
Abstract
Background:
Delay in surgical fixation of distal radius fractures (DRFs) beyond 2 weeks is associated with worse patient-reported outcomes. Although socioeconomic disadvantage affects many orthopedic outcomes, its association with delayed DRF fixation is unclear. We evaluated whether neighborhood disadvantage is associated with surgical delay beyond 14 days.
Methods:
This retrospective study used deidentified electronic health records from multiple academic health systems to identify patients undergoing operative DRF fixation from 2012 to 2024. Multivariable logistic regression identified socioeconomic and demographic factors associated with delay beyond 14 days. Covariates included age, sex, area deprivation index (ADI), race, ethnicity, language, Medicare insurance, and Charlson Comorbidity Index (CCI).
Results:
The cohort included 6639 patients (median age 62 years; 64.7% female; 64.8% white; 90.4% English-speaking; 16.1% Medicare). Median time from diagnosis to surgery was 8 days (IQR 5-13), with 25.3% delayed beyond 14 days. Higher ADI (quartile 3: OR 1.59, 95% CI 1.24 to 1.81; quartile 4: OR 1.47, 95% CI 1.20 to 1.80), Spanish-speaking status (OR 1.48, 95% CI 1.08 to 2.02), higher CCI (OR 1.10, 95% CI 1.06 to 1.13), and Medicare insurance (OR 1.25, 95% CI 1.00 to 1.55) were independently associated with delay.
Conclusions:
Socioeconomic disadvantage, limited English proficiency, comorbidity burden, and Medicare insurance were independently associated with delayed DRF fixation. These findings highlight existing disparities in timely orthopedic care of DRFs and support targeted interventions to improve access.
Introduction
Distal radius fractures (DRFs) are among the most common fractures in the United States and worldwide, accounting for a substantial portion of emergency department visits and orthopedic consultations. 1 The timing of surgical intervention for DRF appears to play a crucial role in determining functional outcomes, although this relationship remains incompletely understood. Some studies suggest that delayed surgical management may lead to increased complications and diminished recovery. For example, a systematic review of 1189 patients comparing early versus delayed DRF surgery noted delays greater than 2 weeks for distal radius fracture surgery may be associated with inferior patient-reported outcomes. 2
There is growing interest in understanding how social determinants of health impact orthopedic outcomes. Prior studies have shown that race, ethnicity, and language preference may influence access to care and surgical timing after DRF. For example, in an analysis of a nationwide database including patients undergoing open reduction/internal fixation for DRF, Hispanic patients experienced longer times to surgery than white patients. 3 Insurance status has also been shown to impact surgical access, with Medicaid patients less likely to undergo timely DRF surgery and more likely to experience malunion or nonunion. 4 Similarly, MacIntyre and Dewan 5 linked lower socioeconomic status (SES) and education level to worse outcomes in pain, disability, range of motion, and grip strength following DRF. Finally, in a single-institution study, a higher area deprivation index (ADI) was associated with a lower likelihood of undergoing surgery following an emergency department visit for DRF, although time to imaging was not affected. 6 These findings suggest that structural factors tied to SES may influence surgical access in ways that are not captured by patient-level variables alone.
We thus sought to determine whether socioeconomic disadvantage, as measured by ADI, is associated with delays in surgical treatment of DRF. Although prior studies have shown increased ADI is associated with worse outcomes after other orthopedic procedures,7-10 the relationship between ADI and time to surgery after DRF remains unclear. Given the impact of surgical delay on patient-reported outcomes after DRF, we hypothesized that patients with higher ADI scores would not experience significantly greater delays in time to surgery compared with patients with lower ADI scores.
Materials and Methods
We conducted a retrospective cohort study using deidentified electronic health record data from the University of California Health Data Warehouse, which aggregates data from six academic medical centers across California. Patients who underwent open reduction and internal fixation for distal radius fractures between 2012 and 2024 were identified using relevant Current Procedural Terminology (CPT) codes 25607-25609 for distal radius fracture fixation procedures.
Inclusion criteria were patients aged 18 years and older with a confirmed diagnosis of distal radius fracture who underwent open reduction and internal fixation within 6 months of diagnosis. We excluded patients who did not have data on the time from diagnosis to surgery and those who underwent revision or staged procedures, as determined by CPT codes. Comorbidities were assessed using the Charlson Comorbidity Index (CCI).
