
Abstract
Background
More data is needed on the short- and medium-term efficacy and safety of the Willis covered stent in treating distal internal carotid artery (DICA) aneurysms and vertebral artery dissecting aneurysms (VADAs).
Methods
Records of all 42 patients with DICA aneurysms or VADAs treated with the Willis covered stents at our institute between July 2014 and January 2019 were retrospectively examined. The patients’ demographic information, symptoms, diagnosis, treatment procedure, immediate and follow-up clinical and angiographic outcomes were extracted.
Results
46 Willis covered stents were successfully implanted in all of the 42 patients (total 43 aneurysms). Immediate complete aneurysm occlusion was achieved in 37 patients (38 aneurysms) (88.4%), and endoleak occurred to 5 patients (5 aneurysms) (11.6%). 2 patients died post-operatively from procedure-related complications, another one died from reasons unrelated to the procedure. Among the remaining 39 patients, non-lethal complications occurred in 4 patients including ptosis and diplopia of the right eye, intra-operative hemorrhage and carotid cavernous fistulas (CCF). Angiographic and clinical follow-ups (means ± standard deviation: 8.8 ± 5.3 months) were done for 32 patients (33 aneurysms). Complete occlusion was maintained in all of the 33 aneurysms. 2 of the 32 patients had significant though asymptomatic parent artery (PA) occlusion. No ischemic or hemorrhagic event occurred during the follow-up period. The modified Rankin Scale (mRS) score was 0 in 31 patients and 1 in the remaining 1 patient.
Conclusions
The Willis covered stent could be a safe and effective treatment for complex DICA aneurysms with excellent durability. In addition, the Willis covered stent treated all of the 3 cases of VADAs in the study with complete success without any complications, however, as the number of the VADA cases was small, more cases are needed to further confirm the efficacy and safety of the Willis covered stent in treating VADAs.
Keywords
Introduction
Distal internal carotid artery (DICA) refers to the C2-C7 segments of the internal carotid artery (ICA) according to the Bouthiller classification. 1 DICA aneurysms account for approximately 40% of intracranial aneurysms. 2 Treatment of DICA aneurysms remains challenging because of bony obstacles and their unfavourable morphologies.2–4 Surgical approaches to complex DICA aneurysms are problematic and carry the risk of intraoperative bleeding (up to 23%) and recurrence (up to 8.3%).2,4,5 In some cases, severe intraoperative bleeding could lead to intraoperative death.4,6 Conventional endovascular approaches such as coil embolization have proven superiority to surgical approaches in treating unruptured and ruptured intracranial aneurysms, however, incomplete obliteration of aneurysms and recurrence are inherent problems associated with these approaches.4,7,8
In recent years, treating DICA aneurysms with covered stent has been successful in a highly selective group of patients. 2 However, as covered stents such as the Jostent and Symbiot stents were not designed for intracranial use and are very stiff and lack longitudinal flexibility, it is difficult to navigate them through the tortuous segments of the ICA and could cause ICA dissection and rupture.2,8
The Willis covered stent (MicroPort, Shanghai, China) was developed specifically for navigating intracranial vasculature to immediately exclude aneurysms from circulation while preserve parent artery (PA) patency.2,4,8 It could also reconstruct ICA wall and reduce mass effect. 4 In recent years, the Willis covered stent has been used to treat various types of DICA aneurysms such as blood blister-like aneurysms (BBAs), large and giant aneurysms, pseudoaneurysms and dissecting aneurysms and showed promising short- and medium-term angiographic and clinical outcomes in terms of efficacy and safety.2,4,8–14 However, as it is a relatively new device (first reported in 2007, 10 ) more data on the efficacy and safety of the Willis covered stent in treating various DICA aneurysms is needed.
Vertebral artery (VA) dissecting aneurysms (VADAs), a common cause of stroke and subarachnoid hemorrhage (SAH) in young adults, face the same challenge as DICA aneurysms, because of its deep position and closeness to important side branches such as the anterior spinal artery and the posterior inferior cerebellar artery. Its treatment strategy remains controversial. 15 It has been reported that the Willis covered stent was efficacious and safe in treating VADAs.15,16 However, data on this topic is scarce.15,16
In this retrospective study, we report the efficacy and safety of the Willis covered stent in treating patients with DICA aneurysms and VADAs at our institute.
Methods
Patients
We retrospectively reviewed the records of patients with DICA aneurysms or VADAs treated with the Willis covered stent at our institute between July 2014 and January 2019. DICA aneurysms and VADAs were diagnosed by computed tomography (CT) angiography (CTA) and digital subtraction angiography (DSA). Beside the presence of DSA confirmed DICA aneurysm(s) or VADAs, patients treated with the Willis covered stent must have a PA with a diameter of 2.5–5.0 mm and passed a balloon occlusion test (BOT) before the procedure (more details on the BOT in Supplemental material Appendix S1).10,11,17–19 A patient was excluded if he/she had cardiopulmonary disease(s) and could not tolerate the procedure, had a PA with a diameter <2.5 mm or >5.0 mm, had extremely tortuous ICA or VA and thus was unsuitable for stent implantation, or had other serious disease(s) with a life expectancy of less than a year.
Medical records, clinical data, angiographic findings and endovascular treatment records of the included patients were reviewed to extract relevant information. This study was approved by the ethics committee of our hospital. All methods were performed in accordance with the Declaration of Helsinki. All patients or their caregivers gave written informed consent before the endovascular procedures and data collection.
The Willis covered stent
The Willis covered stent (MicroPort, Shanghai, China) is a balloon-expandable stent specifically designed for intracranial vasculature and has been described in detail previously.2,7,8,11,14–16,20 More detailed description could be found in Supplemental material Appendix S2.
Endovascular treatment
The procedure was described in detail previously.2,4,9,14–16,20 A detailed descriptions could be found in Supplemental material Appendix S3.
Clinical and imaging follow-up
Clinical examinations and DSA were conducted after the endovascular procedure. After discharge, patients were instructed to come back whenever their neurological symptoms deteriorated or new neurological symptom(s) occurred and a head CT or MRI was performed if necessary. The modified Rankin Scale (mRS) was used to evaluate the clinical treatment outcomes during patients’ clinical follow-up. Follow-up DSA was performed for the patients at least 2 months after their endovascular procedure to evaluate status of the aneurysms and to exclude the possibility of residual endoleak, aneurysm recurrence or in-stent stenosis.4,21,22
Statistical analysis
Continuous variables were presented as means ± standard deviations (SD), and categorical variables were presented as numbers (percentages [%]).
Results
Patient and aneurysm characteristics
Between July 2014 and January 2019, 42 patients with DICA aneurysms or VADAs were treated with the Willis covered stent at our institute, among them, 32 patients (33 aneurysms) had medium-term angiographic and clinical follow-ups. Each patient's baseline characteristics, types and locations of their aneurysms, treatment and outcomes were described in detail in Table 1. Table 2 listed a summary of patient and aneurysm characteristics. These 42 patients had a mean age of 45.2 ± 12.6 years, and 20 of them were male. 41 of the patients had single aneurysm while the remaining patient had 2 neighbouring aneurysms, bringing the total number of aneurysms treated in this study to 43. 16 of the patients had ruptured aneurysms and SAH at presentation, among them, 3, 10, 2 and 1 patients had Hunt and Hess (H-H) grade I, II, III and V lesions, respectively (Tables 1 and 2).
