
Abstract
Background:
Camitz opponensplasty performed for severe carpal tunnel syndrome (CTS) is sometimes complicated during the dissection of palmar aponeurosis, and it is difficult to obtain sufficient length and strength of the transition tendon. In this study, we modified the Camitz procedure and devised a tendon-lengthening approach that does not involve the palmar aponeurosis. We evaluated this procedure clinically.
Methods:
Our study included 11 patients with severe CTS and opposable thumb dysfunction. All patients underwent the same modified Camitz procedure including turnover lengthening of the palmaris longus (PL) tendon. Grip strength, pulp pinch, lateral pinch, active range of motion (thumb palmar abduction), and Quick Disability of the Arm, Shoulder, and Hand score were compared before and over 6 months after surgery.
Results:
The mean follow-up duration was 15 months. No postoperative complications such as numbness, pain, or contracture of the thumb were observed. All parameters improved significantly (P < .05) after surgery. At the final follow-up, ultrasonography confirmed the presence and gliding of the transition tendon.
Conclusion:
Our modified method was effective in all cases, and a hemisected PL tendon seemed effective for opponensplasty for CTS.
Keywords
Introduction
Opponensplasty is an established procedure for addressing severe carpal tunnel syndrome (CTS) to achieve hand function immediately after surgery.1-5 Numerous opponensplasty methods have been reported, with procedural details left to the surgeon’s discretion. The original and modified Camitz procedure that involves the palmaris longus (PL) tendon is a common and popular method.6-11 However, using this method, it is occasionally difficult to handle the palmar aponeurosis to avoid transecting the cutaneous branch of the median nerve and to extract fragile or short transition tendons. To address this problem, we devised a modified Camitz procedure, creating a novel opponensplasty technique using turnover lengthening 12 of the PL tendon without involving the palmar aponeurosis. The purpose of this study was to evaluate the efficacy and safety of this tendon-lengthening approach for thumb opponensplasty in severe CTS.
Patients and Methods
Prior to the surgery, we obtained approval from the ethics committee of the involved hospital, as well as informed consent from all patients. We also ensured that the study protocol was in accordance with the ethical guidelines of the Declaration of Helsinki.
We retrospectively reviewed 11 thumbs of 11 patients (3 men and 8 women) who underwent this surgical procedure between June 2019 and August 2022. The patients were over 65 years old (mean age, 74 years; range 65–83 years) and suffered from severe CTS with opposable thumb dysfunction. From the appearance of the thumb, all patients had severe short thumb abductor pollicis brevis (APB) muscle atrophy. Abductor pollicis brevis-compound muscle action potential was not derived or had a significantly reduced amplitude during motor nerve conduction velocity measurements. The procedure was applied to 9 right and two left hands. Grip strength, pulp pinch, lateral pinch, active range of motion (thumb palmar abduction), and Quick Disabilities of the Arm, Shoulder, and Hand (QuickDASH) score were assessed before and over 6 months after surgery. Statistical analysis was performed using a paired t-test to evaluate these outcomes with IBM SPSS Statistics 28.0 for Windows (SPSS Inc., Chicago, Illinois). Significance was defined as P < .05.
Surgical Technique
The presence of the palmaris tendon was confirmed preoperatively by ultrasonography, the transverse width of the tendon was measured, and cases of width >5 mm were identified. We recommend a width of >5 mm for surgeons who are not experienced specialists. A small incision was made to open the carpal tunnel and dissect the median nerve. In cases of severe synovial proliferation, the incision was enlarged, and synovectomy was additionally performed. A new proximal small incision was made in a central part of the forearm, or the existing incision was extended proximally to secure the necessary length of the PL tendon. The tendon was then split longitudinally with a surgical scalpel (blade #11) from its proximal end to its distal end (Figure 1a). The tendon flap was elevated, leaving a suture allowance of approximately 5–6 mm at the distal end of the tendon at the wrist level. After turnover of one half of the tendon, the proximal cut edge was reinforced with nylon mattress sutures (Figure 1b). In the distal side of the tendon, the folded portion of the tendon was reinforced with 3 or 4 stitches using nylon mattress sutures (Figure 1c). Thereafter, the distal tendon was cut. With this, the turnover-lengthened tendon was prepared.
