
Abstract
Type II endoleak after endovascular aortic aneurysm repair still remains the Achilles’ heel of the treatment, the source of which regularly is difficult to identify and treat. We present a patient with a persistent type II endoleak associated with a continuous aneurysm sac expansion after endovascular aortic aneurysm repair for which many diagnostic modalities were used during his follow-up such as duplex scan, computed tomography angiography and magnetic resonance angiography. Attempts were undertaken to treat the source of endoleak including coil micro-embolisation of lumbar arteries and subsequent open ligation of the inferior mesenteric artery, but they failed to eliminate the endoleak. Finally, a middle sacral artery was identified as the source of the endoleak. At that time, the patient was subjected to surgery for sigmoid carcinoma, and simultaneously, a ligation of the sacral artery was undertaken which eventually eliminated the endoleak completely. This case highlights that type II endoleak may be evoked by various sources and there can be a great difficulty to identify these feeding vessels; thus, careful planning for its management is mandatory.
Introduction
Endovascular aortic aneurysm repair (EVAR) has been established as the treatment of choice for abdominal aortic aneurysm in many vascular centres instead of the traditional open repair.1–5 However, type II endoleak remains the Achilles’ heel of this treatment, 6 and lifelong imaging surveillance is mandatory.7–10 We present herein such a case in order to highlight the difficulties we encountered to identify the sources of a persistent type II endoleak and the challenges we faced to eliminate it.