Demographic characteristic, endovascular treatment, immediate and follow-up outcome of patients treated with Willis covered stent.
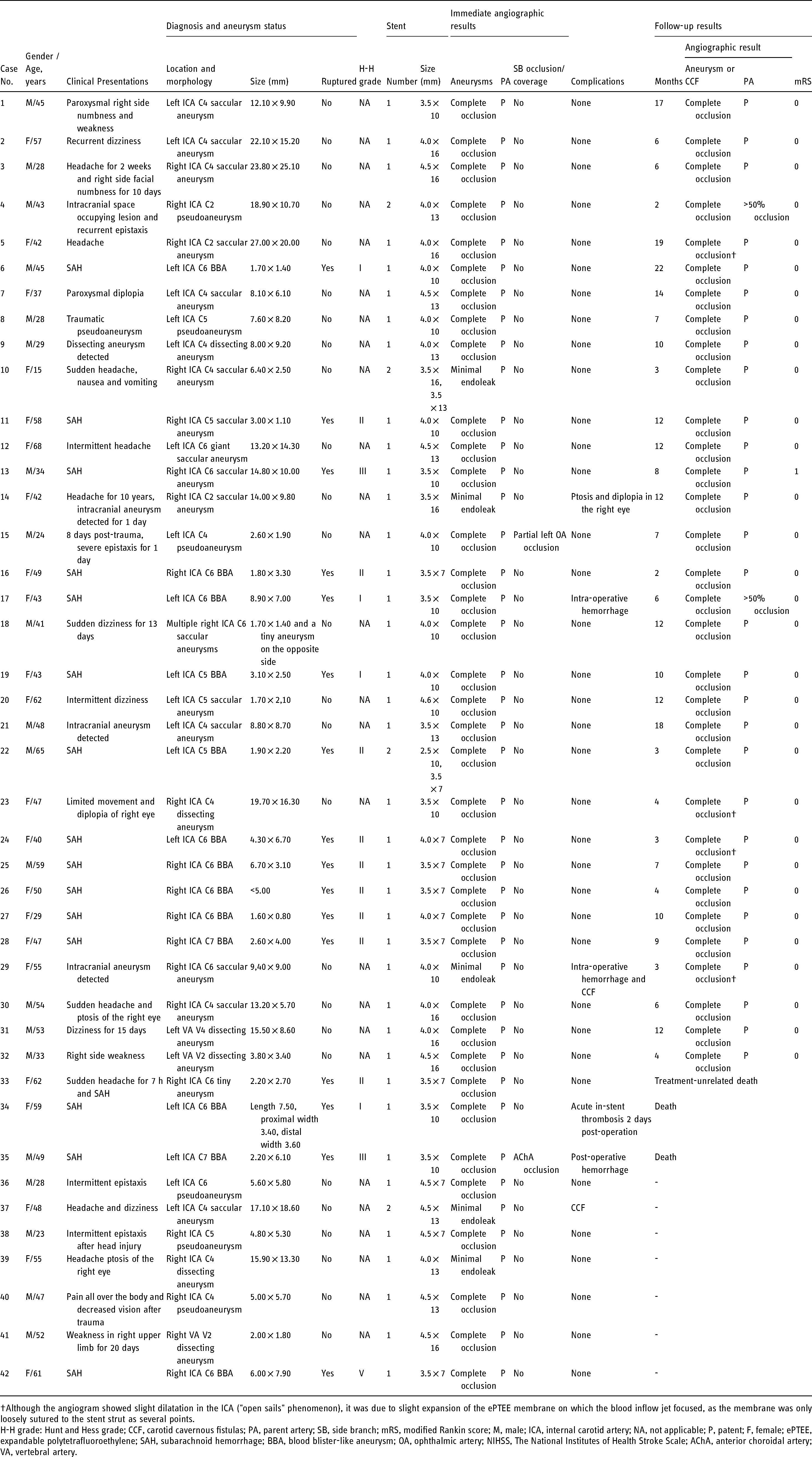
Although the angiogram showed slight dilatation in the ICA ("open sails" phenomenon), it was due to slight expansion of the ePTEE membrane on which the blood inflow jet focused, as the membrane was only loosely sutured to the stent strut as several points.
H-H grade: Hunt and Hess grade; CCF, carotid cavernous fistulas; PA, parent artery; SB, side branch; mRS, modified Rankin score; M, male; ICA, internal carotid artery; NA, not applicable; P, patent; F, female; ePTEE, expandable polytetrafluoroethylene; SAH, subarachnoid hemorrhage; BBA, blood blister-like aneurysm; OA, ophthalmic artery; NIHSS, The National Institutes of Health Stroke Scale; AChA, anterior choroidal artery; VA, vertebral artery.
Summary of patients demographics, aneurysm characteristics and treatment (N = 42).
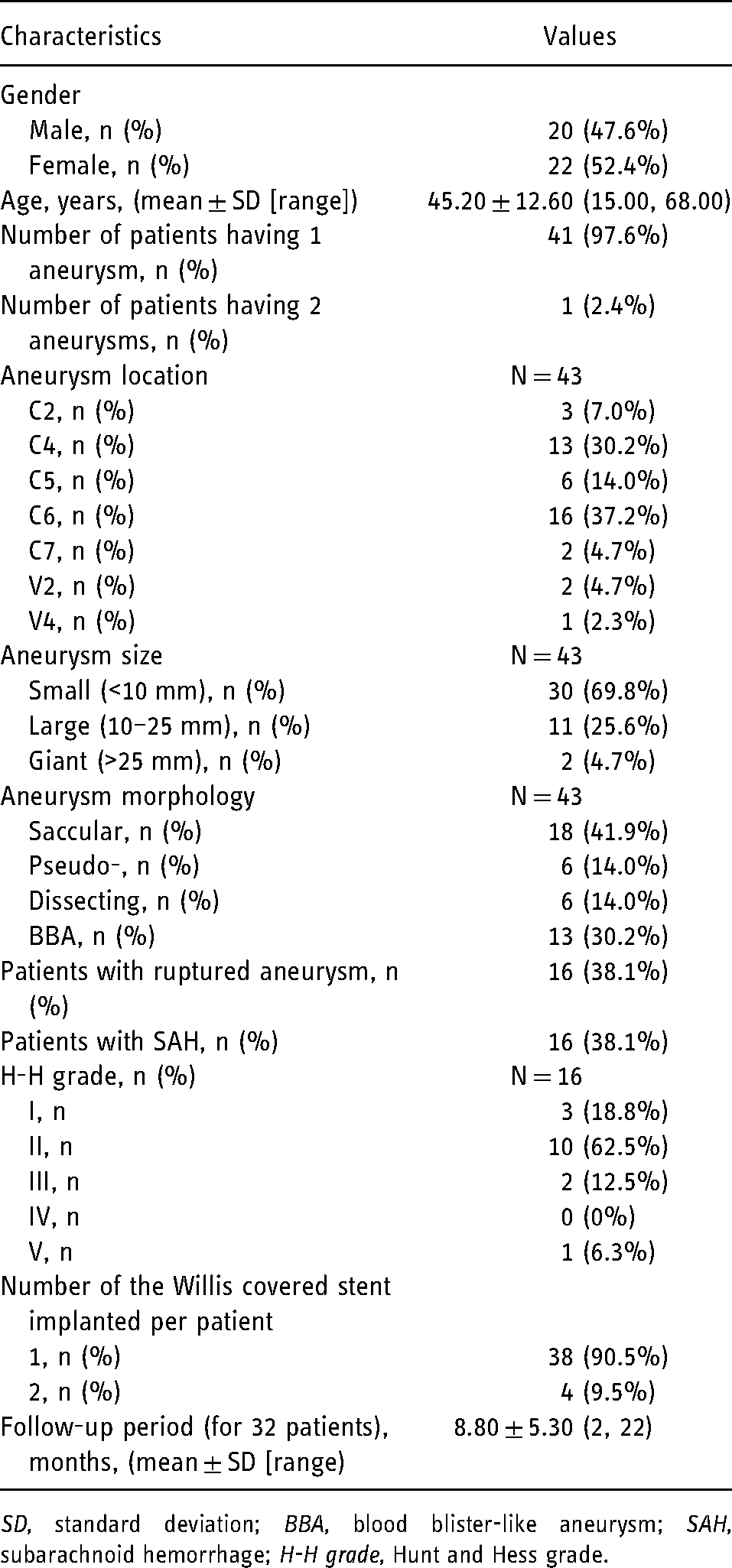
SD, standard deviation; BBA, blood blister-like aneurysm; SAH, subarachnoid hemorrhage; H-H grade, Hunt and Hess grade.