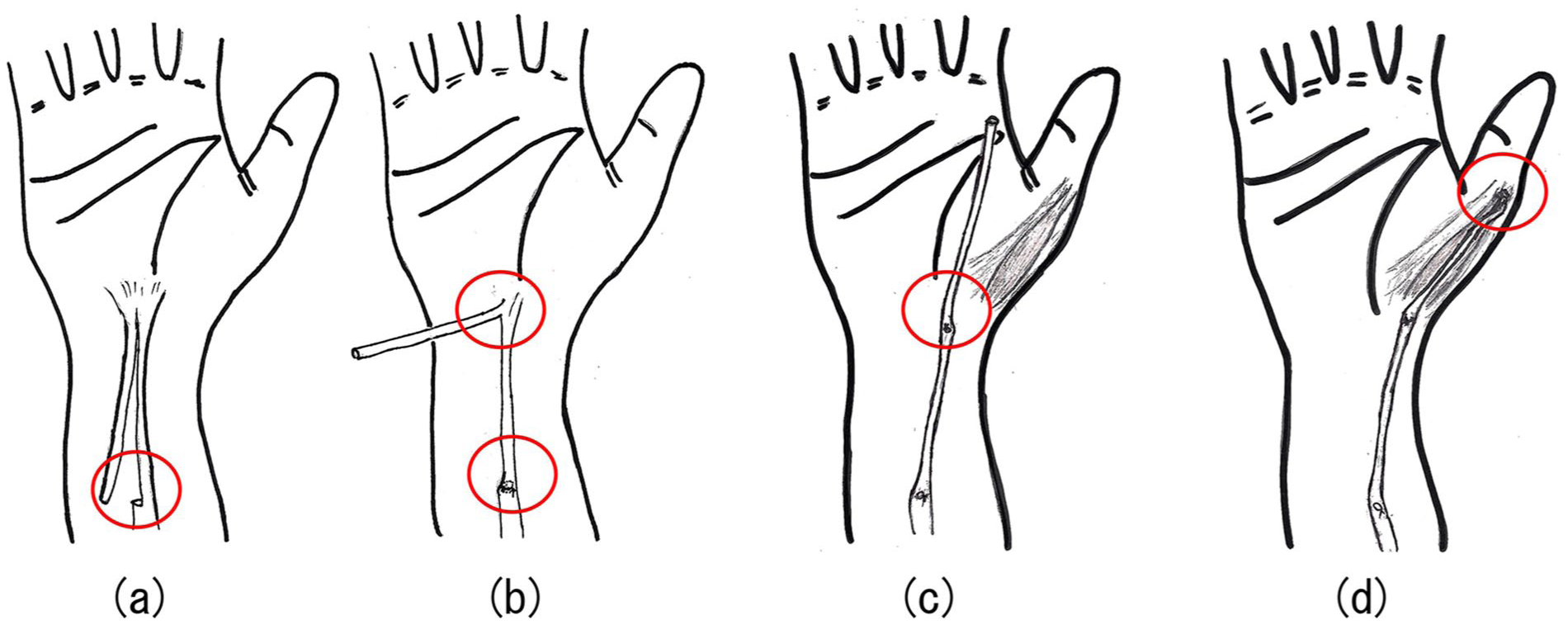
Schema of the surgical technique.
To allow gliding of the PL tendon, the proximal subcutaneous tissue around the PL tendon was dissected in the forearm region. A subcutaneous tunnel was created alongside the APB muscle to lead the PL tendon to the metacarpophalangeal (MP) joint. In this series, we used radial-side complex remnant of palmar fascia and released flexor retinaculum as a pulley based on the route of the original Camitz procedure.10,11 The thumb was placed in the opposing position as much as possible, and the MP joint was temporarily fixed with a Kirschner wire (K-wire). Transferred tendon was fixed in the insertion of the APB and compound tendons at the base of the proximal phalanx using an interlacing suture (Figure 1d).13,14 A short thumb spica cast was used to keep the position of the maximum radial and palmar abduction. Three weeks after surgery, the K-wire and cast were removed, and range of motion exercises for the thumb were performed without restriction.