Case report
We present a case of a 71-year-old male patient who underwent an EVAR under regional anaesthesia using a Medtronic Talent® bifurcated stent graft. During his completion of angiography, the aneurysm sac was successfully excluded, and there were no signs of any type of endoleak. He was discharged on the fourth post-operative day. As per protocol,
11
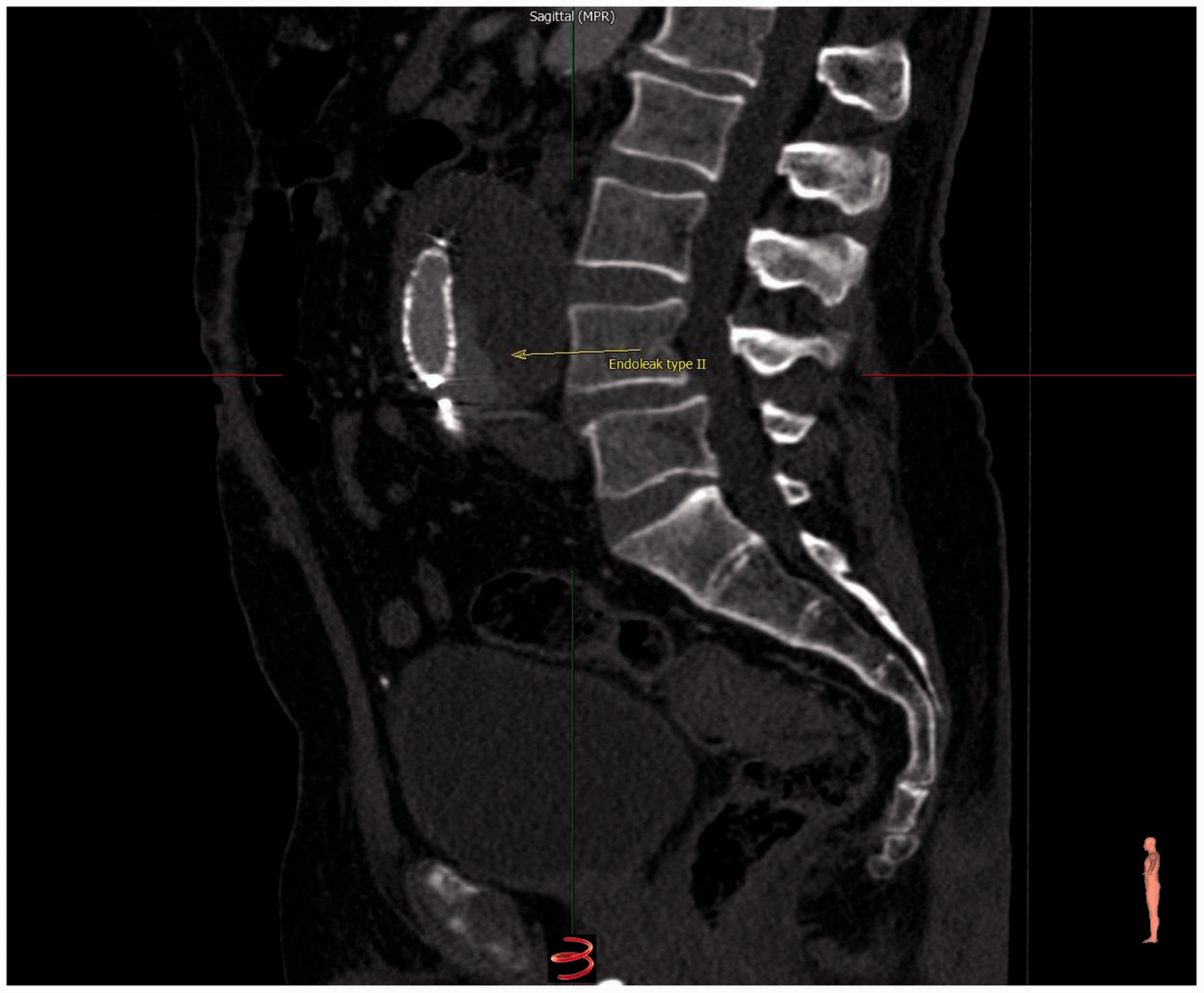
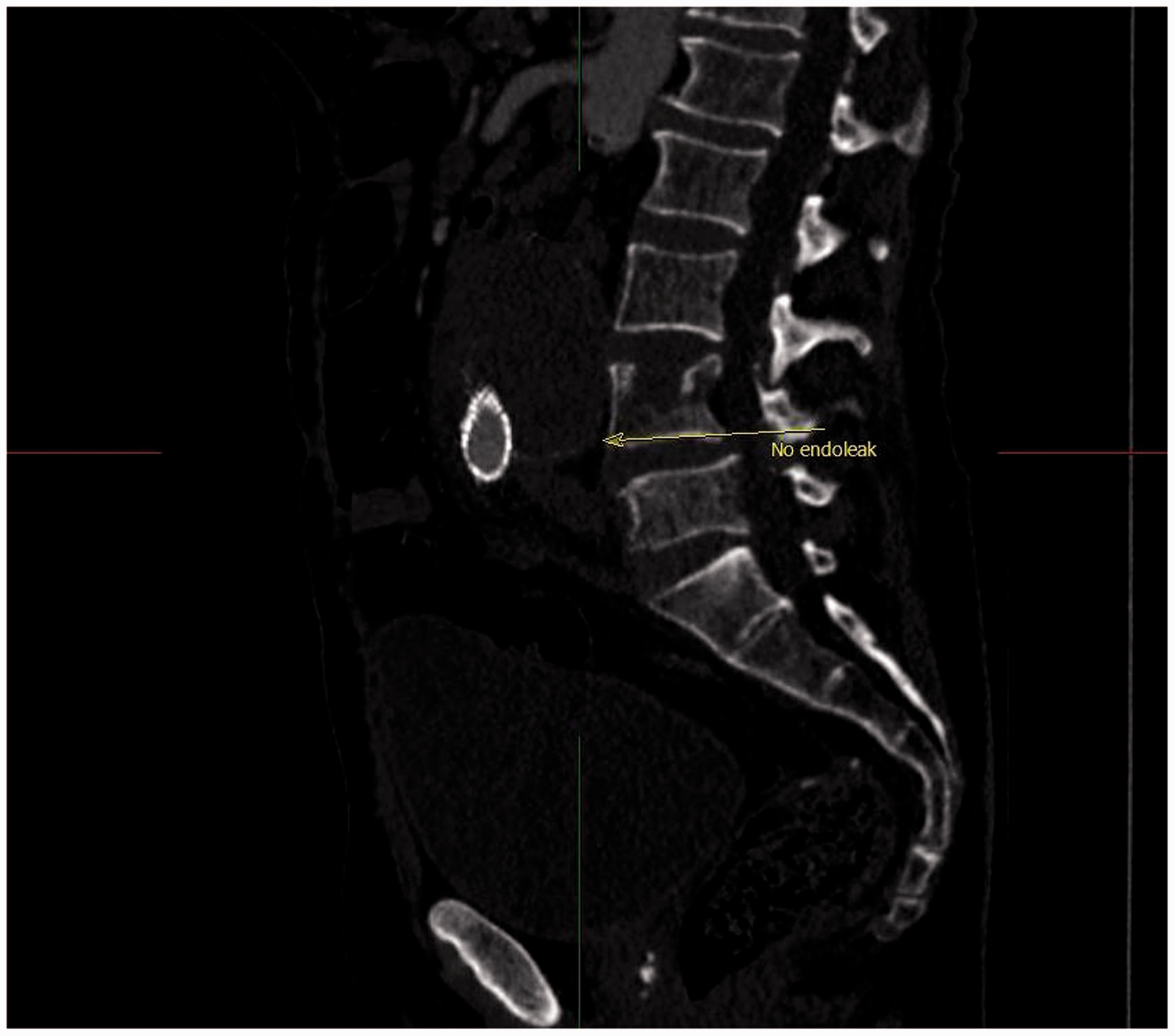
he was subjected to computed tomography angiography (CTA) in various phases of contrast-enhanced scans. On the first post-EVAR month CTA, a small type II endoleak with no changes in sac diameter was demonstrated and the same result was demonstrated in magnetic resonance angiogram after three months. On the six-month CT scan, type II endoleak was still present, but a 4-mm increase of the sac diameter was concurrent. At that time, micro-coil embolisation of the lumbar arteries was undertaken (Figure 1). However, a month later, the endoleak was still present on duplex scan and observation was decided. At first year post-EVAR CTA, the endoleak still persisted (Figure 2) and it was attributed to a patent inferior mesenteric artery (IMA) that was ligated through a midline laparotomy. The aneurismal sac was not open because no other sources of endoleak were identified in the imaging investigations. One month later, the type II endoleak was still apparent and