The primary outcome was delay to surgery, defined as greater than 14 days from the date of diagnosis to the date of operative intervention. This threshold was selected based on prior literature demonstrating inferior patient-reported and functional outcomes when fixation is delayed beyond 2 weeks, while acknowledging the optimal timing threshold for distal radius fracture fixation remains an area of ongoing investigation. 2 Independent variables included age, sex, race, ethnicity, insurance type (specifically Medicare), and ADI, which was divided into quartiles from Q1 (least disadvantaged) to Q4 (most disadvantaged). This was based on established practices for measuring and quantifying ADI.8,11 Area deprivation index was calculated using the national ADI measure and linked at the ZIP + 4 level, which provides finer geographic resolution than standard ZIP code aggregation.
Because DRF surgery is typically performed in the outpatient setting, and inpatient cases likely represent patients with other traumatic injuries or comorbidities that may impact surgical timing, our analysis was conducted only on patients undergoing fracture fixation as an outpatient. Fracture pattern, displacement, and radiographic severity were not directly available in the structured electronic health record data and therefore could not be explicitly adjusted for; however, restriction to patients undergoing operative fixation was intended to partially mitigate heterogeneity in injury severity.
Statistical analyses included descriptive statistics to characterize the cohort. Multivariable logistic regression analysis was then performed to assess the independent effects of ADI, race, ethnicity, insurance, language, age, and comorbidity burden (CCI) on delay in surgery. Kaplan-Meier curves were constructed to examine time to operative fixation among patients who ultimately underwent surgery, stratified by ADI quartile, and language. These analyses reflect differences in the timing of surgery rather than overall likelihood of operative management. All analyses were conducted using R version 4.5.2 (R Foundation, Vienna, Austria).
