
Abstract
Background:
Wrist fractures are prevalent, and the diagnostic performance of artificial intelligence for their detection requires clarification. This study aims to determine the diagnostic accuracy of machine learning in detection of scaphoid fractures, distal radius fractures, and other types of wrist fractures on skeletally mature wrist radiographs through a meta-analysis while accounting for heterogeneity of studies using a random-effects model. In addition, this study will compare the results of machine learning to those of experts, including orthopedic surgeons, hand surgeons, and radiologists.
Methods:
Following Preferred Reported Items for Systematic Reviews and Meta-Analysis guidelines, study design, fracture type, radiograph details, artificial intelligence algorithm features, ground truth, and diagnostic performance were extracted. Pooled estimates and heterogeneity were analyzed using a random-effects model. Data were presented using metrics such as area under the curve (AUC). Area under the curve reflects the overall ability of an algorithm to discriminate fractured from non-fractured wrists across all thresholds, providing a broad measure of diagnostic accuracy.
Results:
A total of 48 algorithms were identified from literature that aimed at detecting wrist fractures. The pooled AUC of detection of scaphoid, distal radius, and unspecified wrist fractures by machine learning were 0.88, 0.97, and 0.93, respectively. The AUC of expert detection of wrist fractures was 0.88 for scaphoid fractures and 0.98 for distal radius fractures.
Conclusion:
The performance of machine learning in wrist fracture detection is highly comparable to that of experts.
Introduction
Wrist, distal radius, and carpus fractures are common, accounting for 21% of emergency department upper extremity injuries. 1 Due to its cost-effective and pragmatic nature, plain radiography remains the gold standard when screening for wrist fractures. 1 However, up to 30% of wrist fracture radiographs are misdiagnosed, which may lead to serious patient consequences and complications. 2 Human analysis of radiographs can be time-consuming, subjective, and prone to error, especially when countering complex fractures. 3
Human rooted errors in radiograph analysis may potentially be minimized using an artificially intelligent (AI) powered computer-assisted diagnosis tool. 4 Recent advancements in AI have demonstrated promising potential to enhance diagnostic accuracy and efficiency in medical imaging. 3 Studies have shown that various deep-learning models can be used as assistive methods to increase accuracy and efficiency of wrist fracture diagnosis. 5 One such tool is the convolutional neural network (CNN), a type of machine learning designed to mimic the interconnected neurons of the human brain to analyze images.
Imaging data is processed through multiple layers of a CNN. The CNN then learns by developing and testing algorithms in iterations until it has optimized its ability to identify the feature assigned. Convolutional neural network–based models are trained on large datasets of labeled radiograph images, allowing them to learn distinctive patterns and features associated with fractures. The models can then automatically detect and localize fractures by identifying regions within the image that exhibit fracture characteristics, such as disrupted bone continuity, cortical irregularities, or abnormal bone alignment. 3
Recent developments have shown that machine learning may possess a potential applicability in diagnosing wrist fracture radiographs. Bulstra 6 demonstrated machine learning’s successful capability of predicting whether a patient has a scaphoid fracture through a combination of analyzing pain scores, demographics, and wrist imaging. Machine learning algorithms have also been trained to capture nuances of healing stages among distal radial fractures. 7 In a recent systematic review of AI’s ability to detect and classify scaphoid and distal radial fractures, AI was found to have good diagnostic performance on average; however, a meta-analysis was not performed due to concerns for heterogeneity in the performance of algorithms, ground truth, inclusions, and exclusions among included studies. 8 The current study would be among the first to perform a meta-analysis on algorithms’ ability to detect wrist fractures through a subgroup random-effects model analysis, offering a more thorough assessment of the diagnostic performance of machine learning for this application. The aim of this comprehensive meta-analysis is to quantify the diagnostic binary accuracy of AI in skeletally mature wrist fracture diagnosis. Furthermore, this study assesses the accuracy of AI-driven diagnostic tools in comparison to the interpretations of experts, including attending-level, board-certified radiologists, orthopedists, and hand surgeons with varying level of experience.
Methods
Study Criteria and Eligibility
Study eligibility was based on multiple criteria, including: (1) population type—adult wrist fracture radiographs; (2) index test—evaluation of diagnostic accuracy of neural networks and machine learning interpretation of adult radiographs; (3) reference standards of the machine learning model performance—specificity, sensitivity, and area under the curve (AUC); and (4) type of study—retrospective. The AUC is a single metric used to represent performance of binary classification models. Increasing AUC, closer to 1, indicates greater ability to differentiate between classes. The following studies were excluded: (1) abstracts, opinion pieces, systematic reviews, meta-analysis, and editorials; (2) non-wrist injury radiographs; (3) soft tissue wrist injuries; (4) pediatric wrist radiographs; (5) incomparable reference measures of the performance of the algorithm such as Youden Index or Cochrane; (6) machine learning prediction of fracture rather than diagnosis; and (7) machine learning creating clinical plans for wrist radiographs.