Results
The postoperative follow-up duration ranged from 7 to 31 months (mean, 15.3 months). The postoperative course was uneventful, and no patient experienced postoperative complications such as numbness, pain, or range of motion limitations in the thumb during daily activities based on the clinical examination and interview. Grip strength increased from an average of 13.7 kg preoperatively to 17 kg postoperatively (P < .05), while the pinch force for pulp pinch increased from an average of 2.1 kg preoperatively to 3.5 kg postoperatively (P < .05) and from 3.7 kg preoperatively to 5.2 kg postoperatively (P < .05) for lateral pinch. Active range of motion (thumb palmar abduction) averaged 32° preoperatively and 49° postoperatively (P < .05), and the QuickDASH score improved from an average of 34.3 preoperatively to 17.8 postoperatively (P < .05). All clinical parameters improved significantly (Table 1). Residual tendon gliding in the transferred PL tendon was confirmed by ultrasound examination over 6 months after surgery (Figure 2).
Clinical Outcomes of Each of the 11 Hands of This Procedure.
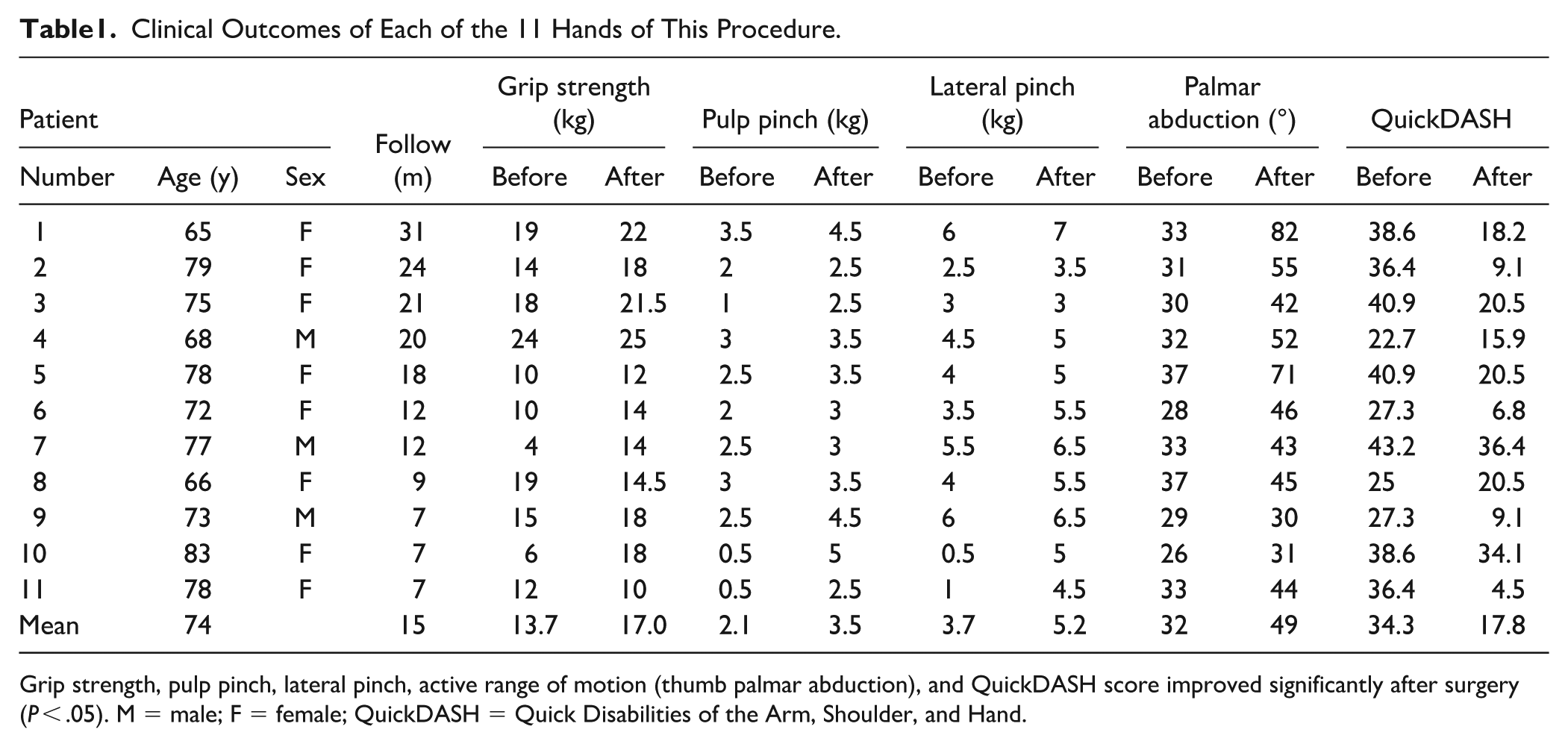
Grip strength, pulp pinch, lateral pinch, active range of motion (thumb palmar abduction), and QuickDASH score improved significantly after surgery (P < .05). M = male; F = female; QuickDASH = Quick Disabilities of the Arm, Shoulder, and Hand.
