
Abstract
Introduction
Mural type vein of Galen malformation (mVOGM) is characterized by direct, high flow anastomoses between feeding arteries and the median prosencephalic vein of Markowski.1,2 This feature poses challenges to depositing embolic material at a favorable location near the arteriovenous shunt. Several adjunctive methods have been described, including induced hypotension or asystole, balloon-assisted flow control, and creation of a coil basket.3–5 Each has advantages and shortcomings which depend much on the particular scenario involved.
Rapid ventricular pacing (RVP) has been proposed as an alternative strategy for reducing blood flow more predictably and significantly than induced hypotension, without complex endovascular maneuvers.6,7 RVP has been utilized in other pediatric transcatheter procedures including balloon aortic valvuloplasty8,9 and stenting of coarctation of the aorta. 10 The right ventricle is catheterized and a pacing catheter is connected to a temporary external pacemaker. Prior to embolization, rapid ventricular pacing is initiated to lower cardiac output. Following embolization, pacing is discontinued, and the heart returns to sinus rhythm.
We report a single center case series in which five patients aged two weeks to four years underwent ten mVOGM embolizations in which RVP was utilized twenty-six times. RVP predictably reduced cardiac output, enabling precise deposition of nBCA near the arteriovenous shunt. No RVP-associated complications occurred.
Materials and methods
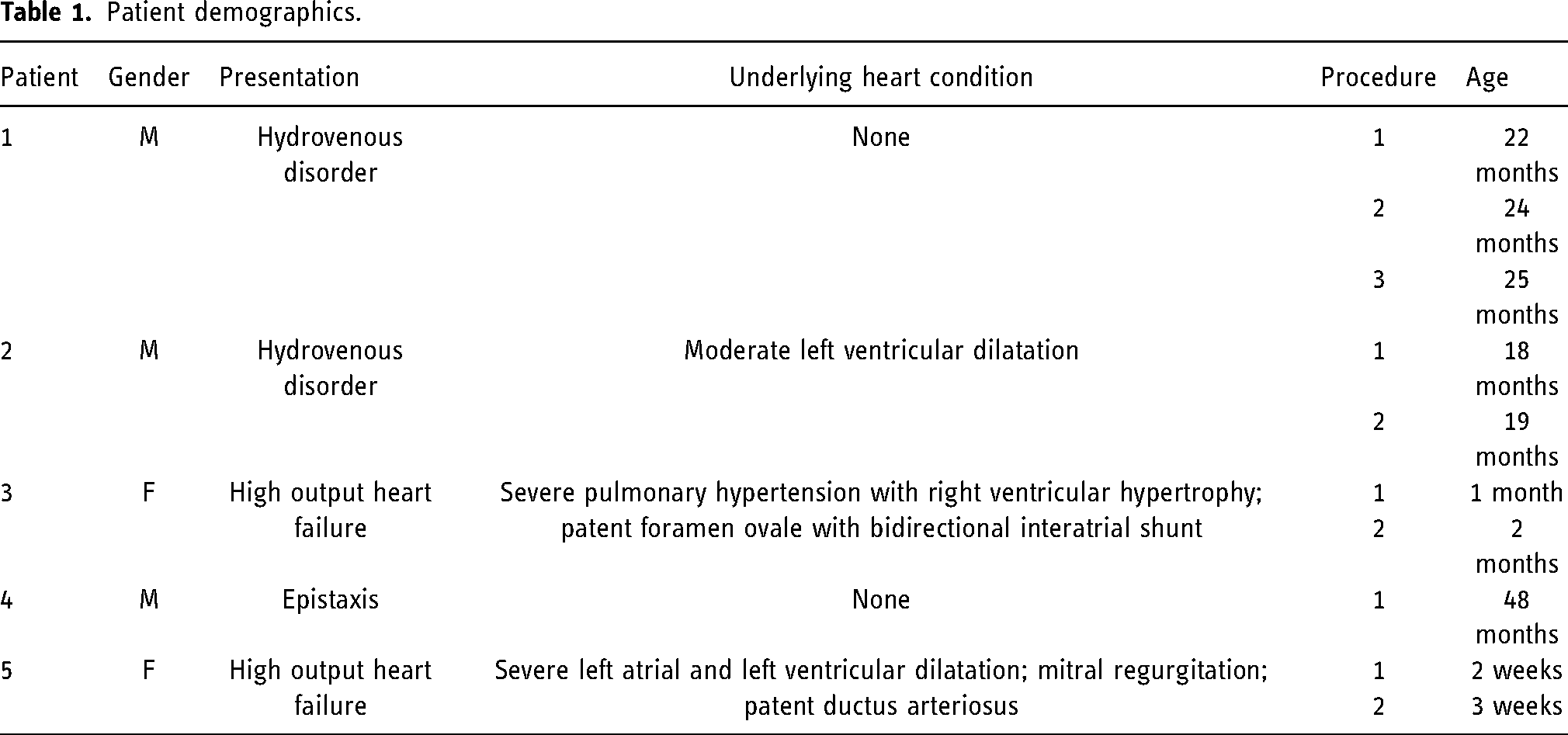
Following IRB approval, data on all mVOGM embolizations utilizing RVP at our institution were collected. Date range was 4/2020 through 7/2021. Five patients were identified; accounting for multiple procedures, RVP was utilized in ten cases (Table 1). Demographics, pacing parameters, embolization technique and outcomes were determined through retrospective electronic medical chart review. Cardiac evaluation revealed high output heart failure in two neonates, one of whom also suffered from severe pulmonary hypertension. One toddler was known to have left ventricular dilatation from high cardiac output. No other heart comorbidities were identified.
Patient demographics.
Pacing procedure
