
Abstract
Background:
Corticosteroid injections are commonly performed in hand surgery and are often prepared in advance to improve efficiency. Despite aseptic preparation, unused syringes are routinely discarded due to concerns about microbiologic contamination, resulting in substantial avoidable waste. We conducted a controlled laboratory study simulating outpatient injection workflows to assess the sterility of stored corticosteroid-lidocaine injections using next-generation sequencing (NGS).
Methods:
Sterile corticosteroid-lidocaine injections were prepared under aseptic conditions using sterile 3 mL Luer-lock syringes, 0.5 mL of 1% lidocaine, and 3 mg of triamcinolone acetonide (20 mg/mL), drawn with an 18-gauge needle and capped with a sterile 25-gauge needle. Syringes were labeled and stored at room temperature in a closed cabinet away from light and temperature fluctuation. The primary endpoint was the detection of bacterial DNA by NGS on either the 25-gauge needle or the fluid in the syringe. Samples were analyzed at 1 day, 3 days, 1 week, and 2 weeks postpreparation.
Results:
Forty experimental samples and 8 positive controls were analyzed. Of the experimental samples, 39 (97.5%) tested negative for bacterial DNA, including all 20 needle samples and 19 of 20 fluid samples. One fluid sample from the 1-week group tested positive for a Streptococcus species. All positive controls from the 1-day, 3-day, and 1-week groups demonstrated polymicrobial contamination.
Conclusions:
Predrawn corticosteroid injections prepared under aseptic conditions demonstrated a low contamination rate over 2 weeks. These findings support extending injection use beyond same-day administration and provide an opportunity to reduce waste, lower costs, and advance sustainability in hand surgery.
Keywords
Introduction
The administration of a corticosteroid injection in a clinic setting is a common procedure performed in many fields, especially hand surgery, and comes with significant waste. 1 Time constraints for many practitioners result in the frequent practice of premixing and storing syringes of the injectable medications (“injection preparations”) ahead of patient encounters. However, there is often overestimation of the number of injection preparations, resulting in a large burden of plastic syringes, needles, and medications that go unused and are subsequently disposed. Given the low concern regarding the stability of the medications in corticosteroid-local anesthetic injection preparation, the motivation for discarding the injection preparations has been the loss of sterility of the injection and inoculation of a patient. 2 Yet, the magnitude of this burden of waste and the microbiologic safety of the syringes or medication has not been previously studied.
Leaders in the American Society for Surgery of the Hand and American Association of Hand Surgery have championed a “Lean and Green” initiative since the mid 2010s in the hopes of reducing the waste produced and environmental impact of the treatment of patients with hand pathologies. 3 Previous efforts have focused on minimizing excess packaging, single-use disposable products, and overpreparation of surgical and office-based materials.4-6 Injection preparations, which are frequently discarded despite no known breaches in technique or contamination, represent a particularly preventable source of waste. In hand surgery clinics alone, the cumulative environmental burden of unused injections contributes significantly to landfill volume and energy consumption associated with medical waste processing.3,7,8 Despite the scale of this issue, little is known about the actual sterility of predrawn injections over time, and no studies have employed high-sensitivity molecular methods such as next-generation sequencing (NGS) to investigate this question.
The purpose of this study was to simulate standard outpatient corticosteroid injection preparation in a clinically relevant setting and evaluate microbiologic contamination over time using NGS. We aimed to determine: (1) the presence of infection-causing organisms on needles and within syringes at increasing time points from initial aspiration and mixture; and (2) whether the results could inform safe timelines for use of predrawn injections to reduce unnecessary disposal. We hypothesized that predrawn corticosteroid injections prepared under standard outpatient aseptic technique would remain sterile for up to 2 weeks and could be safely retained for later use without significant risk of contamination. Understanding if and when infection-producing bacteria become present will help characterize the presence of microbial contamination over time and explore implications for storage practices. These data can be used to inform the creation of injection preparations at time intervals with low contamination risk while reducing the burdens of time on staff who prepare the injections, environmental waste creation, and cost to the system.
Methods
Study Design
This was a controlled laboratory experiment conducted at an academic orthopedic center. Injection preparations were created to simulate real-world clinical workflows in outpatient orthopedic settings, with standardized preparation, storage, and delayed testing intervals modeled after actual usage scenarios. The primary aim was to evaluate the presence of microbiologic pathogens on predrawn corticosteroid injections stored in typical clinic conditions over time using NGS.