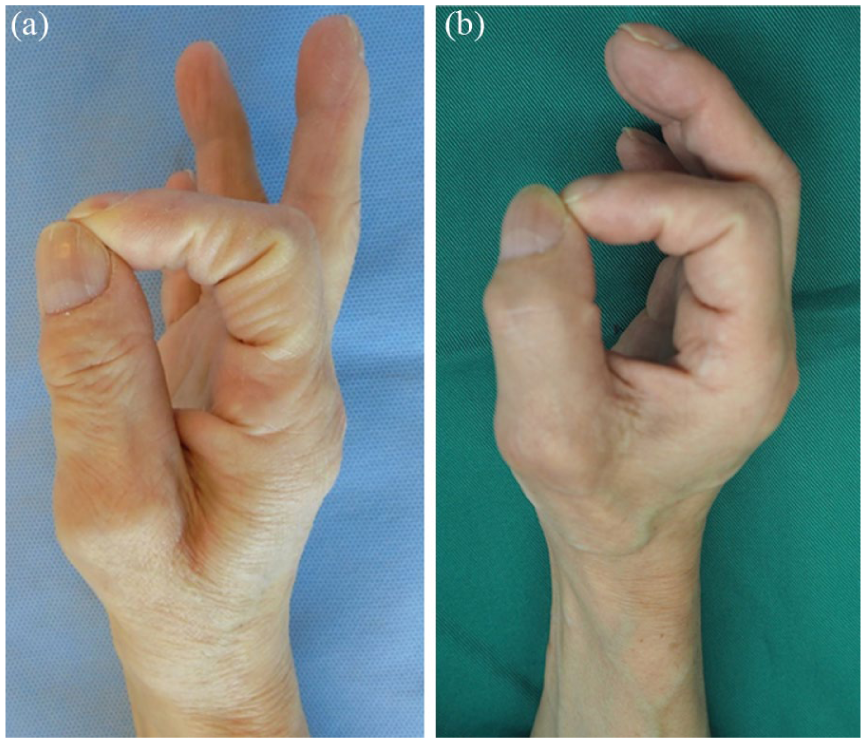
Preoperative (a) and 6-month postoperative (b) perfect “O” sign in a 66-year-old woman with thenar atrophy.
Discussion
Many opponensplasty methods that utilize tendon transfer have been reported in severe CTS with thumb thenar muscle atrophy including the PL, flexor digitorum superficialis of the middle or ring finger, and extensor indicis. In addition, there are various options regarding the site and method of pulley construction, as well as for the insertion point of the transferred tendon.2-4,6,10,11,14,15 We prefer the Camitz procedure for the reconstruction of the opposing thumb as it can be performed in the same operative field as for carpal tunnel release.7-9 However, the conventional Camitz procedure requires extensive surgical invasion of the palmar region and is sometimes complicated. In addition, fragile or short transition tendons may occasionally be extracted, making it difficult to transfer a sufficient length for confrontation reconstruction, which results in reduced loss of function, although it is generally associated with complications such as poor rotation and weak pinch force. 7 Therefore, we devised this technique to achieve a tendon-lengthening effect without using the palmar aponeurosis.