40 of the 43 aneurysms were DICA aneurysms and 3 were VADAs. 30, 11 and 2 of the 43 aneurysms were small (<10 mm), large (10–25 mm) and giant (>25 mm), respectively. 12 Of the 43 aneurysms, 18 were saccular aneurysms, 6 were pseudoaneurysms, 6 were dissecting aneurysms and 13 were BBAs. These aneurysms were at C2 (3), C4 (13), C5 (6), C6 (16), C7 (2), V2 (2) and V4 (1) (Tables 1 and 2).
Immediate procedural results
Primary procedural outcomes were described in Tables 1 and 3. A total of 46 Willis covered stents were successfully implanted in the target lesion in all of the 42 patients (43 aneurysms). Immediate complete aneurysm occlusion was achieved in 37 patients (38 aneurysms) (88.4%) (Figure 1). 2 patients had endoleak after the stent was inflated for the first time, however the endoleak disappeared either after observation for several minutes or after the stent was re-inflated with a pressure of 6–8 atmospheres (Figure 2). 2 other patients had endoleak that was eliminated by implanting a second stent. 5 patients (5 aneurysms) (11.6%) had slight endoleak immediately after the procedure, including 2 patients who each had 2 stents implanted. All of the 42 patients showed PA patency immediately after the procedure. One patient with a left C4 pseudoaneurysm (Patient No. 15) had partial occlusion of the ophthalmic artery (OA) and another one with a ruptured left C7 BBA (Patient No. 35) had occlusion of the anterior choroidal artery (AChA). In both cases, the aneurysm was very close to the side branch (SB), it was unavoidable that the membrane of the Willis covered stent would cover the SB upon stent implantation. However neither showed any relevant symptoms possibly due to collateral circulation (Tables 1 and 3).
A 34-year-old male (patient No. 13) with a ruptured right internal carotid artery (ICA) C6 large aneurysm.
A 49-year-old female (patient No. 16) with a right ICA C6 blood blister-like aneurysm (BBA).
Summary of immediate and medium-term treatment outcomes.
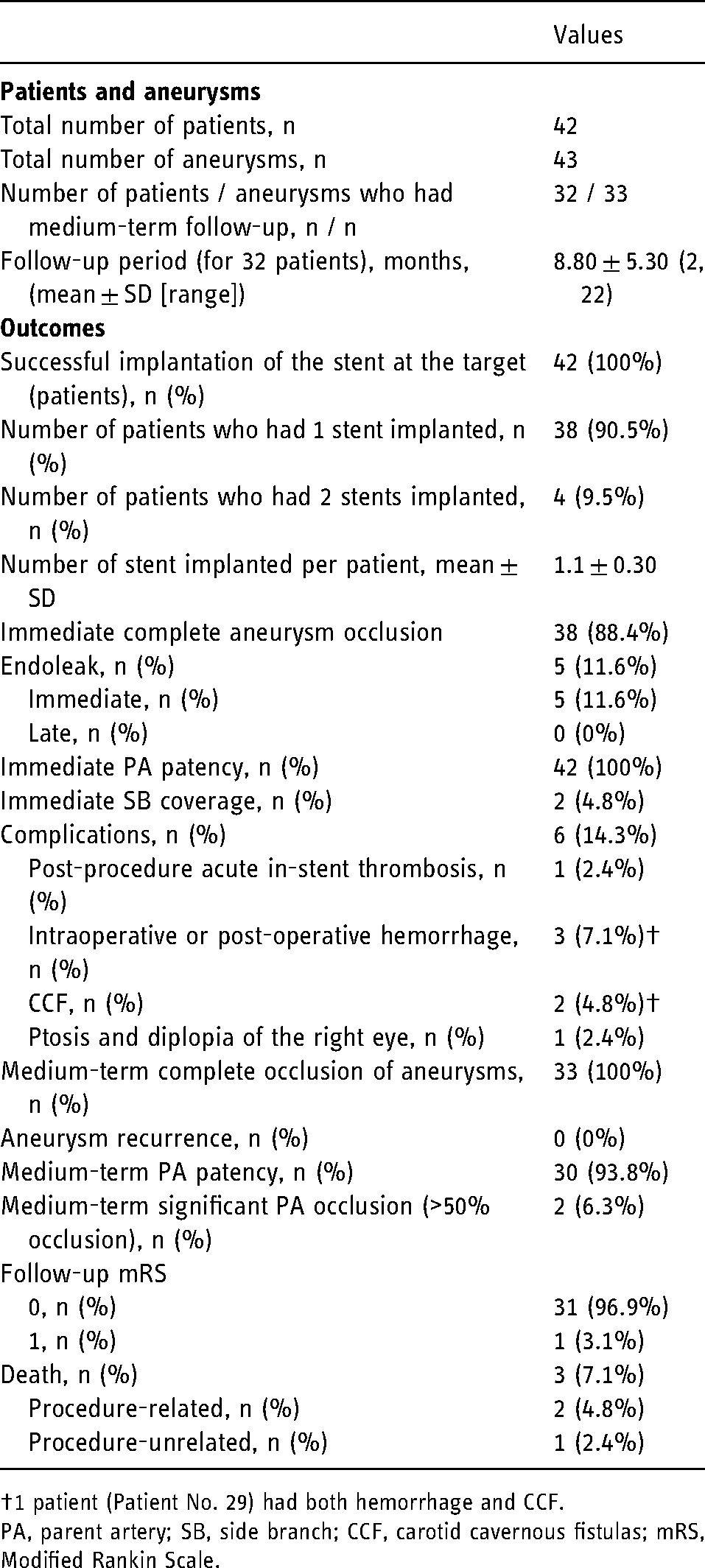
1 patient (Patient No. 29) had both hemorrhage and CCF.
PA, parent artery; SB, side branch; CCF, carotid cavernous fistulas; mRS, Modified Rankin Scale.
