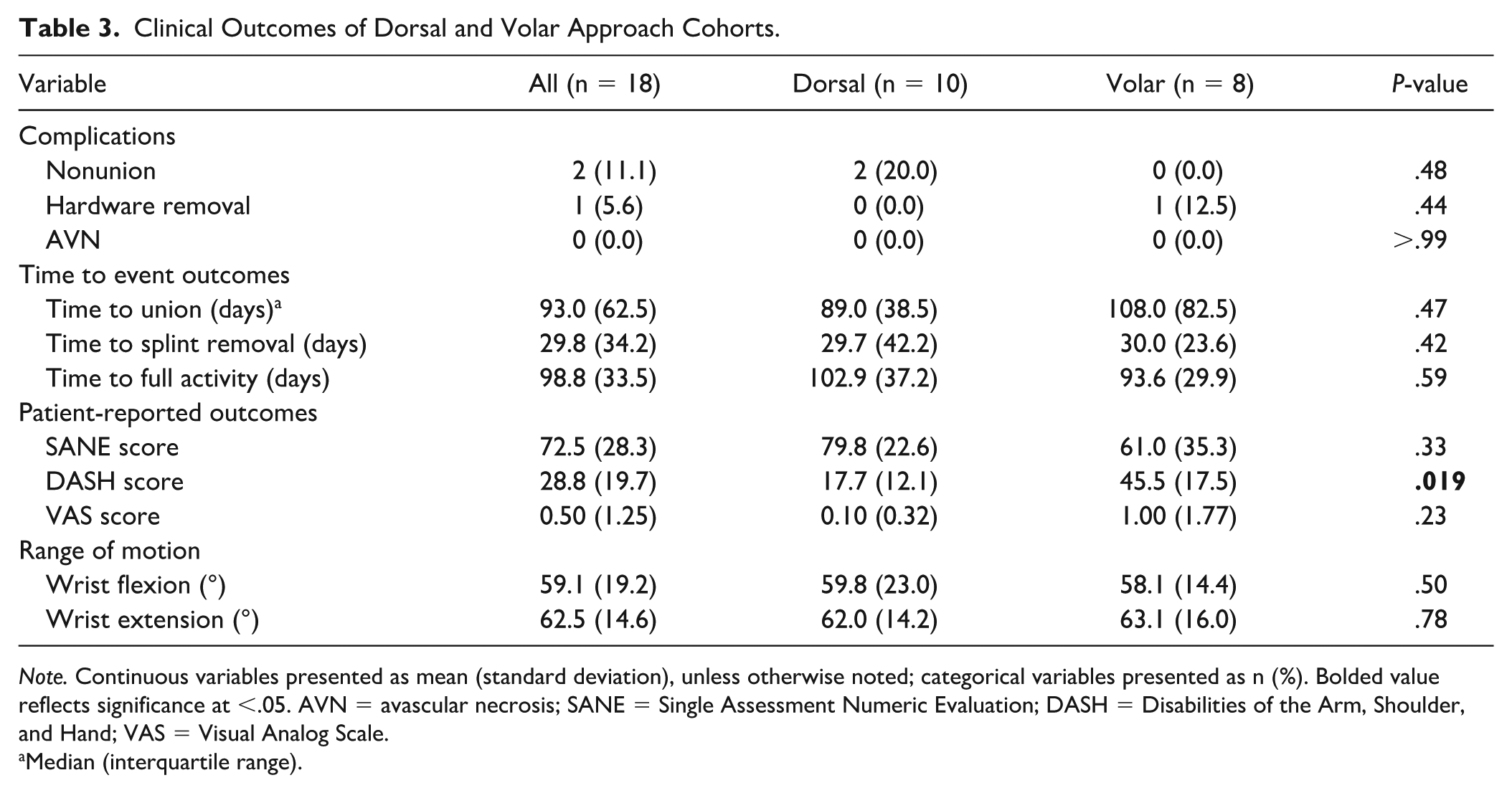
Note. Continuous variables presented as mean (standard deviation), unless otherwise noted; categorical variables presented as n (%). Bolded value reflects significance at <.05. AVN = avascular necrosis; SANE = Single Assessment Numeric Evaluation; DASH = Disabilities of the Arm, Shoulder, and Hand; VAS = Visual Analog Scale.