Injection Preparation
Injections were prepared according to standard protocols for sterility in a medical office setting. All injections were drawn by 2 investigators using aseptic technique to simulate routine outpatient practice. While sterile supplies were used throughout, including individually wrapped syringes, needles, and medication vials, the investigators wore non-sterile gloves to simulate typical outpatient preparation protocols. Each injection consisted of a mixture of 0.5 cc of 1% lidocaine and 3 mg of triamcinolone acetonide (20 mg/mL). The solution was drawn into sterile 3 cc Luer-lock syringes using an 18-gauge needle. A sterile 25-gauge injection needle was then affixed, and the cap was secured and left undisturbed. Following preparation, all syringes were labeled with unique identifiers and stored in a locked cabinet at ambient room temperature, shielded from direct sunlight or temperature fluctuation. No refrigeration, agitation, or additional handling occurred after initial preparation. This storage method was intentionally chosen to mirror the conditions in which predrawn corticosteroid injections could be kept in the clinic.
Sample Collection
Injections were prepared at baseline (time 0) and assigned to 1 of the 4 standardized testing intervals to evaluate sterility over time: 1 day, 3 days, 1 week, and 2 weeks. Each time point included a total of 12 specimens: 5 experimental fluid samples, 5 experimental needle samples, and 2 fluid-only positive controls. A total of 7 syringes were prepared per time point to generate these samples, with fluid and needle components analyzed separately. At the prespecified time from aspiration of the medication, syringes were opened in a sterile field. The fluid was expelled into a sterile DNA-free specimen tube. The needle was then cut and removed with sterile wire cutters and placed into a separate sterile tube. Figure 1 demonstrates the study workflow from sample collection to analysis.
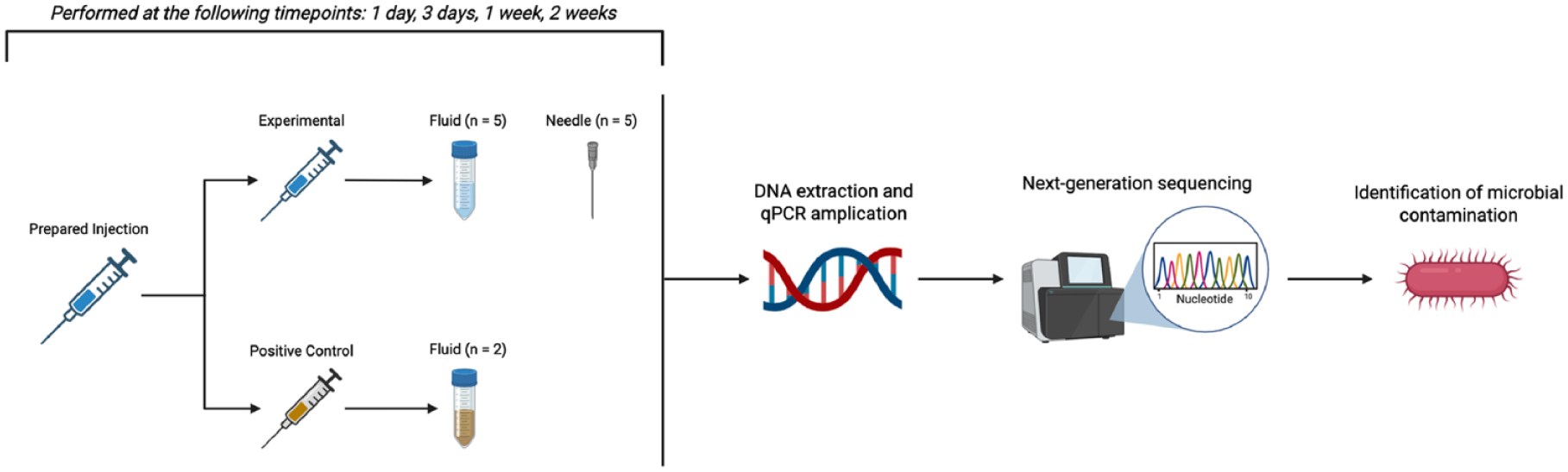
Workflow diagram of injection preparation, sampling, and microbial analysis via next-generation sequencing.
Positive Control Samples
To confirm the sensitivity and reliability of the NGS-based detection method, 2 positive control samples were created through intentional contamination. These syringes were prepared using the same corticosteroid-lidocaine mixture as the experimental samples but were deliberately exposed to environmental surfaces in the clinic to simulate a high-risk contamination event. Specifically, the fluid was expelled onto visibly soiled surfaces such as countertops and work areas and then drawn back into the syringe using the same needle. This process was designed to introduce a diverse array of environmental bacteria into the injection system. The purpose of these positive controls was 2-fold: (1) to establish that heavily contaminated specimens would be reliably identified by the NGS platform, and (2) to reduce the risk of type II error (false negatives) by verifying that our protocol could detect bacterial DNA when it was truly present. These contaminated specimens underwent identical processing, handling, and NGS analysis alongside experimental samples. Of note, the sterile wire cutters that were used on the experimental samples were only used on the control samples after the experimental samples were processed.