Search Methods and Data Extraction
This meta-analysis was conducted by 4 independent reviewers following the Preferred Reported Items for Systematic Reviews and Meta-Analysis (PRISMA) guidelines; artificial intelligence was not used in the search nor selection of studies. Studies from Google Scholar, PubMed, and Embase were collected using search and mesh terms comprehensive to the diagnostic accuracy of artificial intelligence in detecting wrist pathologies from wrist radiographs (Supplemental 1). A manual search was also performed by 2 distinct medical university libraries. Four researchers reviewed the titles and abstracts, as recommended by the Cochrane Collaboration using the software Rayyan. Among the 4 researchers, a unanimous agreement was reached for all full text included studies based on the study eligibility criteria.
The inclusion of papers was determined by 4 independent reviewers. Data extraction was also completed by the same 4 independent reviewers and values to extract from each paper were confirmed among the four. The following data from each included study were retrieved: (1) study characteristics—study design (prospective or retrospective or public database); (2) type of wrist fracture; (3) radiograph characteristics—type of radiological images (x-ray and views of the radiograph [anterior-posterior or lateral or oblique]); (4) algorithm characteristics—the number of algorithms developed in each study, the number of wrist pathologies tested by each algorithm, specific type or name of the algorithm of AI, data augmentation, and transfer learning information; (5) classification ground truth of radiographs per study; and (6) diagnostic performance of test results—sensitivity, specificity, accuracy, and AUC. In addition, if a specialist competed against the algorithm, their diagnostic performance in terms of sensitivity, specificity, accuracy, and AUC was recorded. Due to the limited number of studies on expert diagnostic accuracy for unspecified wrist fractures, pooled analysis was not performed.
Specialists included attending orthopedic surgeons, hand surgeons, and musculoskeletal radiologists in varying years of practice. The diagnostic performance of experts excluded residents and trainees. Experts did not have physical examination findings or clinical insights regarding the patient radiograph they were interpreting. The diagnosis of a fracture was only based on radiographic interpretation. Clinicians and AI did not have the same fracture criterion. While the AI models identified fractures based on a predefined radiographic pattern, commonly through programs trained to recognize disrupted cortices, clinician interpretations were based on individual diagnostic judgment without a standardized criterion. All included studies determined ground truth through an attending radiologist, hand surgeon, or orthopedic surgeon. No trainee data was used neither for ground truth nor expert diagnostic accuracy.
Data Analysis
Pooled sensitivity, specificity, positive likelihood ratio, negative likelihood ratio (NLR), and their 95% confidence intervals were calculated as a whole and were displayed as forest plots. The summary receiver operating characteristic (SROC) curve, AUC, and Q index were also calculated using a random-effects model. Area under the curve values of more than 80% represented the greatest potential for actual clinical application. Positive likelihood ratio measures how much more likely a positive test result is in the presence of a true fracture, while a NLR measures how much less likely a negative test result is in the presence of a true fracture. SROC Q index (or Q* value) represents the point on the SROC where sensitivity equals specificity; it reflects the maximum joint performance of sensitivity and specificity.
Statistical heterogeneity was determined using Higgins I2 statistic, at the value of >50%, and the Cochrane Q (χ2 test), at the value of P < .10. Review Manager version 5.4 and MetaDisc software were used to analyze the data. Significance was revealed when the value of P is less than .05.
Results
Literature Search
The original comprehensive search for papers studying the diagnostic accuracy of artificial intelligence in wrist pathologies was done by 4 independent researchers through PubMed, Google Scholar, and Embase. The search method was verified and replicated at 2 distinct medical school libraries. The original search yielded 6980 on Google Scholar, 36 from PubMed, and 25 from Embase. Eight additional papers were found manually by 2 librarians at different medical institutions (Supplemental 1). A PRISMA chart outlines the application of inclusion and exclusion criteria to retrieving the final 25 studies (Supplemental 2). Of the studies that met the inclusion criteria, a methodological quality assessment table was created to demonstrate the studies’ quality using the Quality Assessment of Diagnostic Accuracy Studies tool (Supplemental 3).