All patient’s families provided two separate written consents prior to the procedure. The first consent for embolization of the vein of Galen malformation was obtained by the interventional neuroradiologist The second consent, obtained by the cardiologist, detailed the placement of the temporary pacing catheter and rapid ventricular pacing. Specifically, the family was counseled on the risk of vascular injury, perforation of the myocardium, and ventricular dysrhythmia requiring defibrillation. Families were counseled that rapid ventricular pacing would be used if attempts with the standard embolization approach were predicted to be unsuccessful. During patient preparation in all cases, defibrillation pads were applied to the chest to prepare for the possibility of ventricular dysrhythmia requiring defibrillation. Venous access was obtained via modified Seldinger technique under ultrasound guidance. A 4-French, fixed-curve quadripolar pacing catheter (Boston Scientific Corporation, Marlborough, MA) was introduced into the right internal jugular vein in toddlers or the right femoral vein in neonates and advanced to the right ventricle under fluoroscopic guidance (Table 2). For the first case, a 5-French, balloon-tip, flow-directed bipolar pacing catheter (St Jude Medical, Minnetonka, MN) was used. The 4-French catheter was used in all subsequent cases. The pacing catheter was connected to the atrial channel of a temporary external pacemaker (Oscor, Palm Harbor, FL) to allow for a greater range of rapid pacing programmability. Following catheter positioning, test ventricular pacing was performed at 160–200 beats per minute (bpm) to ensure ventricular capture. Rapid ventricular pacing was not used universally. The choice to use rapid ventricular pacing during embolization was made by the interventional neuroradiologist immediately prior to embolization based on anatomic and flow characteristics of the pedicle. Prior to embolization, RVP was initiated at 240 bpm and incrementally increased by 10 bpm to 240–280 BPM with 1:1 capture until achieving the desired drop in cardiac output based on end-tidal CO2 (etCO2) and mean arterial blood pressure (Table 2). Liquid embolic was infused once etCO2 reached a steady state. RVP was performed throughout nBCA infusion and until the cerebral microcatheter was withdrawn, a duration of 40–60 s. With cessation of pacing, each patient returned to sinus rhythm with normalization of mean arterial blood pressure and end-tidal CO2. No dysrhythmias were induced. There were no complications related to ventricular pacing catheter placement.
Rapid ventricular pacing parameters.