Median (interquartile range).
Discussion
Unstable fractures of the scaphoid are prone to nonunion, often warranting timely surgical fixation to ensure optimal healing.17,20 While fixation is widely regarded as the preferred treatment for Herbert B1 fractures, 2 the choice of surgical approach remains largely based on surgeon preference, as there exists limited literature guiding decision-making. 12 In this retrospective cohort study of 18 patients with Herbert B1 fractures treated with percutaneous fixation, we found that the dorsal approach provided superior anatomic alignment along the scaphoid’s longitudinal axis compared with the volar approach. However, aside from better DASH scores, improved anatomic alignment did not appear to translate to meaningful improvements in clinical outcomes. Patients in the dorsal approach cohort exhibited similar functional outcome with a higher observed incidence of scaphoid nonunion.
While a dorsal approach is preferred for proximal pole fractures, either approach can be used for fractures of the distal third and waist of the scaphoid. Jeon et al 11 analyzed radiograph-based metrics following percutaneous fixation of Herbert B2 (waist) fractures, finding that dorsal fixation enables more favorable screw positioning. Authors did not identify any difference regarding functional outcome and bone union. Owing to the rarity of Herbert B1 fracture patterns, comparative studies remain limited to cadaveric models. In a study including 12 cadavers, Soubeyrand et al 21 noted equivalently optimal screw placement with either approach for Herbert B2 fractures but found that the dorsal approach led to better screw placement for Herbert B1 fractures.
Our findings align with these prior studies, demonstrating that the dorsal approach to percutaneous fixation of Herbert B1 fractures results in a significantly lower H/L ratio compared with the volar approach, indicating more accurate anatomic alignment along the scaphoid’s long axis. The H/L ratio is a reproducible and validated measure of scaphoid alignment.5,6 A recent study by ten Berg et al 6 established normative values for scaphoid H/L ratios in uninjured wrists; authors reported a mean H/L ratio of 0.61, ranging from 0.54 to 0.69. We observed a mean H/L ratio of 0.64 following dorsal percutaneous fixation, approaching that of unfractured scaphoids. The mean H/L ratio in the volar approach exceeded the upper limit of normal values. In addition to a lower H/L ratio, a narrower ISA and wider DCA have been associated with superior fracture alignment.5,22 These measures, however, are more prone to intra- and inter-rater variation. 5 Although we observed a narrower raw ISA and wider DCA with the dorsal approach, these results were not significant. The H/L ratio is largely a culmination of these two angles, with narrower ISAs contributing to reduced scaphoid height, and wider DCAs conferring a greater length along the longitudinal scaphoid axis. Thus, the H/L ratio may serve a more holistic measure of accurate anatomic alignment. 5
Union rates using either dorsal or volar percutaneous approaches in scaphoid waist fractures have been reported between 89% and 100%.11,23,24 In our cohort of distal oblique fractures, we noted an overall union rate of 89%. Although similar between approaches, the overall time to union in our cohort was longer that reported for acute scaphoid fractures. This is likely a result of our institutional imaging protocol, with latent detection of interval union on CT scans at 3 months postoperatively. Superior anatomical alignment via a dorsal approach did not appear to confer any benefit regarding bone union. In fact, both cases of nonunion were observed in the dorsal approach cohort. Although this risk was not found to be significant in our small patient series, it certainly challenges the notion that improved fracture alignment translates to any benefit regarding union.