Next-Generation Sequencing
All samples were packaged, labeled, and shipped overnight at ambient temperature in a preaddressed box to MicroGenDx Diagnostics (Lubbock, TX) and subjected to NGS analysis. Upon arrival at the lab, the first step involved DNA extraction followed by quantitative polymerase chain reaction (PCR) to determine the bacterial burden and screen for resistance genes, including methicillin, vancomycin, beta-lactam, carbapenem, macrolide, aminoglycoside, and tetracycline classes. Following quantification, samples underwent NGS using a 2-target approach for microbial identification. DNA amplification was performed via PCR using forward and reverse primers targeting 2 highly conserved regions: the 16S rRNA gene for bacterial species and the internal transcribed spacer region for fungal organisms.9,10 Amplified DNA was then pooled based on amplification strength and loaded onto beads for emulsion PCR to generate sufficient DNA quantities for sequencing. Sequencing was carried out on the Ion Torrent Personal Genome Machine platform (ThermoFisher Scientific, Waltham, MA). The Ion Torrent system detects nucleotide incorporation through hydrogen ion release, which generates a measurable change in pH corresponding to DNA sequence construction. After sequencing, a denoising process was conducted to eliminate short or low-quality reads that could interfere with interpretation. 11 Final sequence reads were compared to a curated reference database derived from the National Institutes of Health/GenBank. Sequence alignment was performed using USEARCH software, with a minimum identity threshold of 90% required between the sample read and reference genome for a microorganism to be reported.12,13 A final report showing the relative quantity (DNA load) of each microorganism in each sample was then generated.
Statistical Analysis
An a priori power analysis was performed to determine the appropriate sample size based on an expected difference in contamination rates between the 2-week group and the control group. With an effect size of 0.7, β at .20, and α at .05, it was determined that a minimum of 10 samples per group would be required to detect a statistically significant difference. As such, each time point included 10 experimental samples (5 fluid and 5 needle specimens) in addition to 2 fluid-only positive controls. Descriptive statistics were used to summarize contamination rates across all specimens.
Results
A total of 48 samples were analyzed across 4 standardized time points: 1 day, 3 days, 1 week, and 2 weeks. Each time point included 5 experimental fluid samples, 5 experimental needle samples, and 2 positive control fluid samples, resulting in 40 experimental samples and 8 positive controls overall. After NGS analysis, all needle and fluid experimental samples at every time point were negative for the presence of any contamination, except for 1 fluid sample from the 1-week time point, which showed the presence of a Streptococcus species. This resulted in an overall contamination rate of 2.5% (1/40) among experimental samples. All needle samples (20/20) and 95% (19/20) of fluid samples tested negative for microbial contamination. In contrast, control samples from the 1-day, 3-day, and 1-week time points all showed the presence of multiple bacterial species, including Vibrio rumoiensis, Vibrio species, and Leuconostoc gelidum, confirming the sensitivity of the assay. Interestingly, both control samples at the 2-week time point were negative, despite being subjected to the same environmental exposure protocol as the earlier controls. Full NGS results by sample type and time point are summarized in Table 1.
NGS-Positive Results by Sample and Time Point.