The immediate procedural results for the subgroups of the 39 patients with DICA aneurysms (40 aneurysms) and the 3 patients with VADAs (3 aneurysms) (Table 1) were summarized in Table 4.
Subgroup analyses of immediate and medium-term treatment outcomes based on DICA aneurysms or VADAs.
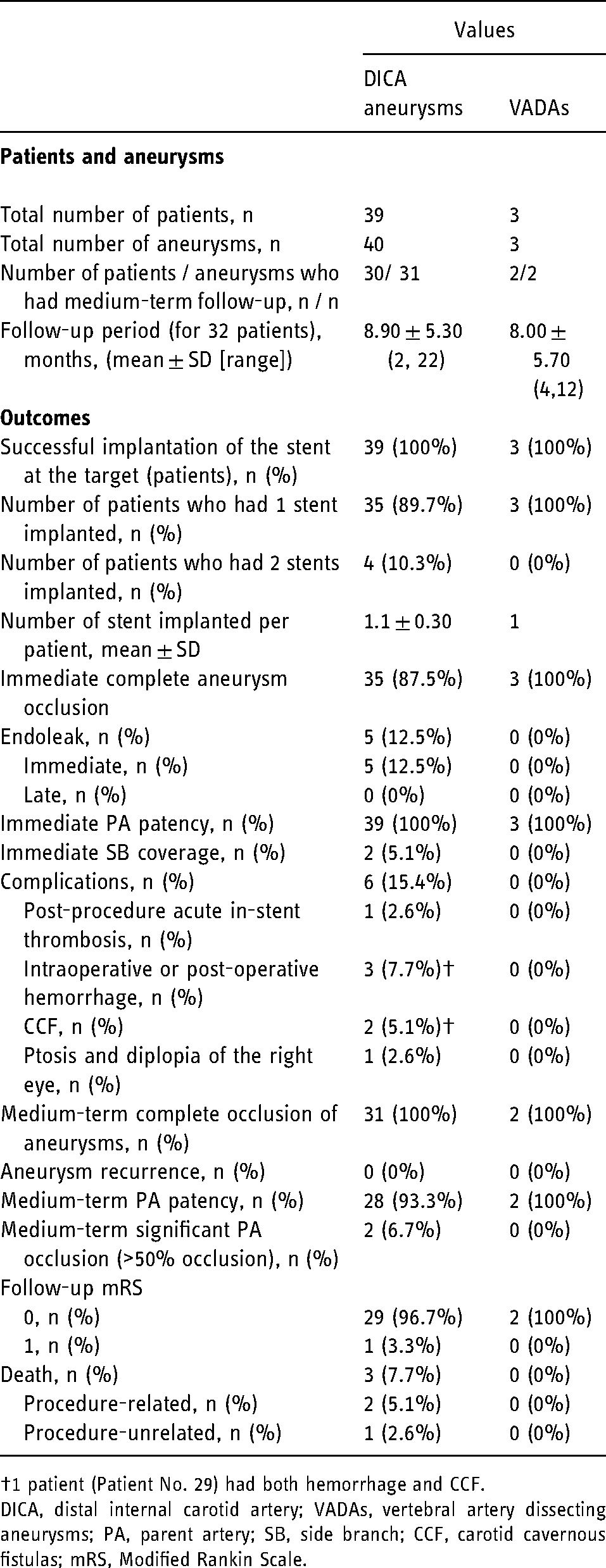
1 patient (Patient No. 29) had both hemorrhage and CCF.
DICA, distal internal carotid artery; VADAs, vertebral artery dissecting aneurysms; PA, parent artery; SB, side branch; CCF, carotid cavernous fistulas; mRS, Modified Rankin Scale.
Complications
1 patient with multiple right ICA C6 saccular aneurysms (Patient No. 18) had a stent navigation-related incident. When the distal end of the microguidewire was navigated to the distal M1 segment of the right middle cerebral artery (MCA), the Willis covered stent fell off the balloon catheter and migrated to the M2 segment of the right MCA. Angiogram showed that the stent was attached antegradely to the M2 segment with good local vascular patency and normal distal blood flow. Another Willis covered stent was implanted to cover the target aneurysm without incident. Post-operation angiogram showed good stent placement, complete aneurysm occlusion and good PA patency. The Willis covered stent was delivered successfully without incident in the remaining 41 patients.
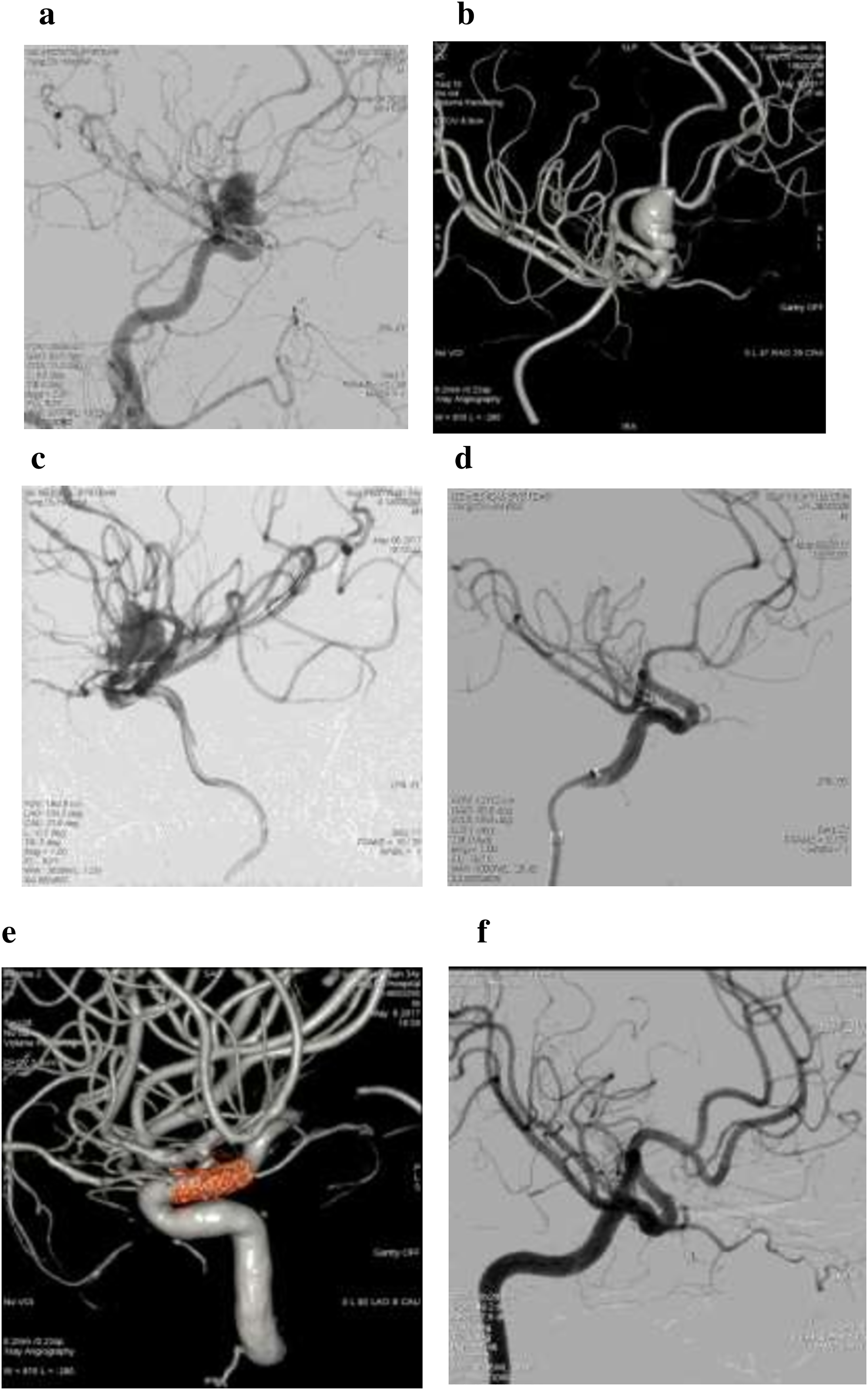
Complications were described in Tables 1 and 3. 3 deaths occurred shortly after the procedure. 2 of them were considered to be procedure-related. One patient with a ruptured left C6 BBA (Patient No. 34) had complete aneurysm occlusion immediately after the procedure. However, she experienced acute in-stent thrombosis 2 days post-operation probably due to vascular endothelial injury that occurred during stent delivery, and was treated with inter-arterially administrated 3.5 mg tirofiban and 9 mg alteplase. The patient improved (complete BBA occlusion, minimal residual