Clinical and functional outcomes were comparable between cohorts, apart from a 28-point lower patient-reported DASH score at final follow-up among dorsal approach patients. This difference exceeds the threshold of minimal clinically important difference (MCID) in DASH scores for procedures on the forearm and hand (MCID = 10, 95% CI [5-15]), 25 indicating less disability of the affected wrist among the dorsal approach cohort. When evaluating functional outcomes, similar studies have found no difference between volar and dorsal percutaneous approaches in the treatment of acute scaphoid fractures.11,12 We found no significant difference between time to return to full activity, SANE scores, VAS scores, and range of motion outcomes between approaches. Our ability to detect significant differences in such clinical outcomes was likely limited by our small cohort size. For example, a 19% higher mean SANE among the dorsal approach cohort was not found to be significant. The single-item questionnaire is a validated measure of global hand function, exhibiting strong correlation with QuickDASH scores. 26 Although a hand-specific MCID has yet to be defined, this observed difference exceeds the MCID reported for improvement following shoulder arthroplasty. 27 Although the symptomology of scaphoid malunion remains debatable, 28 larger studies have shown that with a better reduction and more favorable screw placement, patients experience better clinical outcomes. Trumble et al 29 found that central screw placement resulted in a reduction of time to union. Dias et al 30 later expanded on this work with a randomized control trial (comparing nonoperative management vs early internal fixation), demonstrating that postoperative range of motion is associated with the degree of scaphoid alignment achieved during internal fixation of acute scaphoid fractures.
This study has several limitations worth noting. Most importantly, the small sample size and lack of power analysis limit our ability to decipher further differences between patient cohorts. Distal oblique fracture patterns are rare. Although our institution has a relatively high volume of percutaneous scaphoid fixation, Herbert B1 fractures comprise a minority of these cases. Although we did not find significant differences in terms of nonunion rates, SANE scores, and range of motion outcomes, it is possible that with a larger patient cohort, additional differences might have been appreciated. This study was designed to evaluate the primary outcome of H/L ratio, thus any significant differences (or lack thereof) in secondary outcomes should be interpreted cautiously. The nonparametric distribution of these data necessitated a conservative statistical approach, further restricting our ability to detect small- to moderate-sized differences in clinical outcomes. The retrospective nature of this study poses an additional limitation. We were unable to control for potential coding errors, introducing potential biases in cohort identification and reporting of outcomes data. Although we were able to collect patient-reported outcomes retrospectively, we lacked preoperative reference values, limiting the utility of these inherently patient-dependent metrics. Procedures were performed by multiple hand surgeons at our institution and cohorts exhibited variation in degree of preoperative fracture instability; differences in outcomes must be cautiously attributed to approach alone, as we cannot elucidate surgical approach as an independent modifier of CT-based metrics or secondary clinical outcomes. Although standardized operative protocols were followed for each approach, temporary derotational K-wires were used more frequently in the dorsal approach. It is certainly plausible that K-wire placement might have impacted CT-based metrics. We avoided multiple regression analyses to evaluate independent modifiers of outcome measures, as such a model with this small of a cohort would be unstable. Computed tomography measurements introduced an additional layer of bias. Although measurements were made by a single rater following a standardized approach, intra-rater variation may have confounded results.
Nonetheless, this study provides a comprehensive, CT-based evaluation of the dorsal and volar approaches to percutaneous fixation of distal oblique scaphoid fractures, demonstrating superior anatomic alignment via a dorsal approach. Computed tomography scans were reformatted along the long axis of the scaphoid, allowing for more accurate measurements when evaluating restoration of normal scaphoid anatomy between the 2 approaches. In the future, a larger prospective study with an appropriate power analysis would be integral in further evaluating dorsal and volar approaches to percutaneous scaphoid fixation.
Conclusion
A dorsal percutaneous approach to fixation of acute, unstable distal oblique type scaphoid fractures may achieve a more anatomic reduction than fixation via a volar approach. It remains unclear, however, whether the dorsal approach has any meaningful influence on functional outcome and bone union. In cases of Herbert B1 fracture that are amenable to adequate reduction under flexion, the dorsal approach should be considered to promote restoration of the scaphoid along its true axis. Yet given the technicality of the dorsal approach (ie, proximity to extensor tendons, limited articular surface visualization), and the potential for exacerbation of humpback deformity, decisions regarding approach should be informed by surgeon familiarity, perceived fracture instability, and careful intraoperative evaluation.
Footnotes
Ethical Approval
This study was approved by our institutional review board.
Statement of Human and Animal Rights
This article does not contain any studies with human or animal subjects.
Statement of Informed Consent
Informed consent was not indicated per institutional review board approval, as this article does not include any patient-identifying information.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.