The advantages of our modified technique are as follows: (1) longer transition tendons can be easily harvested without complicated manipulation of the palmar region; (2) it is minimally invasive and can be performed through a small incision; and (3) long, normal-structured tendon tissue can be extracted, unlike the woven palmar aponeurosis. However, a disadvantage is that preoperative ultrasound examination is necessary. To perform the procedure safely, we recommend a tendon width of at least 5 mm whenever possible.
While there are several options of fixation sites and methods for suturing the transferred tendon, we prefer a simple approach in which a single tendon is fixed to the insertion of the abductor digiti minimi muscle on the radial side of the MP joint, which reproduces the most ideal opposition motion, as previously reported by Skie. 15
Whether or not a one-term opponensplasty should be performed in severe CTS is under debate.5,16,17 Seror 18 suggested that even when the APB-compound muscle action potential is not derived and confrontation fails, the carpal tunnel can be opened in some patients. However, the author also suggested poor functional recovery of the thenar muscle in older patients; thus, opponensplasty should be performed for an internal splint during the recovery period. With our technique, even if APB function is fully recovered after carpal tunnel release in cases of severe CTS in older patients, the migrated PL does not interfere with subsequent motion. Therefore, for older patients who are likely to experience an uncertain or prolonged recovery with carpal tunnel release alone, we believe that it is desirable to obtain practical opposing movements as soon as possible after surgery, and we aggressively perform the one-term reconstruction. Several reports of electrophysiologic improvement in patients with severe CTS after long-term postoperative follow-up have been published, with differing views on the necessity of simultaneous thumb confrontation reconstruction in older patients. 17
Regarding the strength of the turnover tendon, Cerovac and Miranda 12 reported good results after shortening or repair of the flexor or extensor tendon using a tendon turnover lengthening technique. Even in biomechanical studies, the turned-over tendon possesses sufficient strength for the reconstruction of extensor and flexor tendons.19,20 In our study, we did not verify the tensile strength of the tendon, but our cases involved internal splints; therefore, strength verification was not difficult. No cases of lost opposition position were observed during follow-up. In addition, the PL was confirmed to be present using ultrasound even in the patient who received the longest follow-up (2 years and 7 months). A similar procedure was reported previously, but it involved a single case, and long-term follow-up was not provided. 21
This study has several limitations. First is the small number of cases, necessitating a larger sample for further evaluation of our results. Second is that the study is a case series, not a comparative study. A randomized controlled trial comparing our method with conventional Camitz opponensplasty is required to provide high-level evidence. The last limitation is the method for evaluating the effectiveness of the surgical procedure. In our results, we observed significant postoperative improvements in many parameters, including the QuickDASH. However, a report which evaluates the minimum clinically important difference values after carpal tunnel release has indicated that a minimum improvement of 18 points in the QuickDASH is required to perceive a meaningful clinical improvement. 22 There is a discrepancy between conventional clinical evaluation methods and patients’ perceived improvement, and it will become increasingly necessary to establish assessment tools that more accurately reflect actual functional improvement and patient satisfaction.
Turnover lengthening is an effective and minimally invasive way to utilize the PL tendon in opponensplasty in patients with a reliable PL tendon because the PL can be divided without depending on the palmar aponeurosis to obtain a sufficiently long transition tendon for opponensplasty.
Footnotes
Ethical Approval
The study was approved by the Ethical Institutional Committee of the Tokyo Hand Surgery Institution.
Statement of Human and Animal Rights
All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional) and with the Helsinki Declaration of 1975, revised in 2008.
Statement of Informed Consent
Informed consent was obtained from all individual participants in the study.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.