Study Characteristics
This meta-analysis encompassed 25 studies that adhered to our inclusion criteria. Across the included studies, each algorithm performed fracture detection, applied to one or more fracture subtypes such as scaphoid, distal radius, distal radioulnar, or ulnar styloid fractures (Table 1). All 25 included studies used an artificial intelligence algorithm specifically for binary fracture detection. Among the analyzed studies, all used x-rays for training, validation, and testing. Views of the radiographs were extracted from each study and included anterior posterior, posterior anterior, lateral, scaphoid views, oblique, and ulnar deviation. The machine learning algorithms were used to detect wrist fractures, including scaphoid fractures, distal radial fractures, distal radio-ulnar fractures, carpal bone, and ulnar styloid fractures (Table 1). The total number of wrist images used for training, validation, and testing differed greatly ranging from 192 to 11 112 wrist images (Table 1). For studies using radiographs from patients from their institutions, the year in which the radiographs were taken was recorded. Ground truth of the wrist diagnosis was established differently for each of the 22 studies. However, 17 studies used an expert in the form of an orthopedic surgeon, hand surgeon, and/or radiologist (Table 1).
Description of Study Design and Characteristics of Previously Published Projects That Met Inclusion Criteria for Meta-analysis.
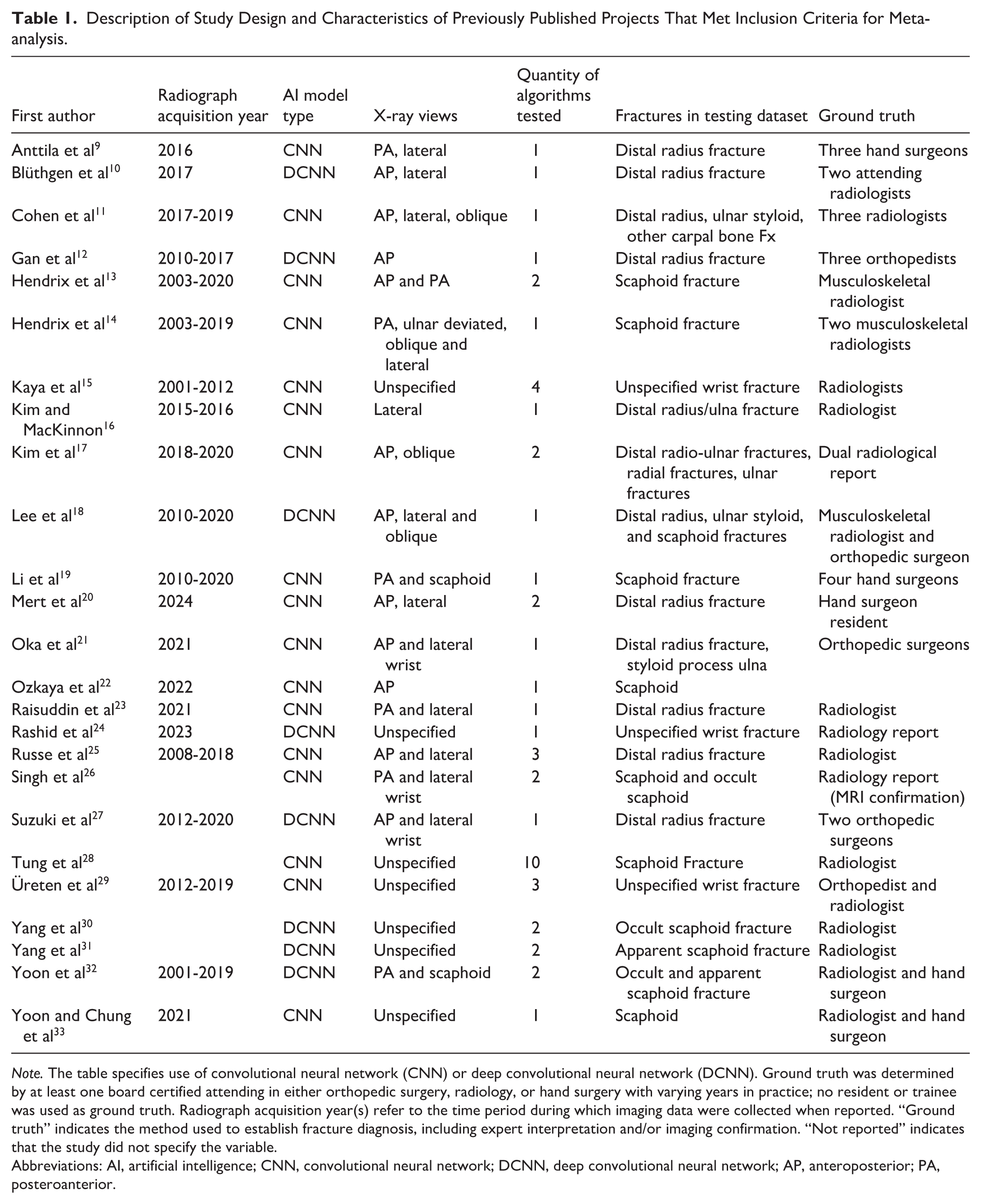
Note. The table specifies use of convolutional neural network (CNN) or deep convolutional neural network (DCNN). Ground truth was determined by at least one board certified attending in either orthopedic surgery, radiology, or hand surgery with varying years in practice; no resident or trainee was used as ground truth. Radiograph acquisition year(s) refer to the time period during which imaging data were collected when reported. “Ground truth” indicates the method used to establish fracture diagnosis, including expert interpretation and/or imaging confirmation. “Not reported” indicates that the study did not specify the variable.