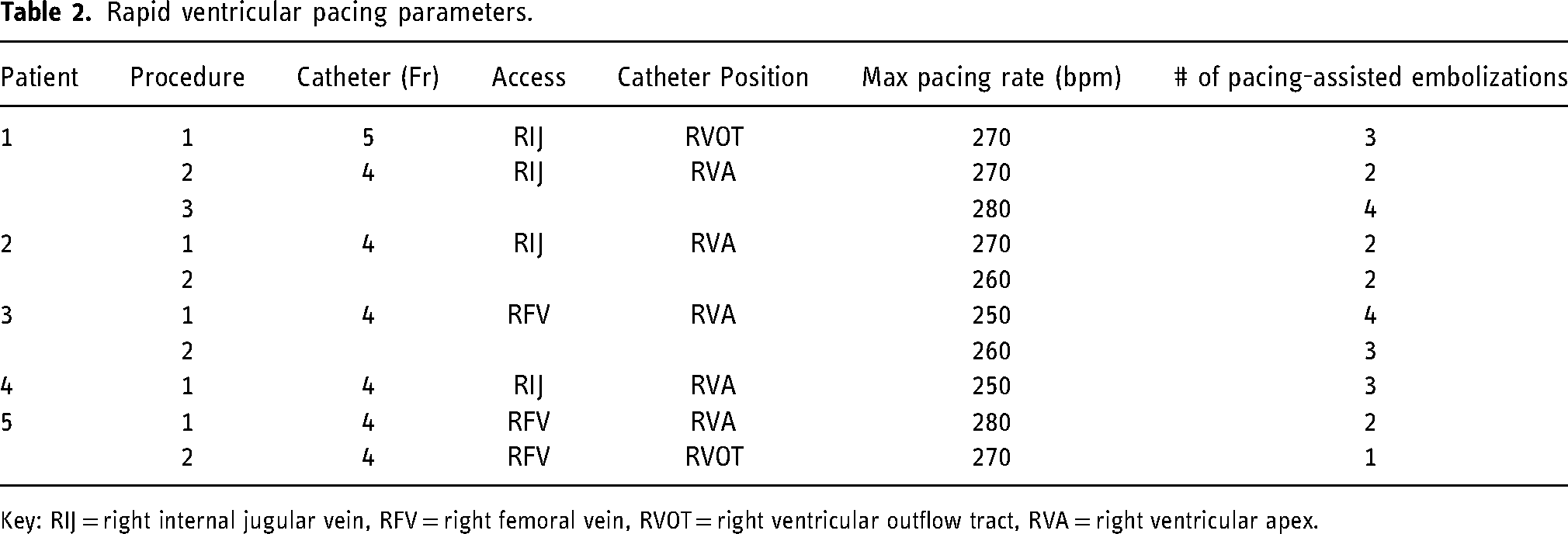
Key: RIJ = right internal jugular vein, RFV = right femoral vein, RVOT = right ventricular outflow tract, RVA = right ventricular apex.
Embolization technique
All procedures involved trans-arterial deposition of liquid embolic as close to the fistulous point as feasible given variability in microcatheter access and pedicle size: tortuous anatomy occasionally limited navigation to the shunting point, and sufficient length beyond the catheter tip was required to ensure polymerization proximal to (or bridging) the venous side. nBCA (Cerenovus, Irvine, CA) was used in nine cases and Onyx (Medtronic, Irvine, CA) in one case (patient 5). Once optimal catheter position was confirmed by angiography, provocative testing was performed with lidocaine and methohexital in conjunction with intra-operative monitoring (EEG, MEP and SSEP). In the two neonatal cases total intravenous anesthesia was not feasible, precluding this step. As the microcatheter was flushed with D5 dextrose or DMSO, the cardiologist initiated RVP and signaled when cardiac output had sufficiently reduced. Liquid embolic was then immediately infused. Once the cast appeared stable by fluoroscopy, RVP was discontinued. The procedure was repeated for each pedicle embolized.
Results
Ventricular capture was achieved in all instances. Subsequent rapid ventricular pacing resulted in a significant decrease in EtCO2 of 25–40%, indicating reduction in cardiac output. Patients tolerated RVP well and no instances of ventricular tachycardia or ventricular fibrillation occurred. Once RVP ceased, EtCO2 returned to baseline over 10 to 15 s. In neonates presenting with heart failure, Patient 5 experienced normalization of brain natriuretic peptide and was discharged home. Patient 3 experienced normalization of the jugular/systemic O2 gradient and aortic flow reversal; however, pulmonary hypertension since birth was refractory to medical and interventional treatment. This patient expired from right heart failure at two months of age.