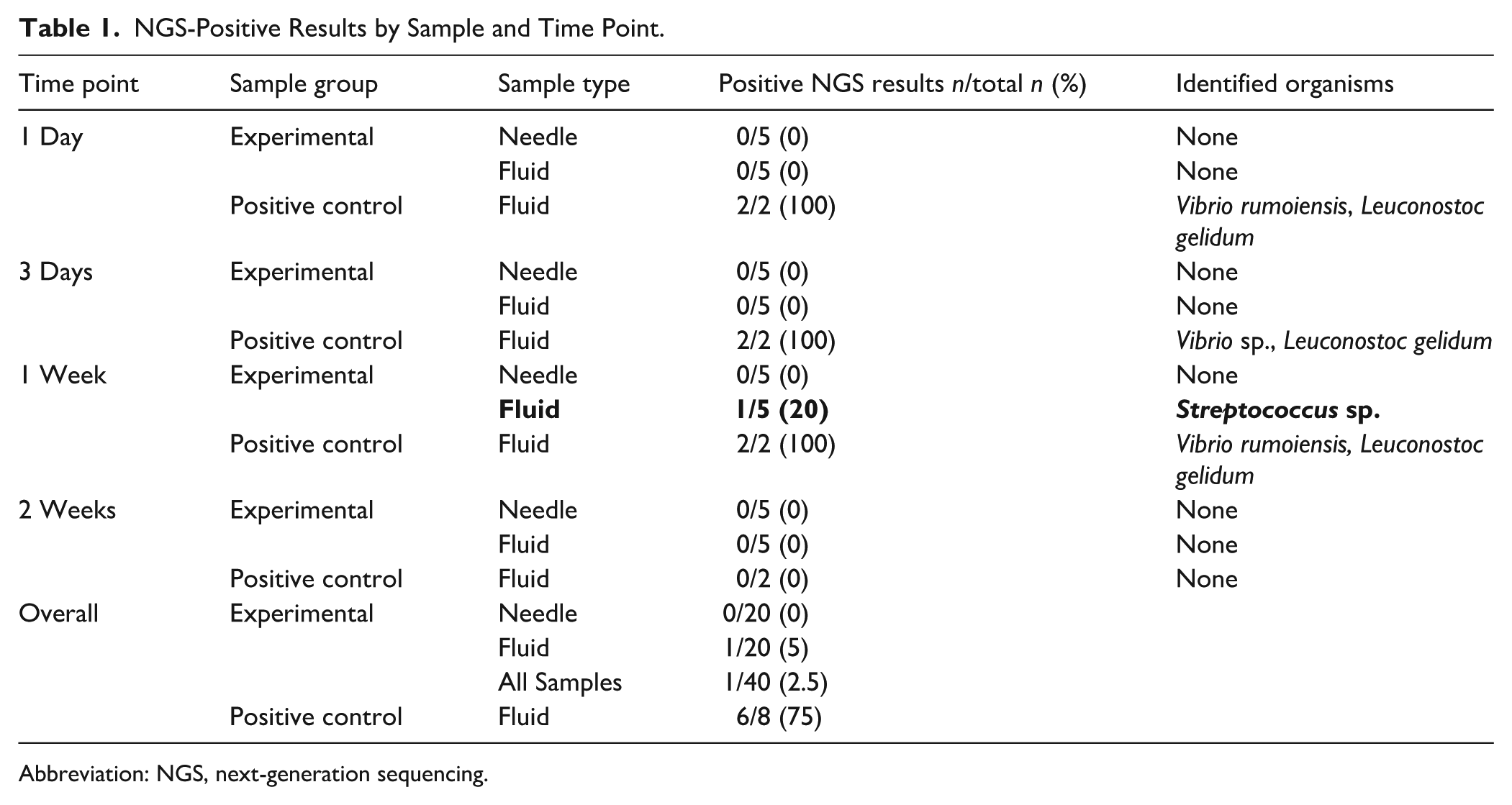
Abbreviation: NGS, next-generation sequencing.
Discussion
This is the first study to utilize NGS to assess microbial contamination of predrawn corticosteroid injections prepared under outpatient clinic conditions. Our findings demonstrate that both fluid and needle components remained largely sterile at all time points up to 2 weeks after preparation, with only 1 out of 40 experimental specimens testing positive. These results align with our original hypothesis: when corticosteroid injections are prepared with aseptic technique and sterile supplies, the likelihood of microbial contamination is exceedingly low. A single positive sample at the 1-week timepoint that grew a Streptococcus species is of unclear clinical significance.
Importantly, our positive control samples demonstrated consistent polymicrobial contamination in the 1-day, 3-day, and 1-week groups, validating the sensitivity of our NGS methodology. However, both 2-week control samples tested negative for contamination, despite being exposed to the same environmental surfaces as earlier controls. This anomaly may reflect biologic variability in contamination events or stochastic differences in environmental flora at the time of exposure. Nevertheless, the control data confirm the functional reliability of the NGS assay and support our conclusion that the sterility of properly handled injection preparations is preserved over time. While our sample size was modest due to resource constraints, the dichotomy between nearly all-negative experimental samples and nearly all-positive control samples offers support for the conclusion that outpatient predrawn injections are microbiologically stable over time.