thrombosis in ophthalmic segment of the ICA, National Institutes of Health Stroke Scale 1), however she died several days after discharge. Whether her death was due to the anti-thrombosis treatment or BBA re-rupture was undetermined. A second patient with a ruptured left C7 BBA (Patient No. 35) achieved immediate complete BBA occlusion after the procedure. However he experienced post-operative hemorrhage 1 day after the procedure, a craniotomy for hematoma evacuation and decompressive craniectomy were successfully performed, and his condition slightly improved before worsened again. Another CT scan revealed hemorrhage at the site of the operation. The patient's caretaker refused further treatment, and the patient died within 1 month after discharge. His hemorrhage was possibly due to undetected transient vasospasms during the procedure which could potentially cause stent-parent vessel mismatch by creating a false impression of aneurysm occlusion. 19 The third lethality was unrelated to the procedure. It involved a patient with a ruptured right C6 tiny aneurysm (Patient No. 33) (Figure 3(a)-c). After achieving complete aneurysm occlusion immediately after the procedure (Figure 3(d)-e), the patient experienced headache and fell into a light coma 3 days post-operation, head CT showed more severe SAH compared to pre-operation SAH (Figure 3(f)). Cerebral angiography revealed that an aneurysm in the left superior cerebellar artery (SCA) was the source of the increased SAH (Figure 3(g)). Interventional therapy was initiated, however, after the patient was put under general anesthesia, multiple angiograms did not visualize the SCA aneurysm (Figure 3(h)). Therefore, the patient underwent conservative treatment. The treatment was ineffective and the patients died.
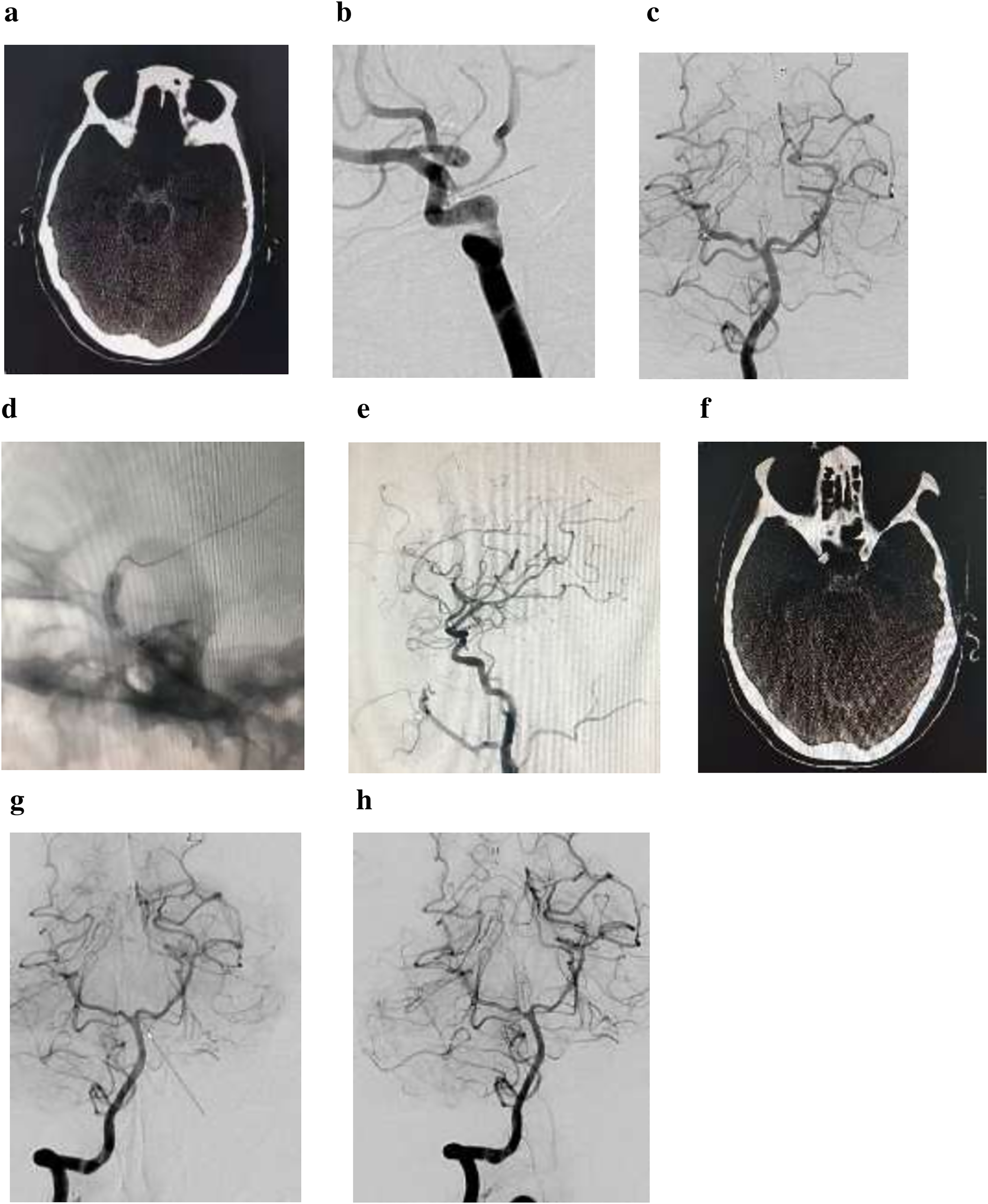
A 62-year-old female (patient No. 33) with a ruptured right ICA C6 tiny aneurysm who had suffered sudden headache for 7 h before admission.