Results
In our cohort (n = 6639 patients), the median age was 62 years (interquartile range [IQR] 43-72), and 1818 patients (31.9%) were over 65 years of age. Most patients were female 4298 (64.7%), non-Hispanic 4743 (71.4%), and white 4169 (64.8%). English was the primary language for the majority 5988 (90.4%), while 442 (6.7%) were Spanish-speaking. Medicare was the primary insurer for 1005 patients (16.1%). The median ADI was 4 (IQR, 2-6), with 2318 (36.8%) of patients in quartile 1 and 1136 (18.0%) in quartile 4. The median time from diagnosis to surgery was 8 days (IQR, 5-13). Approximately 74.7% of patients underwent surgery within 2 weeks of diagnosis (52.9% within 1 week, 21.8% within 2 weeks, and 11.6% within 3 weeks). Baseline demographics of the total cohort are reflected in Table 1.
Baseline Demographics and Clinical Characteristics of the Overall Outpatient Cohort.
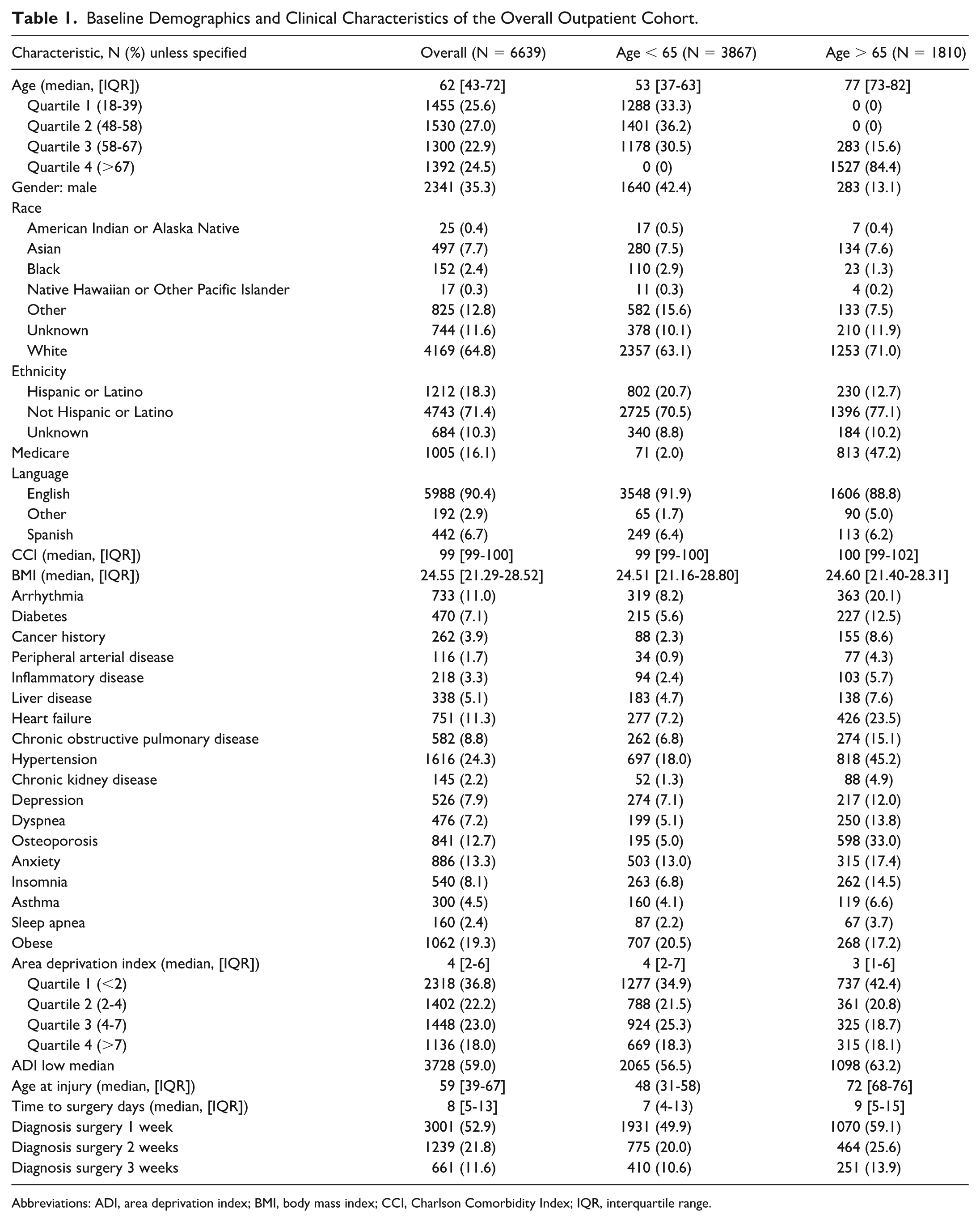
Abbreviations: ADI, area deprivation index; BMI, body mass index; CCI, Charlson Comorbidity Index; IQR, interquartile range.
Multivariable logistic regression confirmed that ADI quartile 3 (odds ratio [OR] 1.59, 95% CI 1.24 to 1.81; P < .001) and quartile 4 (OR 1.47, 95% CI 1.20 to 1.80; P < .001) were associated with significantly increased odds of delay beyond 14 days (Table 2). Spanish-speaking patients (OR 1.48, 95% CI 1.08 to 2.02; P < .05), those with higher CCI (OR 1.1, 95% CI 1.06 to 1.13; P < .001), and those with Medicare insurance (OR 1.25, 95% CI 1.00 to 1.55; P < .05) also had significantly higher odds of delay (Table 2). Race and ethnicity were not independently associated with surgical delay after adjustment for socioeconomic disadvantage, insurance status, language, age, and comorbidity burden.
Multivariable Analysis of Factors Associated With Delay in Surgery Greater Than 2 Weeks From Distal Radius Fracture for the Overall Outpatient Cohort.