Abbreviations: AI, artificial intelligence; CNN, convolutional neural network; DCNN, deep convolutional neural network; AP, anteroposterior; PA, posteroanterior.
Performance of Machine Learning Algorithms on Detection of Scaphoid Fractures
Ten papers and a total of 22 machine learning algorithms tested the classification and detection of scaphoid fractures (Table 1). The algorithms included a variety of deep learning models such as DenseNet, ResNet, YOLO, and Cascade R-CNN, among others, applied across different types of scaphoid fractures and imaging views. The pooled sensitivity of the algorithms across the studies is approximately 83.15% with a moderate heterogeneity of 57.7% (Supplemental Figure 4). Pooled specificity of machine learning detection of scaphoid fractures was found to be 82.34% with a high level of heterogeneity, 97.4%. The heterogeneity of the AUC was moderate at 31.63% with a pooled AUC of 0.88 (Figure 1).
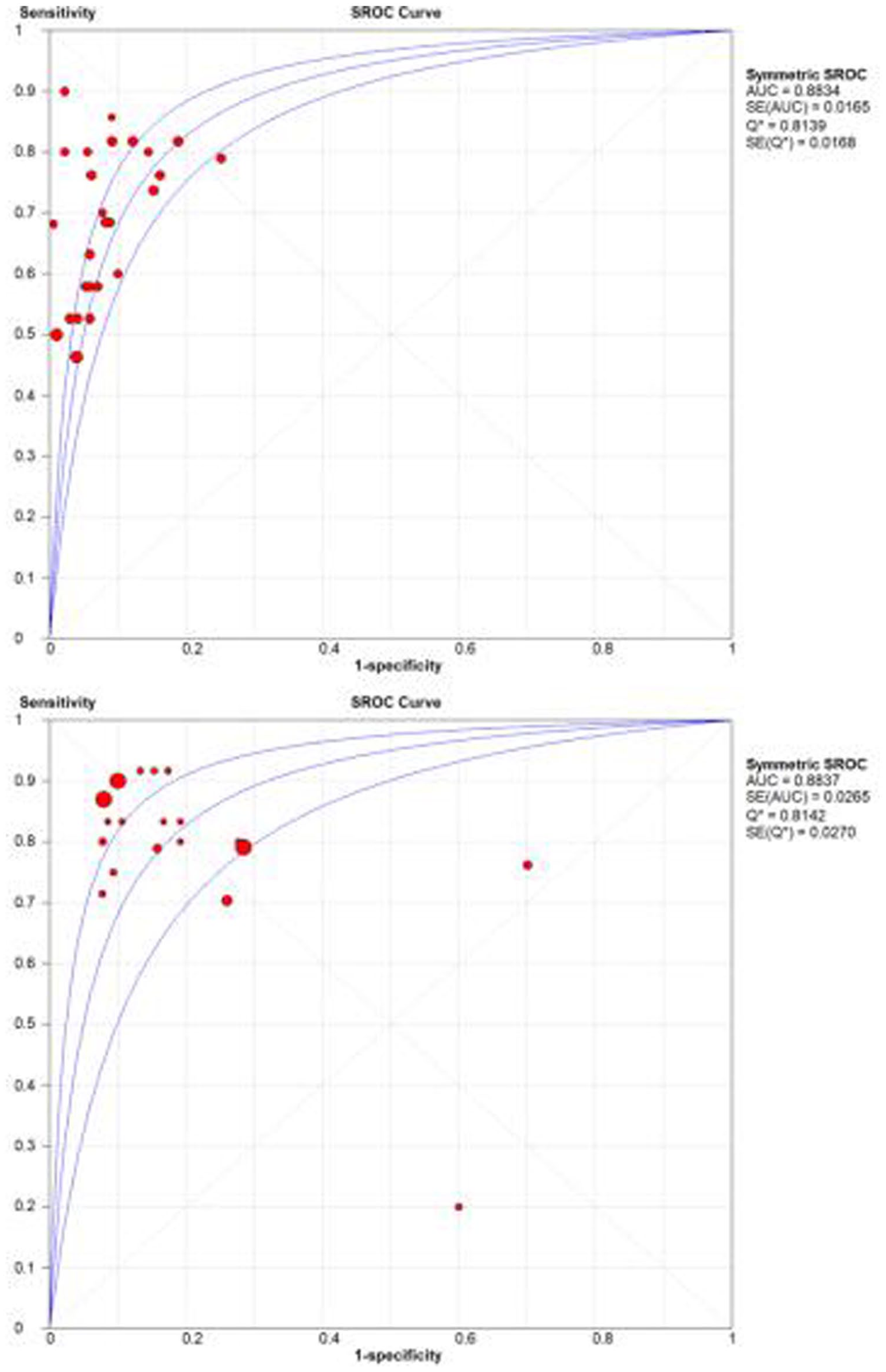
SROC curve of machine learning and expert performance on detection and classification of scaphoid fractures.