Among the remaining 39 patients, 4 patients experienced non-lethal procedural complications. One patient with an unruptured right C2 saccular aneurysm (Patient No. 14) experienced ptosis and diplopia in the right eye 3 days post-operation, her doctor determined that it was probably due to compression of the ophthalmic nerve or the vagus nerve by thrombosis of the aneurysm, and put the patient under observation without additional treatment. The patient's symptoms improved substantially after 7 days. Another patient with an unruptured right C6 saccular aneurysm (Patients No. 29) experienced intra-operative hemorrhage and carotid cavernous fistulas (CCF) at C4 most likely due to arterial vascular lesion(s) caused by guiding catheter, guidewire, or balloon inflation during stent delivery into the tortuous PA. The patient's hemorrhage stopped after hemostasis treatment and she made good recovery. Her CCF was treated by ICA compression and disappeared at the 3-month follow-up. Contrast media extravasation was detected during roadmapping for Patient No. 17 (left ICA C6 BBA), indicating a ruptured BBA, therefore a Willis covered stent was implanted emergently, and the patients achieved immediate PA patency and complete aneurysm occlusion. Post-procedural Dyna CT indicated SAH, hydrocephalus and brain stem compression, the patient underwent symptomatic treatment, and made good recovery and was discharged. Finally, another patient with a left C4 aneurysm (Patient No. 37) developed asymptomatic CCF at C4 with minimal fistulous flow, the patient was managed conservatively and instructed to do regular follow-ups or visit whenever any new neurological symptom(s) occurred. None of the remaining 35 patients had any procedural complications (Tables 1 and 3).
Follow-up angiographic and clinical outcomes
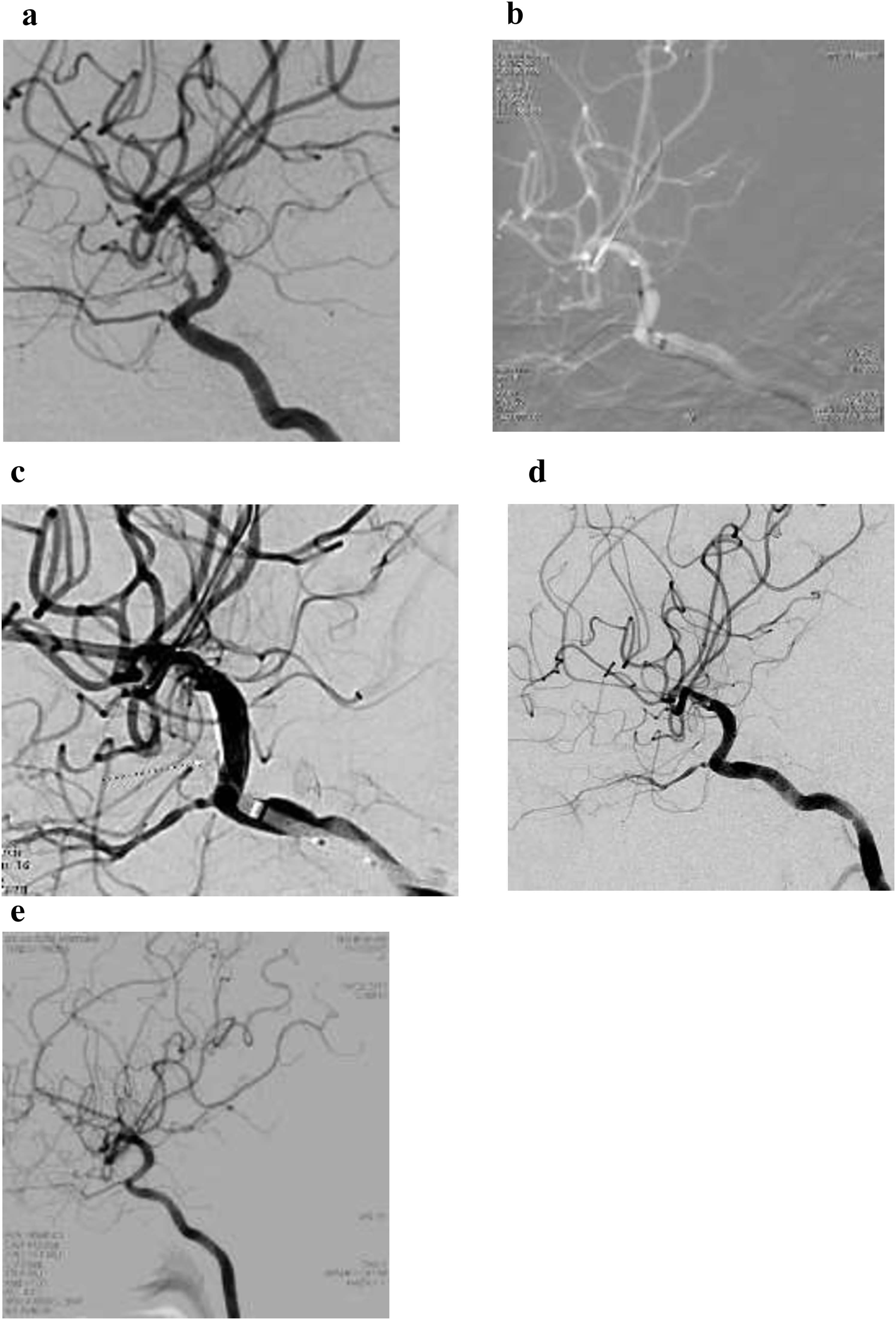
Of the 42 patients, 32 patients (33 aneurysms) had angiographic and clinical follow-ups, and their follow-up results were listed in Tables 1 and 3. The mean follow-up period was 8.8 ± 5.3 months (range 2–22 months). All 33 aneurysms had medium-term complete occlusion and there was no aneurysm recurrence. 3 of the 5 patients who had initial minimal endoleak were among these 32 patients, and all had spontaneous resolution of the endoleak and had complete aneurysm exclusion. Angiographs for 4 patients (Patient Nos: 5, 23, 24, 20) showed slight dilatation in the ICA ("swollen sails" phenomenon) due to slight expansion of the expandable polytetrafluoroethylene (ePTEE) membrane on which the blood inflow jet focused, as the membrane was only loosely sutured to the stent strut at several points (Figure 4). 16 Although such “swollen sails” phenomenon generally did not pose a threat, these patients were instructed to do regular follow-ups and to come back whenever new neurological symptom(s) occurred. Additionally, 30 of the 32 patients showed good PA patency, while 2 patients (Patient Nos. 4 and 17) had significant PA occlusion (>50% occlusion) due to in-stent stenosis. Neither patient was sure whether they strictly followed the dual-antiplatelet therapy. As both of them were asymptomatic, they were instructed to strictly follow the antiplatelet therapy and make regular follow-ups and to come back when new neurological deficits occurred.