Casting the arterial pedicle with nBCA immediately adjacent to, or traversing, the fistulous point was achieved in 9/10 cases (Figures 1 and 2). A glue cast (1:0.5 nBCA:Lipiodol) initially formed in the target pedicle of Patient 5 but subsequently embolized a few seconds later, resulting in non-occlusive deposition within the left transverse sinus as well as occlusion of a subsegmental pulmonary artery without clinical sequelae. Coils were subsequently deployed within the venous pouch to serve as a basket and successful trans-arterial embolization was then performed with Onyx 34 using a Scepter XC balloon microcatheter (Microvention, Aliso Viejo, CA) in conjunction with RVP to allow for a more gradual injection.

A: patient 1. Microcatheter angiogram in frontal oblique projection demonstrates a mural-type right posterior choroidal artery feeding pedicle (arrow) joining the prosencephalic vein of Markowski (arrowhead). Adequate caliber and lack of significant tortuosity favored balloon microcatheter placement for flow control. Figure 1B: Balloon microcatheter angiogram of the right posterior choroidal artery feeding pedicle shown in Figure 1A. This pedicle was subsequently embolized with Onyx. Figure 1C: Microcatheter angiogram in lateral projection demonstrates a high flow left posterior lateral choroidal pedicle (same patient as Figures 1A, 1B). Prior Onyx cast is present (triangle). Although the pedicle feeds into a choroidal network (arrowhead), it was necessary to embolize from a position distal to the thalamoperforator (arrow) which could not be reached with a balloon microcatheter. Figure 1D: Microcatheter angiogram in the same pedicle as Figure 1C, distal to thalamoperforator. Initial n-BCA cast traversed the choroidal network into the recipient vein. The injection was terminated and repeated with RVP upon re-catheterization. Figure 1E: Left vertebral artery angiograms in frontal projection before (Left) and after (Right) RVP assisted embolization of the left posterior lateral choroidal pedicle (arrow). Glue cast (arrowhead) is positioned near the arteriovenous shunt.

A: patient 2. Right internal carotid artery angiogram demonstrates a mural type posterior choroidal artery feeding pedicle to the prosencephalic vein of Markowski. Figure 2B: Roadmap of image in Figure 2A with balloon microcatheter inflated in the feeding pedicle. Despite balloon inflation, Onyx traversed the arteriovenous shunt and formed a non-obstructive plug in the torcula. More aggressive balloon inflation was felt unsafe given the consequences of perforating a high flow vessel. There was also concern that even complete flow arrest would not reduce the Venturi effect from other shunting pedicles. Figure 2C: Post-embolization right internal carotid artery angiogram following re-catheterization of the posterior choroidal artery pedicle and embolization with 75% n-BCA under RVP. Rather than attempt further Onyx injection with RVP, a concentrate glue was felt to provide quicker polymerization. The microcatheter was withdrawn once glue began to reflux, yet the embolization (arrowhead) is sub-occlusive. Subtraction artifact from prior distalized Onyx plug is noted in the torcula (arrow). Figure 2D: Follow-up right internal carotid artery angiogram one month later demonstrates spontaneous occlusion of the posterior choroidal artery feeding pedicle from Figure 2B and 2C. Four vessel angiography demonstrated no residual arteriovenous shunting, consistent with angiographic cure of the VOGM.
No new clinically evident ischemic infarcts were identified. One patient was slow to emerge from anesthesia and a head CT revealed acute subdural hemorrhage into ex vacuo dilation adjacent to encephalomalacia. No intra-operative complications were apparent to explain this finding, although the patient did receive routine systemic heparinization (60 Units/kg loading dose and 12 Units/kg maintenance dose hourly). The neonate returned to her neurologic baseline over several hours and the hematoma was managed expectantly.