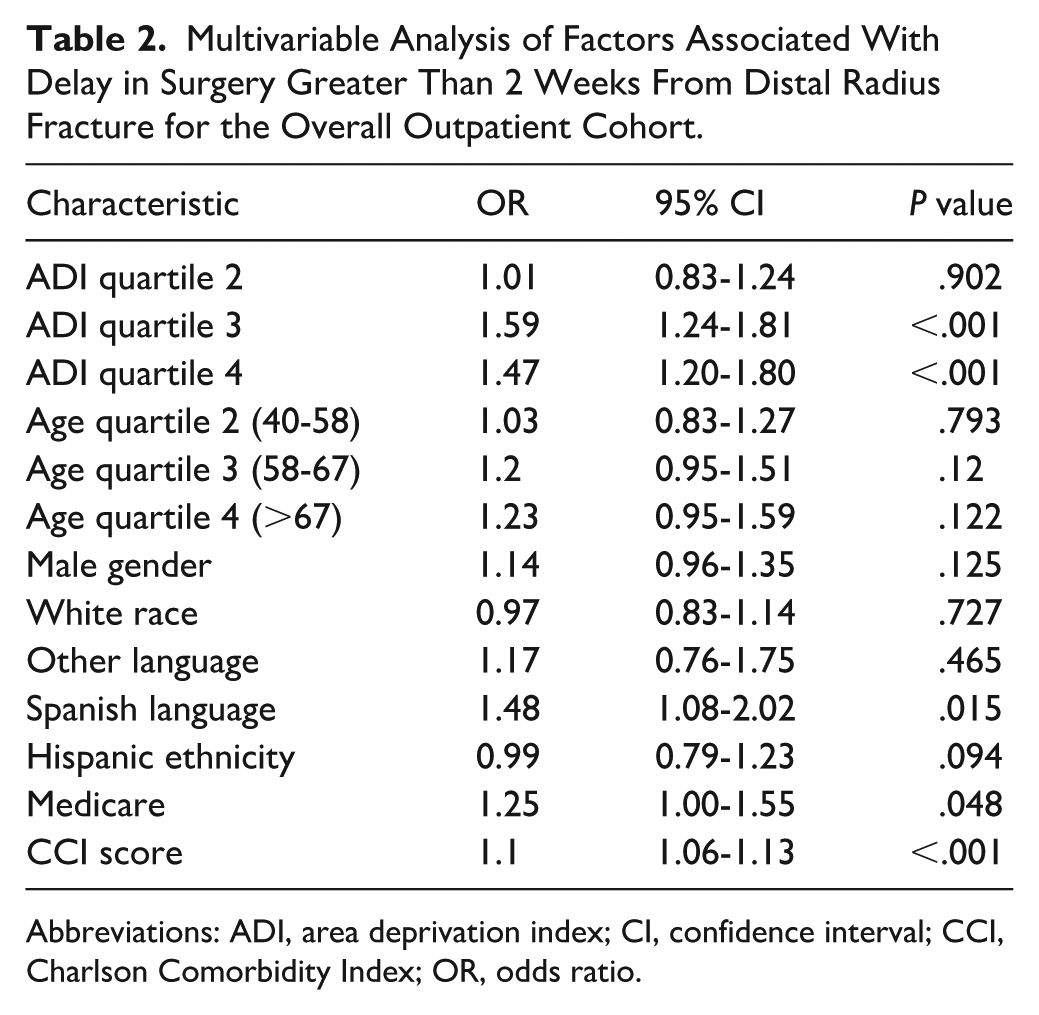
Abbreviations: ADI, area deprivation index; CI, confidence interval; CCI, Charlson Comorbidity Index; OR, odds ratio.
Figure 1 demonstrates the Kaplan-Meier curves of all outpatients by ADI. Figure 2 demonstrates the Kaplan-Meier curves of all outpatients by language.
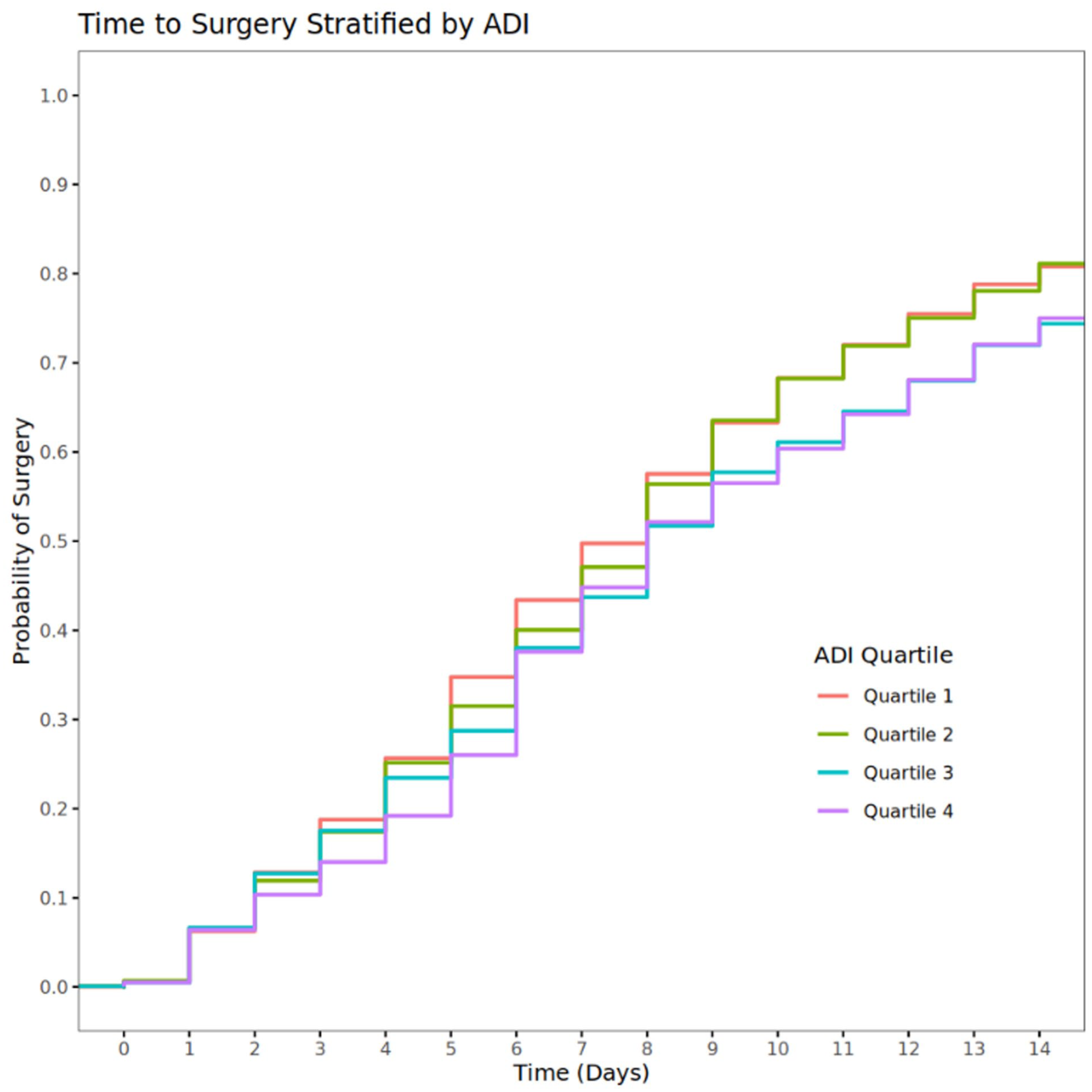
Probability of surgery for distal radius fractures stratified by area deprivation index quartile for the overall outpatient cohort.
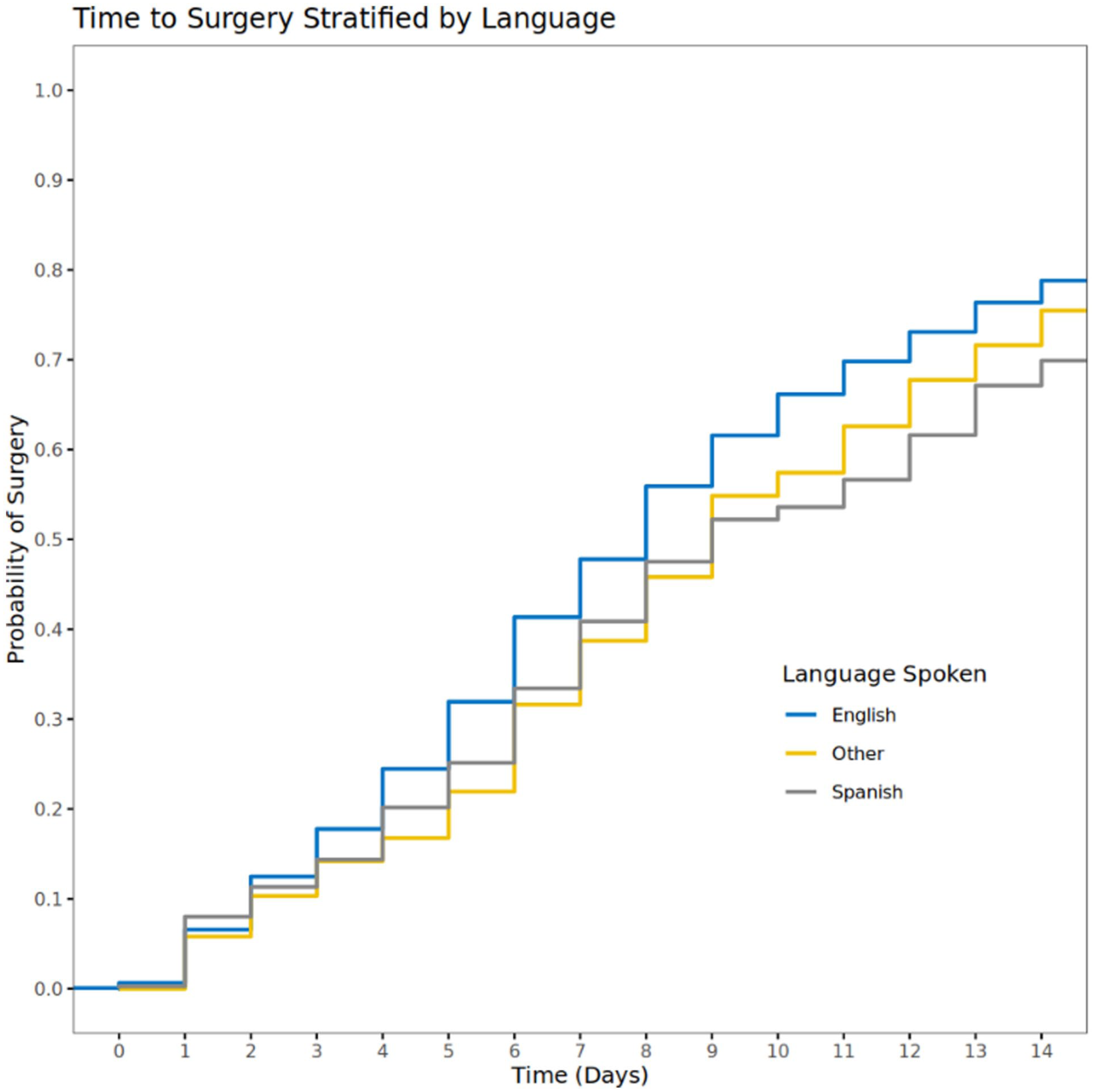
Probability of surgery for distal radius fractures stratified by language for the overall outpatient cohort.
Discussion
In this large, multicenter retrospective study, outpatients undergoing DRF open reduction and internal fixation from more socioeconomically disadvantaged neighborhoods, patients who are Spanish-speaking, patients with greater comorbidity burden, and those insured through Medicare were more likely to experience delays in surgical management of DRFs. These findings contribute to a growing body of literature highlighting the influence of SES and insurance on access to timely orthopedic care.
Patients in ADI quartiles 3 and 4 demonstrated a significantly higher likelihood of experiencing a delay greater than 14 days to DRF fixation compared with those in quartiles 1 and 2. This finding suggests that patients from socioeconomically disadvantaged neighborhoods may face meaningful barriers to