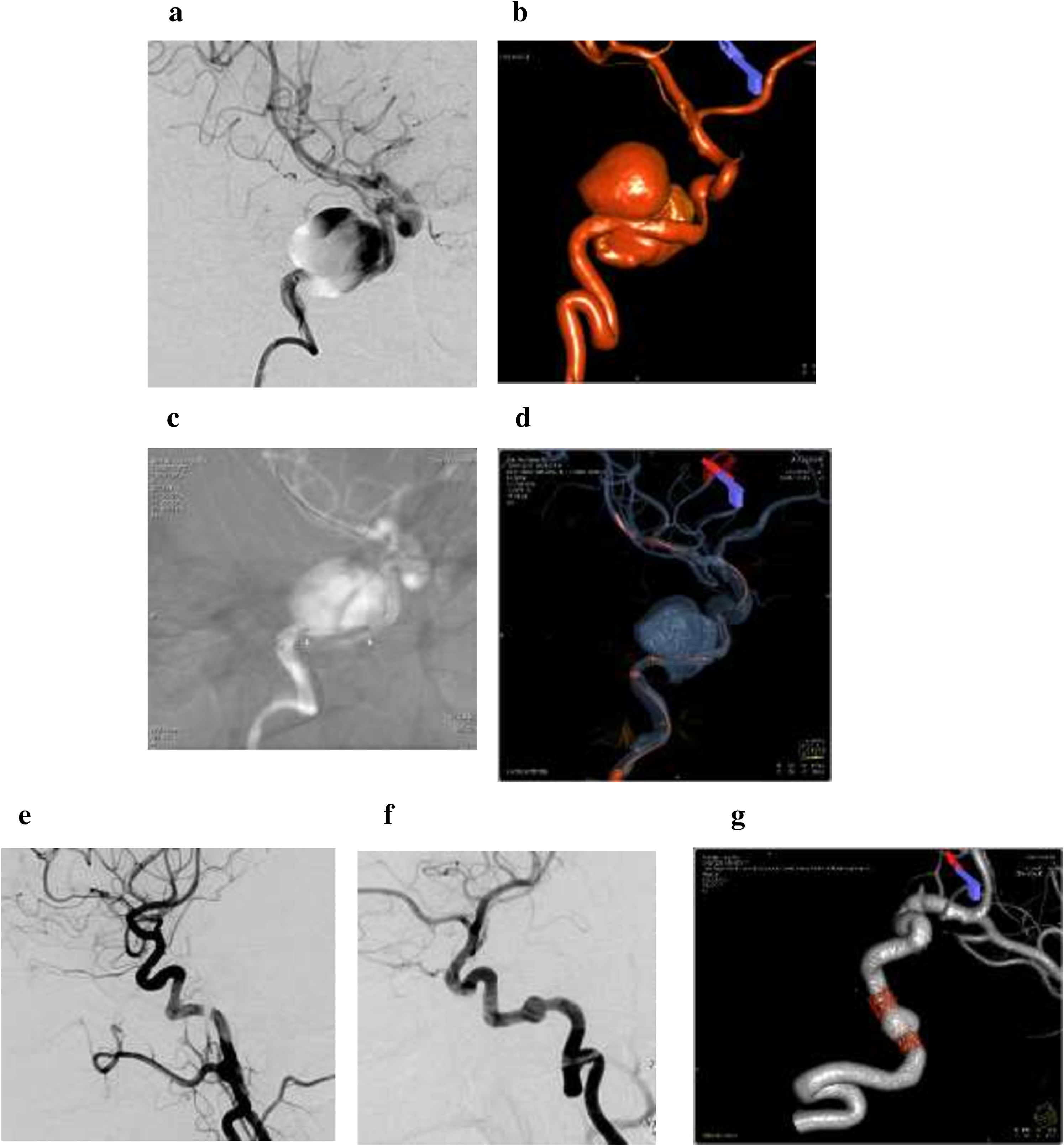
A 42-year old female (patient No. 5) with a right ICA C2 giant saccular aneurysm.
During the follow-up period, none of the 32 patients experienced any ischemic or hemorrhagic events. Their follow-up mRS was 0 in 31 patients and 1 in the remaining 1 patient. Additionally, the 1 patient with partial OA occlusion did not show any delayed related clinical symptoms. Finally, except for the 3 patients who died shortly after the procedure, all of the remaining 39 patients were alive during preparation of this manuscript according to telephone interviews.
The follow-up angiographic and clinical outcomes for the subgroups of the 30 patients with DICA aneurysms (31 aneurysms) and the 2 patients with VADAs (2 aneurysms) were summarized in Table 4.
Discussion
In this retrospective study, we examined the immediate and medium-term outcomes of 42 patients with DICA aneurysms or VADAs treated with the Willis covered stent at our institute and reached the following conclusions: for DICA aneurysms including saccular aneurysm, BBAs, dissecting aneurysms and pseudoaneurysms, using the Willis covered stent to immediately exclude the aneurysms is efficacious and safe in term of high rate of immediate aneurysm occlusion and PA patency, low rate of SB coverage, complications and relatively low rate of treatment-related mortalities. Additionally, medium-term follow-up results suggested that this approach had excellent durability as there was no aneurysm recurrence and low rate of significant PA occlusion due to in-stent stenosis. In addition, the Willis covered stent treated all of the 3 cases of VADAs in our study with complete success without any complications (Table 4), and 2 of the 3 patients with follow-ups had excellent medium-term outcomes.
Advantages and limitations of the Willis covered stent
Our study revealed that compared to surgical approaches and conventional endovascular approaches such as coil embolization, the Willis covered stent could produce better results. Surgical approaches are often problematic for DICA aneurysms and VADAs and carry the risk of intraoperative bleeding (up to 23%) and recurrence (up to 8.3%),2,4,5,15 and conventional endovascular approaches such as coil embolization has a relatively low immediate (35%-76.8%) and later complete occlusion rate (50.7–87.8%) and high aneurysmal recurrence rate (one third). 2 Meanwhile, our immediate complete aneurysm occlusion rate was 88.4% and medium-term complete occlusion rate reached 100% with no aneurysmal recurrence. Intra- or post-operative hemorrhage happened in 7.1% of the 42 patients included in our study. Therefore, consistent with previous reports,4,12,15,23 our study showed that endovascular treatment with the Willis covered stent has superior outcomes compared to surgical approaches as well as coil embolization.