Traditional microbiological culture methods used in hand surgery have well-documented limitations, particularly in detecting contamination in deep infections or operating room environments. These methods are often plagued by low sensitivity, inability to detect fastidious or slow-growing organisms, and a propensity to miss polymicrobial infections due to competitive overgrowth by more virulent strains.14-19 These shortcomings stem from a variety of factors, including differential growth kinetics and microbial biofilm formation. Although advanced culture-based techniques like sonication, subculture, and varied media can improve yield, they remain complex, costly, and inconsistently adopted in clinical microbiology labs. In addition, culture-based assays carry a risk of false positives from handling contamination, which further undermines their diagnostic reliability.20,21
By contrast, NGS has emerged as a powerful diagnostic tool due to its ability to detect bacterial DNA with far greater sensitivity.14,22-24 In a study of 511 chronic infections, Miao et al 25 demonstrated that NGS improved detection of atypical organisms—including anaerobes, mycobacteria, fungi, and viruses—particularly in culture-negative cases. NGS has also been implemented across multiple orthopedic subspecialties.26-34 For example, Dehghani et al 26 used NGS to evaluate bacterial contamination on scalpel blades after skin incision in upper extremity trauma cases and found no increased contamination compared to unused blades, challenging the long-held surgical dogma of mandatory blade changes after skin incision. Najafi et al 27 used NGS to evaluate operating room environments and found notable rates of contamination on back tables and in ambient air. During the evaluation of revision total shoulder arthroplasty, Namdari et al 28 demonstrated that NGS outperformed traditional cultures in identifying Cutibacterium acnes and distinguishing true infection from contamination. In a multicenter study by Ivy et al, 29 synovial fluid from failed total joint arthroplasties was evaluated using both culture and NGS, revealing that 16% of culture-negative samples were in fact positive on NGS. These studies collectively highlight the diagnostic breadth of NGS in surgical applications. By extending its application to outpatient injection practices, our study provides a high-fidelity method for assessing sterility in a real-world clinical setting.
The potential downstream environmental and economic impact of our findings are noteworthy. As emphasized by Van Demark et al, 3 even minor procedural changes can yield significant environmental savings when scaled across healthcare systems. Injections are among the most common procedures in musculoskeletal clinics and preparations are frequently discarded due to perceived contamination risk. Our data supports the extension of storage duration for such injections, potentially preventing the disposal of thousands of unused syringes annually in each clinic. Future cost-benefit and life cycle assessments will be critical in quantifying the true financial and environmental benefits of storing injection preparations rather than discarding them at early time points. In addition, future research should explore the clinical translation of these findings. While our microbiologic data indicate a low contamination risk, prospective studies are needed to assess whether extended storage is associated with increased rates of postinjection complications, such as clinical infections (eg, cellulitis or abscess). Implementation studies may also help evaluate workflow optimization, cost-effectiveness, and staff satisfaction with batch preparation protocols.
Despite the use of highly sensitive NGS, standardized preparation protocols, and real-world simulation of outpatient workflows, several limitations must be acknowledged. First, our sample size was relatively small, limited by funding and the cost of high-throughput sequencing. Although our findings were consistent across all time points, the study may be underpowered to detect low-frequency contamination events, and larger-scale investigations are needed to assess generalizability across varied clinical settings. Second, while NGS provides high sensitivity for bacterial DNA detection, it cannot differentiate between live and nonviable organisms. As such, we cannot definitively determine whether the single positive result at 1 week represented a viable pathogen. Third, the study was conducted under idealized conditions that simulated standard outpatient workflows using aseptic technique and controlled storage environments. In actual clinical practice, variations in staff training, glove usage, surface contamination, and ambient conditions may introduce unmeasured variables that affect sterility. Fourth, because this was a pilot study, our sampling intervals were selected pragmatically rather than optimized based on prior microbiological data. Future studies could refine this design by including additional time points or stress-testing syringes under different environmental conditions. Fifth, this study aimed only to identify the presence of bacteria on injection preparations, not to assess injection efficacy or stability as has been completed in other studies. 35 Finally, while NGS improves detection over traditional cultures, its extreme sensitivity may identify clinically insignificant contamination. As with other studies using molecular techniques, our results should be interpreted in the context of this limitation, recognizing that the detection of microbial nucleic acid does not always equate to infection risk.
Our findings suggest that corticosteroid injection preparations, when drawn under aseptic conditions and stored in typical clinic environments, demonstrate a low rate of detectable microbial contamination over a 2-week period. The use of NGS provides a highly sensitive, culture-independent confirmation of sterility and offers a novel lens for evaluating outpatient procedural safety. These results support reducing healthcare waste, improving clinic efficiency, and contributing to environmentally conscious surgical practices. Adoption of evidence-based storage protocols for predrawn injections may represent a simple yet impactful step toward achieving a “Lean and Green” future in hand surgery.
Footnotes
Ethical Considerations
This study was approved by our institutional review board.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Statement of Human and Animal Rights
This article does not contain any studies with human or animal subjects.
Statement of Informed Consent
No formal informed consent was required as no living patients were involved in this study.