Performance of AI on General, Unspecified Wrist Fracture Dataset
A total of 6 studies and 12 algorithm’s diagnostic performance were analyzed on unspecified wrist fracture datasets. The studies evaluated 12 different algorithms, including DenseNet, ResNet, EfficientNet, and VGG-16, among others. The pooled sensitivity of these algorithms was 87%, with a very low heterogeneity of 0.6%; the pooled specificity was found to be 88%, with a high heterogeneity of 93.7% (Supplemental Figure 5). The AUC was found to be 0.93 with a moderate heterogeneity of 44.7%, which falls in the moderate but acceptable range for the meta-analysis category (Figure 2).
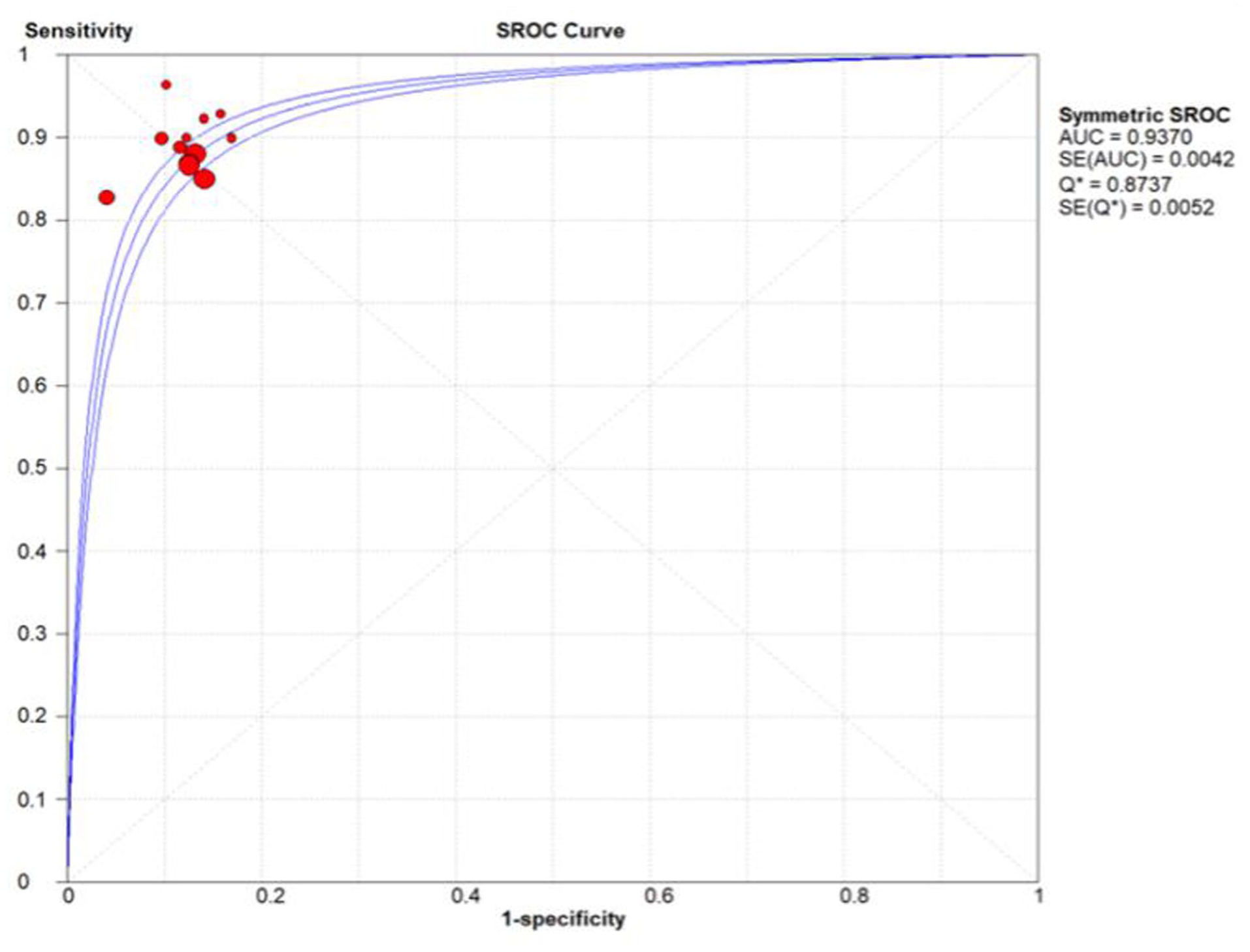
SROC curve of machine learning on detection and classification of unspecified wrist fractures.