According to our study and previous reports, compared to the traditional endovascular approaches, the Willis covered stent has the advantages of minimal risk of procedure-related aneurysm rupture or re-bleeding, no coil herniation, delayed migration or coil loop protrusion, maintenance of PA patency and low rate of PA stenosis, being relatively simple, fast and less expensive, reduced or eliminated mass effect caused by large or giant aneurysms, and no aneurysm recurrence or recanalization and very low rate of in-stent stenosis.2,14,15,23 On the other hand, despite the fact that the Willis covered stent was designed specifically for intracranial vasculature navigation, as a covered stent, it is still stiffer than a naked stent. Although the use of a supporter catheter such as Naiven greatly improves its ability to pass through the tortuous ICA, the Willis covered stent is still not flexible enough to fully comply with the tortuous configuration of the target artery and could lead to poor adherence to the vessel wall, additionally, there is a risk of the PA or distal branches being damaged during stent delivery.4,11,23
During the recent years, flow-diverting devices (FDDs) have been considered by many to be a breakthrough in treating cranial aneurysms. 24 Design-wise, FDDs have better flexibility than the Willis covered stent and therefore are easier to navigate, and both the Willis covered stent and FDDs carry the risk of SB occlusion. 9 According to a recent meta-analysis, the FDDs’ overall complete aneurysm occlusion rate was lowest (69.6%) less than 3 months after the procedure and could reach 90.8% more than 12 months after the procedure. 24 85.5% of the patients receiving the FDD treatment had a mRS of 0–2 and the remaining 10.7% of the patients had a mRS of 3–4. 24 The Willis covered stent could produce much higher immediate complete occlusion rate, in our case, 88.4%, and our medium-term complete occlusion rate was 100%. In addition, 31 out of the 32 patients with follow-ups in our study had a mRS of 0, and the remaining 1 had a mRS of 1, indicating a less severe long term neurological deficit. The same meta-analysis reported that FDDs’ associated mortality was 4.3%, 24 and another meta-analysis found that the rate of ischemic and hemorrhagic complications associated with FDDs in treating cranial aneurysms were 4.1% and 2.9%, respectively. 25 It also reported that neurological morbidity and mortality associated with FDDs were 3.5% and 3.4%, respectively. 2 Our study found that the rate of complications associated with the Willis covered stent in treating DICA aneurysms and VADAs was 14.3% (ischemic complications 2.4%, hemorrhagic complications 9.5%, neurological complications 2.4%) and that the rate of mortality was 4.8%. Compared to FDDs, besides being relatively simple, fast and less expensive, 23 the Willis covered stent has the additional advantages of being able to immediately exclude aneurysms from circulation2,4,8 and to reduce mass effect caused by large or giant aneurysms.2,15 FDDs were designed to facilitate the redirection of blood flow along longitudinal axis of the device and to reduce inflow and outflow of the aneurysm. Such a design can lead to blood stagnation and cause thrombosis within the aneurysm and aneurysm obliteration over time. 24 However, it also creates a “latent period” that could last weeks or even months, and during this period, there is a risk of aneurysm enlargement and re-bleeding especially considering the fact that these patients are on dual anti-platelet therapy. 9 In addition, when treating large or giant aneurysms with FDDs, large amount of coils were usually implanted, this would not reduce the initial mass effect and could potentially cause long term neurological complications.2,15,25 Meanwhile, as a covered stent, the Willis covered stent is still not flexible enough and is currently only used to treat ICA aneurysms and VA aneurysms with less tortuous PA.4,11,23 Additionally, it carries the risk of PA damage.4,9,11,23 In our experience, FDDs might be more suitable for treating unruptured aneurysms especially saccular aneurysms and dissecting aneurysms, while the Willis covered stent could be better suited for treating ruptured aneurysms especially BBAs. The Willis covered stent could also be especially suitable for treating traumatic aneurysms with or without epistaxis that need urgent interventions, as its design allows it to immediately exclude the traumatic aneurysms from circulation, maintain PA patency and treat vascular injury caused by trauma.2,21–23
Complications
Endoleak
In our study, 5 of the 42 patients (11.1%) experienced minimal endoleak. However, for the 3 patients who had medium-term follow-ups, their minimal endoleak disappeared at their follow-ups and their aneurysms were complete occluded.
Endoleak is most likely caused by incomplete occlusion of aneurysm orifice(s), a size mismatch between the stent and PA, the inhomogeneous nature of the blood vessel lumen, the aneurysm being located at a vessel segment that is acutely angled, a ruptured stent membrane, stent migration or transient vasospasm.4,9 It is important to select a covered stent with an adequate size. The deployed stent could also be re-inflated to eliminate endoleak with a pressure of 6–8 atmospheres for no more than 3 times. If endoleak persists after 3 re-inflations, a second stent could be implanted to cover the endoleak. In our experience, if a minor endoleak in a patient could not be immediately resolved by a second stent implantation and the angiograph immediately after the procedure revealed only slight aneurysmal filling, no further action is needed as thrombosis would occur over time to completely occlude the aneurysm. Of course, it is necessary for these patients to have follow-up angiographs to monitor the status of the endoleak and thrombosis in the aneurysm cavity, as there is potentially an increased risk of aneurysm rupture before it is completely occluded, especially in patients with acute SAH. Meanwhile, endoleak for BBAs was dangerous as it could potentially lead to increased pressure inside the BBAs and BBA rupture, and thus should be eliminated.
Other complications
A small number of patients in our study experienced other complications such as OA or AChA occlusion, in-stent stenosis, in-stent thrombosis, or intra-operative or post-operative hemorrhage (Table 1 and 3), all were well-documented and thoroughly discussed complications associated with the Willis covered stent.4,9,12,22,23,26,27 Additionally, 2 patients in our study experienced CCF at ICA C4 during the procedure. CCF after stenting is extremely rare. Only 1 case of CCF during treatment with the Willis covered stent has been reported. 28 CCF was most likely due to arterial vascular lesion(s) caused by guiding catheter, guidewire, or balloon inflation during stent delivery into the tortuous PA..28,29 The skills of the doctors performing the procedure are important in minimizing vascular injuries associated with stent delivery.
The “swollen sails” phenomenon
4 of the 32 patients (Patient Nos: 5, 23, 24, 20) who had medium-term follow-ups had what we called the “swollen sails” phenomenon. Angiographs of these 4 patients showed slight dilatation in the ICA (Figure 4), such dilatation was caused by slight expansion of the ePTEE membrane on which the blood inflow jet focused, as the membrane was only loosely sutured to the stent strut at the middle segment of the body to facilitate relative shift when stent is deployed in a curved vessel. 16 These patients were instructed to do regular checkups and to come back whenever new neurological symptom(s) occur, although such “swollen sails” phenomenon generally does not affect the stent's safety. There has only been one reported case of aneurysm recurrence due to partial isolation of the covering membrane from the stent body. 30 As there is a remote possibility that blood inflow jet could lead to partial isolation of the covering membrane from the stent body and cause aneurysm recurrence, it is especially important to have regular checkups for patients with the “swollen sails” phenomenon.
Limitation of the study
Our study has several limitations. First, our sample size is not large and thus the robustness of our finding is somewhat limited. Secondly, our study does not evaluate long-term outcomes of the Willis covered stent treatment. Finally, our study is not a controlled study, therefore the efficacy and safety of the Willis covered stent could not be directly compared with other treatments such as FDDs and coil embolization.
Conclusion
The Willis covered stent can be a safe and effective treatment for complex DICA aneurysms with excellent durability. In addition, the Willis covered stent treated all of the 3 cases of VADAs in our study with complete success without any complications, however, more cases are needed to further confirm its efficacy and safety in treating VADAs. Long-term studies and controlled studies are needed to further evaluate the safety, efficacy and durability of the Willis covered stent.
Supplemental Material
sj-docx-1-ine-10.1177_15910199211070900 - Supplemental material for Endovascular treatment of distal internal carotid artery aneurysms and vertebral artery dissecting aneurysms with the Willis covered stent: A single-center, retrospective study
Supplemental material, sj-docx-1-ine-10.1177_15910199211070900 for Endovascular treatment of distal internal carotid artery aneurysms and vertebral artery dissecting aneurysms with the Willis covered stent: A single-center, retrospective study by Yu Wu, Jia Yu, Tao Zhang, Jian-Ping Deng and Zhenwei Zhao in Interventional Neuroradiology
Footnotes
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Xxxxxxx.This study was funded by MicroPort, Shanghai, China. The funder did not play any role in the study design or conduction, data collection, analysis or interpretation, nor did it play any role in writing of this manuscript or the decision to submit the article for publication. The authors declare that they have no other conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the MicroPort, Shanghai, China
Ethical approval
This study was approved by the ethics committee of Tangdu Hospital, Air Force Medical University (The Fourth Military Medical University).
Authors’ contributions
YW, JY and ZZ conceived and designed the study. YW, JY, TZ and JPD acquired, collected, analysed and interpreted the study data. All authors have drafted the work or substantively revised it, have approved the version to be published; and have participated sufficiently in the work to take public responsibility for appropriate portions of the content.
Availability of data and materials
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.