observation was decided. On the second year post-op CT scan, the sac diameter showed further increase by 17 mm. On examination, the source of the endoleak was apparently a patent middle sacral artery, and in the same examination, an incidental sigmoid-colon mass was discovered. During the surgery for colorectal resection, the middle sacral artery was directly ligated leading to complete elimination of the type II endoleak as confirmed on CT scan one month after surgery (Figure 3).
Six-month follow-up computed tomography angiogram 3D reconstruction micro-coils embolisation (yellow arrow) and type II endoleak (red arrow). One-year follow-up computed tomography angiogram with type II endoleak (yellow arrow). Computed tomography angiogram after ligation of middle sacral artery follow-up with no endoleak (yellow arrow).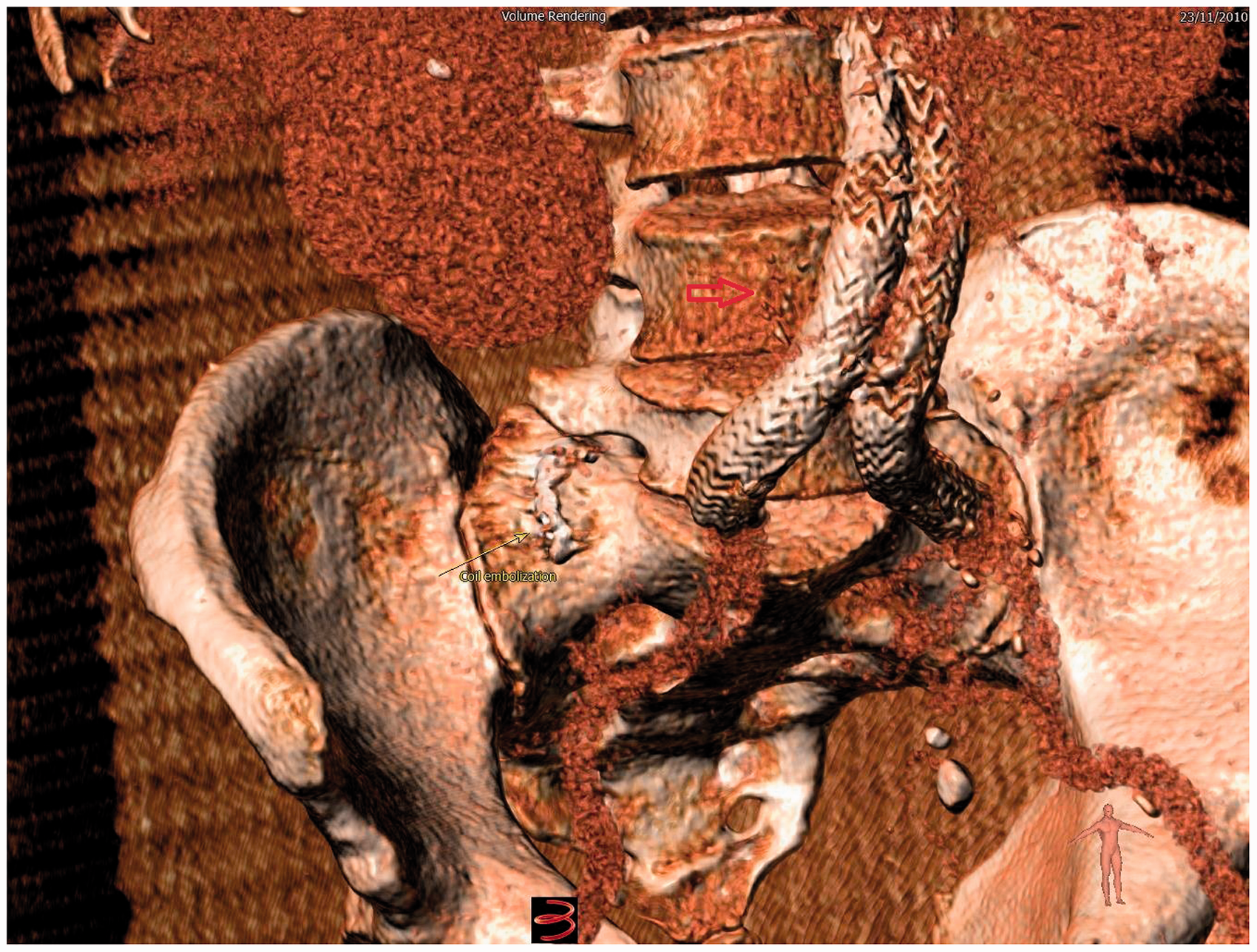
Discussion
In most of the cases, isolated type II endoleak is considered as innocuous and it is expected to seal spontaneously or it is not associated with high risk of rupture.12–14 However, this has been questioned from other researchers,15–17 and it has been recommended that in the presence of a type II endoleak and significant sac enlargement, the risk of rupture may be substantial 15 ; thus, sac enlargement is currently the best surrogate available and guides the indication for intervention. 18