timely access to urgent outpatient surgical care. Although similar disparities have not been observed in the management of scaphoid fractures, where delays to fixation were not associated with SES, 12 delays in surgical care have been well documented across other common orthopedic conditions. Higher ADI and Medicaid insurance status have been associated with prolonged time from injury to surgery in anterior cruciate ligament reconstruction, 13 and patients from higher-deprivation areas have been shown to present with more advanced disease severity at initial evaluation for cubital tunnel syndrome 14 and carpal tunnel syndrome. 15
Delays in surgical fixation of distal radius fractures associated with socioeconomic disadvantage are likely multifactorial and due to interactions between patient, provider, and system-level factors. At the patient level, socioeconomic disadvantage may be associated with reduced access to transportation, decreased health literacy, uninsurance or under-insurance, and delayed presentation to specialty care. At the system level, coordination of preoperative evaluation, outpatient surgical scheduling constraints, and variability in surgeon availability may contribute to prolonged wait times to surgery. Structural barriers including insurance authorization requirements and language discordance may further compound these delays by increasing friction in care navigation. Together, these factors likely contribute to the observed disparities in time to operative fixation.16,17
Beyond timing, socioeconomic disadvantage has also been associated with inferior outcomes and care continuity in orthopedic surgery. Low income has been linked to worse postoperative outcomes following distal radius fracture fixation, 18 and delays in fracture care have similarly been reported in adolescent populations from disadvantaged backgrounds. 19 In addition, higher ADI has been associated with incomplete postoperative follow-up after other orthopedic procedures, such as tibial intramedullary nailing, suggesting that systemic barriers may persist even after surgical intervention has occurred. 20
The association between Medicare insurance and delayed surgery persisted even after controlling for age, suggesting that insurance type has an independent impact on care pathways. This also parallels findings in the surgical management of other orthopedic problems, where public insurance is associated with delays in surgical care of pediatric patellar instability, bucket handle meniscus tears, and acute spinal fractures.21-23 Potential contributing factors to insurance-associated delays include the requirement of a primary care referral before surgical consultation and administrative barriers to surgical authorization. 16 This finding highlights the importance of reevaluating policy when payers impose barriers to urgent outpatient surgical access.