Diagnostic Accuracy in Detection of Distal Radius Fractures
A total of 9 studies and 12 algorithms were identified that evaluated the diagnostic performance of machine learning on detection of distal radius fractures. Both the pooled sensitivity and specificity were found to be 92% (Supplemental 6). Pooled AUC was found to be 0.975 among machine learning and 0.982 among experts (Figure 3).
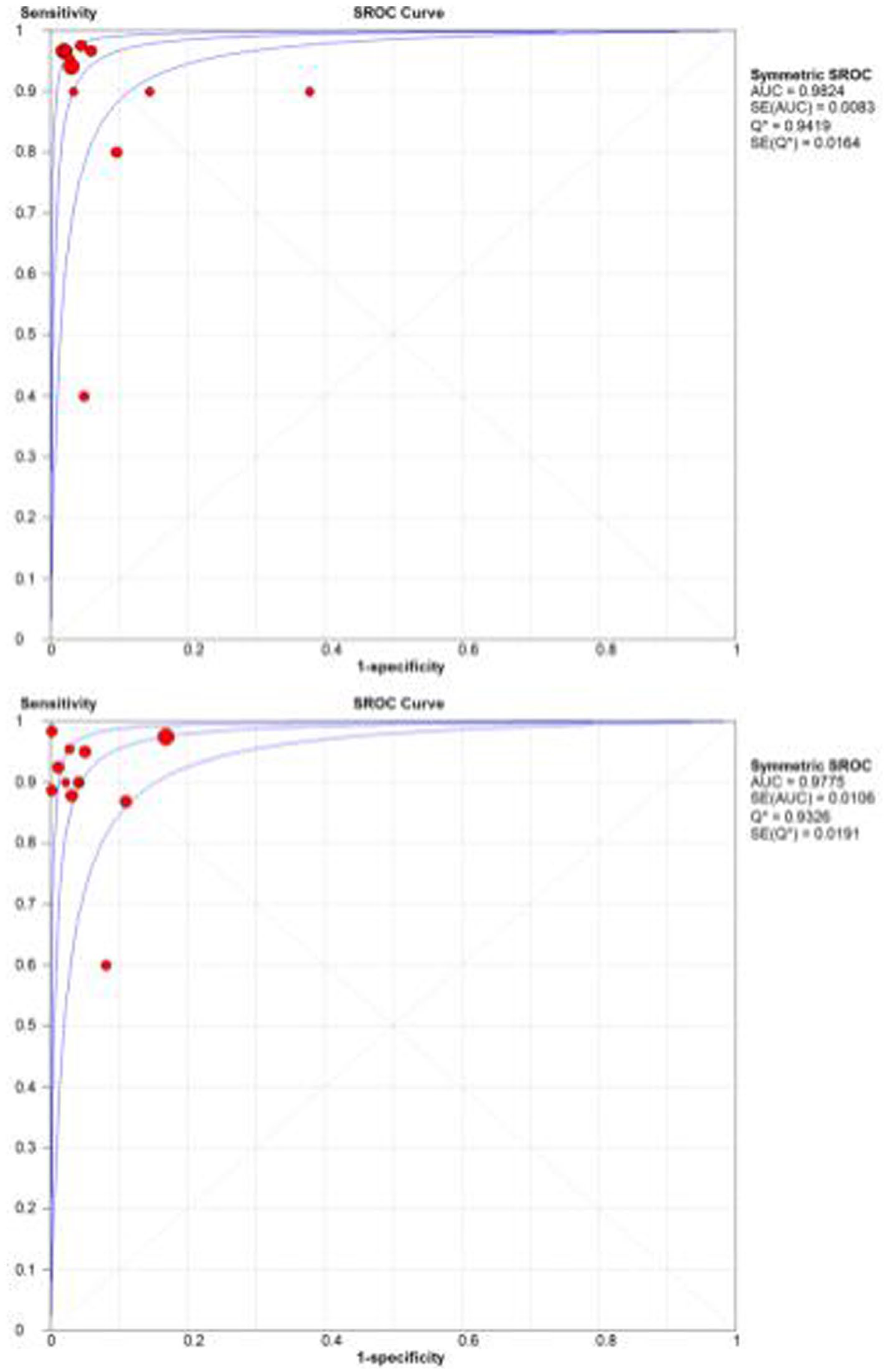
SROC curve of experts (top image) and experts (below image) on detection and classification of distal radius fractures.