As it was highlighted in our case, it is really important to anticipate that treatment of a feeding artery may be not successful, as other feeding arteries may be responsible too or will appear as a result of blood flow redistribution.9,19 Thus, although we embolised the lumbar arteries at first, we had to ligate the IMA secondly and the middle sacral artery later. However, only the preoperative embolisation of the IMA (according to specific criteria) has been associated with reduced incidence of type II endoleak and aneurysm sac volume enlargement.10,19 On the other hand, in contrast to the secondary endovascular procedures, there are devotees who suggest elective open surgery after EVAR in order to eliminate an isolated type endoleak II with good results20,21 or even conservative treatment as an effective strategy for the management of type II endoleak with equivalent aneurysm-related mortality and an improved survival.12–14,22,23
Conclusion
Our case highlights the difficulty to accurately identify and confirm the sources of type II endoleak and to instigate the appropriate treatment for its elimination. Utilization of various imaging modalities in the follow-up, and close observations are required for the management of cases of persistent type II endoleak.
Footnotes
Authors’ Note
Although identifying information, including patient’s name, his initials, or his hospital number, was not published in the manuscript and in the photographs, as it is recommended by the International Committee of Medical Journal Editors, Uniform Requirements for Manuscripts Submitted to Biomedical Journals, a patient’s consent was obtained.
Conflict of interest
None declared.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.