Regarding language, Spanish-speaking patients were found to have an increased odds of delay to surgery on multivariable analysis. This suggests language may be yet another barrier to accessing care for DRF in a timely fashion. Prior studies have demonstrated that patients with limited English proficiency or whose preferred language was not English have documented reduced access and longer wait times for surgical care.24,25 Systematic reviews of language barriers also highlight miscommunication, scheduling difficulties, and navigation issues within the system as contributory factors. 26 These data support the interpretation that language and communication barriers may contribute to delays in time to surgery noted in this study.
Greater comorbidity burden was also associated with increased odds of surgical delay on multivariable analysis. Medically complex patients often require additional preoperative optimization including cardiology, anesthesia, or primary care clearance. These necessary steps may delay surgical scheduling even for time-sensitive injuries. Competing health priorities may further shift clinical urgency away from fracture fixation toward stabilization of other potentially more acute conditions. Beyond individual patient factors, coordination across multiple services increases healthcare navigation complexity and can prolong time to operative intervention. In addition, surgical decision-making in older or medically complex patients often incorporates functional status and anticipated recovery goals,27-29 and in some cases, acute fixation may not offer clear substantial benefit over nonoperative management, which may support delayed fixation in specific cases.27,30
Although the causes for delay may be multifactorial, the implications of delayed fixation of distal radius fractures are relatively straightforward. In a retrospective cohort review of DRF patients treated with volar locked plates, patients who underwent early fixation had shorter operative times, lower rates of bone grafting, and fewer additional incisions compared with those treated with late fixation. 31 In addition, Canadian investigators noted that delayed fixation after 14 days was associated with greater healthcare utilization (more clinic visits and therapy sessions) and lower degrees of early wrist flexion. 32 Finally, patients with a delay in fixation of more than 3 weeks have been associated with higher odds of reoperation. 33 Thus, identifying and mitigating factors associated with delayed fixation are essential to optimizing outcomes in DRF care.
Our study has several limitations. As a retrospective analysis of electronic health record data, we are constrained by the accuracy and completeness of coding. We lacked granular clinical data, such as fracture severity or mechanism of injury, which may have influenced surgical timing. Nonetheless, confining our cohort to outpatients only helps mitigate some of these concerns. In addition, our data derive from academic health systems in California, which may limit generalizability to other geographic regions or practice settings. Finally, the specialist density and access patterns of patients at academic hospitals in California may differ from those in community or rural settings, potentially limiting generalizability.
Future research should investigate the specific system-level processes that contribute to these delays and evaluate whether targeted interventions, such as care coordination programs, patient navigation services, and insurance reform, can reduce disparities. Our results suggest that more granular stratification of disadvantage and larger cohorts may uncover additional nuances in access to care. Incorporating additional social determinants of health, such as language preference, health literacy, and access to transportation, will be crucial for developing a more comprehensive understanding of the barriers to timely surgical care.
In conclusion, this study demonstrates that socioeconomic disadvantage, language, and insurance type are significant, independent predictors of delay in DRF surgery. Addressing these disparities will require future system-level changes to improve equity in access to timely orthopedic care.
Footnotes
Ethical Considerations
This study received ethical approval from the University of California, San Francisco IRB (#22-36804).
Consent to Participate
This is an IRB-approved retrospective study, all patient information is deidentified and patient consent was not required. Patient data will not be shared with third parties (#22-36804).
Consent for Publication
Not applicable.
Author Contributions
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability Statements
The data that support the findings of this study are contained within the University of California Health Data Warehouse, a secure institutional platform. Access to the database requires authorized login credentials and knowledge of database-specific coding procedures. Due to institutional and regulatory restrictions, the data cannot be publicly shared. Researchers interested in accessing similar data may contact the University of California Health Data Warehouse for information on authorized access procedures.
Statement of Animal and Human Rights
All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2008.
Statement of Informed Consent
This study received ethical approval from the IRB (approval #22-36804). This is an IRB-approved retrospective study, all patient information was deidentified and patient consent was not required. Patient data will not be shared with third parties.
Disclosure of AI Use
Not applicable.