Discussion
The results of this study show that the AUC of machine learning in its ability to detect and classify scaphoid, distal radius, and unspecified wrist fracture datasets are at levels comparable to those of experts. Machine learning’s ability to detect and classify wrist fractures suggests its potential as a valuable prospective screening tool, which may help reduce missed fractures by flagging potentially abnormal studies for expedited review. The detection of scaphoid fractures, in particular, could benefit from machine learning adoption, as these are notoriously missed on plain radiography and often require advanced imaging for diagnosis. 34 A study found that experts’ sensitivity and specificity of scaphoid fractures using only plain radiograph was 72% and 64%, respectively. 34 Furthermore, this study demonstrated that scaphoid fracture detection using both computed tomography and x-ray by experts had a diagnostic accuracy of 80%. In this meta-analysis study, machine learning detection of scaphoid fracture from plain wrist radiographs had a promising AUC of 0.88. Artificial intelligence may reduce the number of missed fractures without the need for further advanced imaging. Furthermore, 6 of the algorithms designed to detect scaphoid fractures included occult scaphoid fractures in the datasets, indicating machine learning’s ability to detect subtle, nondisplaced fracture lines.
In Oeding’s systematic review of machine learning, the findings of 9 scaphoid papers were described and summarized. The current study built on this work by pooling sensitivity, specificity, accuracy, and AUC by accounting for heterogeneity. 8 This meta-analysis was able to compare and pool the AUC of scaphoid and other wrist fractures patterns with moderate and acceptable heterogeneity. Another meta-analysis evaluating the performance of 9 algorithms reported an AUC of 0.92 for detecting scaphoid fractures in skeletally mature wrists, while the present study, which pooled 22 algorithms for skeletally mature wrist scaphoid fracture detection, found a comparable AUC of 0.89. 35 Considering the enhanced size of the analysis and that it was limited to skeletally mature radiographs to reduce heterogeneity, this study may provide a more updated and accurate assessment of machine learning’s capability at detecting scaphoid fractures. 35 Regarding machine learning performance on distal radius fractures, Oeding reported a AUC of 0.9 to 0.99 consistent with our random-effects analysis. 8
To date, this is one of the largest meta-analyses and reviews on the diagnostic accuracy of deep machine learning on skeletally mature wrist radiographs. It attempts to counter differences in studies using a random-effects model, categorization by fracture type, and stringent record of neural network properties and design. The analysis resulted in 25 papers and 48 algorithms that aimed to detect skeletally mature scaphoid fractures, distal radius fractures, and other types of wrist fractures, while heterogeneity was reduced using a random-effects model.5,8,35
This study has several important limitations, one of which is inherent to the operation of common neural networks; these algorithms lack a qualitative explanation of how algorithms reach a binary decision. 36 It is unclear how machine learning prioritizes radiographic characteristics to create a binary decision of fracture detection. Factors that may be involved include matrices that outline bone cortices, radiolucency, and displacement. In addition, the diversity of fracture patterns likely contributed to the heterogeneity observed across studies. Comminuted, intra-articular, and minimally displaced fractures often produce subtle cortical disruptions that are more difficult for both AI models and clinicians to detect, whereas simple, extra-articular fractures are typically recognized with higher accuracy. These variations may explain a portion of the heterogeneity in pooled sensitivity and specificity values (I² ranging from 31% to 57%). Although the aim of model design is to create inferences from the fracture site, it cannot be ruled out that the model is analyzing irrelevant parts of the radiograph. Furthermore, the following components were not standard across studies: ground truth, radiographic views in datasets, testing set size, training set size ranging from the hundreds to the thousands, and different subclasses of fracture type within each fracture group, for example, occult and apparent scaphoid fractures being analyzed together (Table 1).
Conclusions
This study analyzed the performance of a total of 48 algorithms to describe the capability of AI in diagnosing skeletally mature wrist imaging in adult x-rays. Compared with orthopedic surgeons, hand surgeons, and radiologists, machine learning algorithms performed nearly identical across all 3 fracture dataset groups. While limitations exist, this study demonstrates that machine learning may be applicable in real clinical settings.