Discussion
This report describes the largest case series utilizing RVP in mVOGM, including both neonatal patients in acute heart failure as well as young children presenting with hydrovenous disorder. Difficulties encountered while embolizing mVOGM using pure glue, Onyx delivered with balloon microcatheter inflation, and systemic hypotension with intravenous nitroprusside and/or adenosine motived us to explore RVP. Nevertheless, each flow control technique possesses advantages and disadvantages that depend much on the specific clinical scenario. Others have reported success with a combined transarterial and transvenous approach. 11 We reserve RVP for high flow pedicles that we anticipate to be, or have proven, challenging for simpler strategies; it represented 45% of all VOGM embolizations performed during the study period.
The technique appears safe and well tolerated. Complementary interventional cardiology experience with RVP in the setting of heart failure and structural defects, such as aortic stenosis and coarctation of the aorta, has demonstrated very low incidence of ventricular fibrillation.8–10 Patients with VOGM face unique physiology in the form of significant arteriovenous shunt resulting in high cardiac output heart failure. The high-output state affects both the right and left ventricles and is a different physiologic substrate compared to critical aortic stenosis or coarctation of the aorta, in which high afterload to the left ventricle often results in systolic dysfunction and shock. Patients with VOGM typically have ventricular dilatation with preserved systolic function, though also represent a high-risk group.
Hockley et al. 6 describe several challenges encountered with rapid ventricular pacing for VOGM embolization, including catheter dislodgement, loss of capture, 2:1 ventricular capture, and induced ventricular fibrillation. We have not experienced ventricular dysrhythmias. During the first procedure, 2:1 capture was encountered during the initial trial at RVP prior to embolization. By starting at a slower pacing rate and increasing the paced rate incrementally, the problem was overcome. This technique became our standard protocol.
We have experienced loss of capture requiring catheter repositioning during the procedure. While Hockley et al. used a temporary pacing catheter equipped with active fixation, this particular catheter is no longer available in the United States. Our experience to date indicates that by using fluoroscopy, standard bipolar or quadripolar pacing catheters can be positioned safely and securely. Given the high blood flow in mVOGM, ensuring a drop in cardiac output with resultant decreased flow through the lesion prior to embolization is important to achieving cast formation in the targeted pedicle.
End-tidal CO2 monitoring is a reliable, non-invasive tool that correlates with cardiac output.12,13 So long as CO2 production and ventilation are constant, decrease in etCO2 reflects decrease in cardiac output.12–14 Experimental animal models of cardiac arrest and resuscitation found a linear relationship in etCO2 and cardiac output.12,13 A subsequent animal study that included evaluation of supernormal cardiac output in addition to normal and low cardiac output found a logarithmic relationship between etCO2 and cardiac output. 15 EtCO2 monitoring to estimate cardiac output is used during cardiac surgery,14,16,17 volume resuscitation in shock, 18 and cardiopulmonary resuscitation during cardiac arrest. 19 As endotracheal intubation is routinely performed for embolization, etCO2 provides an alternative method to trend cardiac output though is not a replacement for accurate determination of cardiac output such as thermodilution or calculation by the Fick method. In our experience, a drop in etCO2 occurs within 2–3 breaths after RVP initiation and reaches steady state within approximately 5 breaths.
While differences in embolic behavior in the presence of RVP cannot be directly compared to its absence, the ability to achieve an arterial cast near (or bridging) the fistulous point in 9/10 cases attests to its utility. Nevertheless, torrential flow within mVOGM shunts must not be underestimated and despite RVP, we did encounter distal embolization once. For this emergent case, the pediatric cardiologist/electrophysiologist (AK) who had performed the first eight pacing procedures was unavailable, so pediatric cardiologists who lacked mVOGM RVP experience performed the pacing. Rather than awaiting verbal confirmation from the interventionalist that a stable glue cast had been achieved, pacing was prematurely discontinued. This underscores the importance of working with a consistent team well versed in critical timing and communication as there is a learning curve in mastering the technique. When catheter access to the shunt is feasible, a high nBCA concentration is still indicated as cardiac output is reduced, but not eliminated. In situations where distal access is not possible, RVP allows for a more dilute nBCA concentration to be slowly injected, penetrating further towards the fistulous point.
Conclusion
Rapid ventricular pacing appears to be a safe and well tolerated technique that facilitates transarterial embolization in mural type vein of Galen malformations for select pediatric patients who are not amenable to standard flow control techniques. Future studies are warranted to justify the routine use of this adjunctive procedure.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.