Supplemental Material
sj-docx-1-han-10.1177_15589447261457466 – Supplemental material for Meta-analysis and Systematic Review of Diagnostic Performance of Machine Learning Algorithms on Skeletally Mature Wrist Fractures
Supplemental material, sj-docx-1-han-10.1177_15589447261457466 for Meta-analysis and Systematic Review of Diagnostic Performance of Machine Learning Algorithms on Skeletally Mature Wrist Fractures by Reem Sarsour, Sultan Baz, Christopher E. Collins, Angelene Won, Peter Aldo Giammanco, James Hagerty, Jose Jesurajan, Brian A. Schneiderman, Evelyn Ouro-Rodrigues and Joseph G. Elsissy in HAND
Supplemental Material
sj-pdf-1-han-10.1177_15589447261457466 – Supplemental material for Meta-analysis and Systematic Review of Diagnostic Performance of Machine Learning Algorithms on Skeletally Mature Wrist Fractures
Supplemental material, sj-pdf-1-han-10.1177_15589447261457466 for Meta-analysis and Systematic Review of Diagnostic Performance of Machine Learning Algorithms on Skeletally Mature Wrist Fractures by Reem Sarsour, Sultan Baz, Christopher E. Collins, Angelene Won, Peter Aldo Giammanco, James Hagerty, Jose Jesurajan, Brian A. Schneiderman, Evelyn Ouro-Rodrigues and Joseph G. Elsissy in HAND
Supplemental Material
sj-pdf-2-han-10.1177_15589447261457466 – Supplemental material for Meta-analysis and Systematic Review of Diagnostic Performance of Machine Learning Algorithms on Skeletally Mature Wrist Fractures
Supplemental material, sj-pdf-2-han-10.1177_15589447261457466 for Meta-analysis and Systematic Review of Diagnostic Performance of Machine Learning Algorithms on Skeletally Mature Wrist Fractures by Reem Sarsour, Sultan Baz, Christopher E. Collins, Angelene Won, Peter Aldo Giammanco, James Hagerty, Jose Jesurajan, Brian A. Schneiderman, Evelyn Ouro-Rodrigues and Joseph G. Elsissy in HAND
Supplemental Material
sj-pdf-3-han-10.1177_15589447261457466 – Supplemental material for Meta-analysis and Systematic Review of Diagnostic Performance of Machine Learning Algorithms on Skeletally Mature Wrist Fractures
Supplemental material, sj-pdf-3-han-10.1177_15589447261457466 for Meta-analysis and Systematic Review of Diagnostic Performance of Machine Learning Algorithms on Skeletally Mature Wrist Fractures by Reem Sarsour, Sultan Baz, Christopher E. Collins, Angelene Won, Peter Aldo Giammanco, James Hagerty, Jose Jesurajan, Brian A. Schneiderman, Evelyn Ouro-Rodrigues and Joseph G. Elsissy in HAND
Supplemental Material
sj-pdf-4-han-10.1177_15589447261457466 – Supplemental material for Meta-analysis and Systematic Review of Diagnostic Performance of Machine Learning Algorithms on Skeletally Mature Wrist Fractures
Supplemental material, sj-pdf-4-han-10.1177_15589447261457466 for Meta-analysis and Systematic Review of Diagnostic Performance of Machine Learning Algorithms on Skeletally Mature Wrist Fractures by Reem Sarsour, Sultan Baz, Christopher E. Collins, Angelene Won, Peter Aldo Giammanco, James Hagerty, Jose Jesurajan, Brian A. Schneiderman, Evelyn Ouro-Rodrigues and Joseph G. Elsissy in HAND
Supplemental Material
sj-pdf-5-han-10.1177_15589447261457466 – Supplemental material for Meta-analysis and Systematic Review of Diagnostic Performance of Machine Learning Algorithms on Skeletally Mature Wrist Fractures
Supplemental material, sj-pdf-5-han-10.1177_15589447261457466 for Meta-analysis and Systematic Review of Diagnostic Performance of Machine Learning Algorithms on Skeletally Mature Wrist Fractures by Reem Sarsour, Sultan Baz, Christopher E. Collins, Angelene Won, Peter Aldo Giammanco, James Hagerty, Jose Jesurajan, Brian A. Schneiderman, Evelyn Ouro-Rodrigues and Joseph G. Elsissy in HAND
Footnotes
Authors’ Note
Reem Sarsour is also affiliated with Department of Orthopedic Surgery, University of Minnesota, Minneapolis, USA.
Ethical Considerations
This study was approved by our institutional review board.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Statement of Human and Animal Rights
No study subjects were used in this meta-analysis.
Statement of Informed Consent
Human subjects were not used in this study so informed consent was not obtained.
Supplemental material
Supplemental material is available in the online version of the article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.