
Abstract
Background
Thoracic aortic aneurysm rupture is often a fatal condition. Emergent thoracic endovascular aortic repair (TEVAR) has emerged as a suitable treatment option. Unfortunately, respiratory complications from hemothorax continue to be an important cause of morbidity and mortality even after successful management of the aortic rupture. We hypothesize that early hemothorax decompression after TEVAR for ruptured aneurysms decreases the rate of postoperative respiratory complications.
Methods
Single-center, retrospective eight-year review of ruptured thoracic aneurysms treated with TEVAR.
Results
Seventeen patients presented with ruptured degenerative thoracic aortic aneurysms, all of which were successfully treated emergently with TEVAR. The mean age was 74 years among the 12 (70.6%) men and 5 (29.4%) women treated. Inpatient and 30-day mortality rates for the entire cohort were both 17.6% (three patients). The 90-day mortality rate was 47.1% (eight patients). Thirty-day morbidities of the entire cohort included stroke (n = 1, 5.9%), spinal cord ischemia (n = 3, 17.6%; only one was temporary), cardiac arrest (n = 4, 23.5%; 3 were fatal), respiratory failure (n = 5, 29.4%), and renal failure (n = 5, 29.4%). A large hemothorax was identified in the majority of patients (n = 14, 82.4%). While six (42.9% of 14) patients had immediate chest tube decompression on the day of index procedure, three (21.4% of 14) patients had decompression on postoperative day 1, 4, and 7, respectively. Although not statistically significant, there were trends toward higher rates of respiratory failure (50.0% vs. 16.7%, P = 0.198) and 90-day mortality (62.5% vs. 33.3%, P = 0.280) for patients with delayed or no hemothorax decompression when compared to patients with immediate hemothorax decompression.
Conclusions
The morbidity and mortality of ruptured degenerative thoracic aortic aneurysms remains high despite the introduction of TEVAR. In this single-center experience, there was a trend toward decreased respiratory complications and increased survival with early chest decompression of hemothorax after TEVAR.
Introduction
Thoracic aortic aneurysm rupture is often a fatal condition that requires emergent treatment if the patient survives the initial presentation. Traditionally, the treatment involves open surgical repair, which has been associated with disconcertingly high mortality and morbidity rates.1–3 With the introduction of endovascular technique and endograft technology, thoracic endovascular aortic repair (TEVAR; Figure 1) has become the treatment of choice for non-emergent and some emergent thoracic aortic pathologies including ruptured thoracic aortic aneurysms (rTAA).4–6
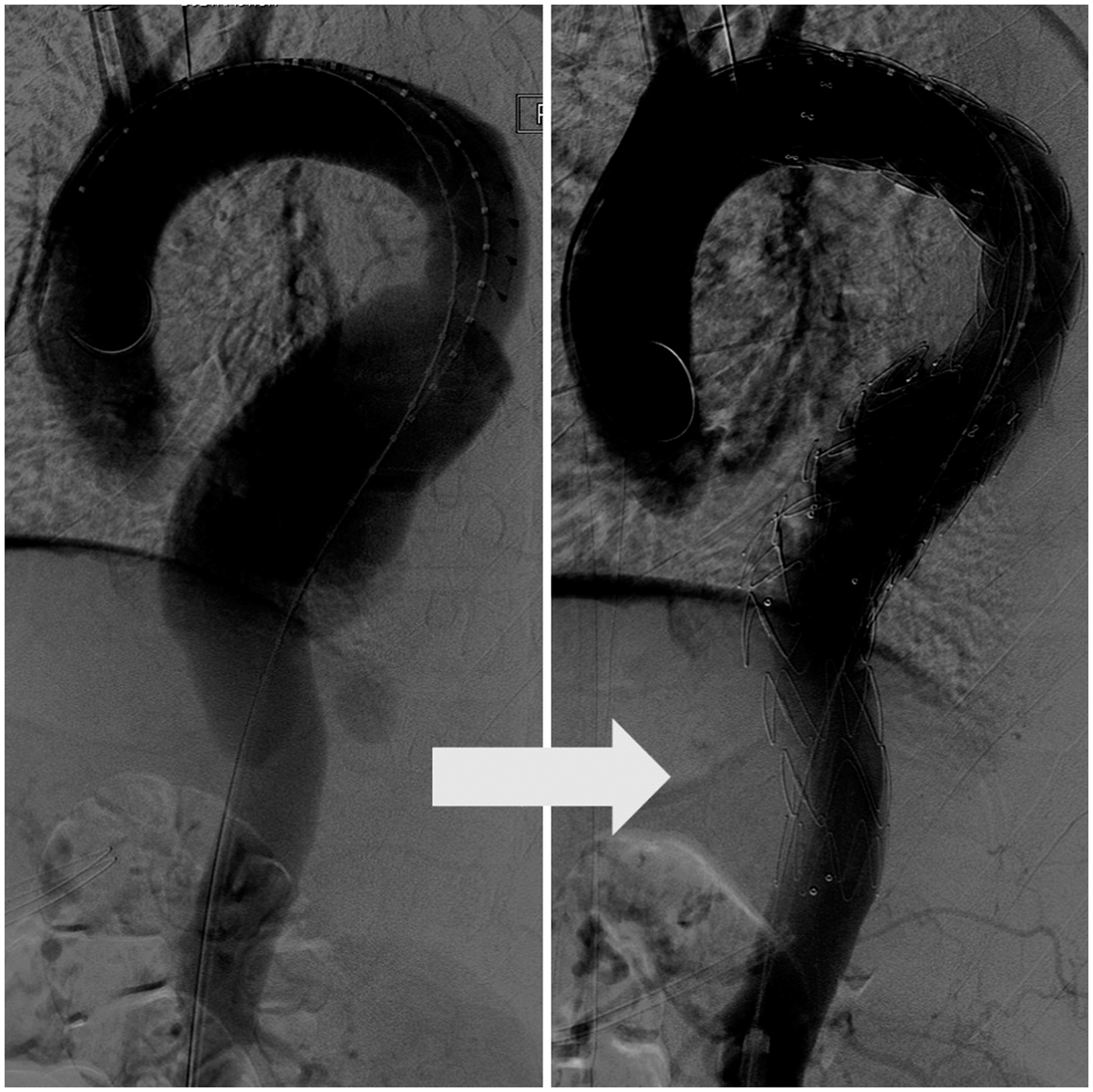
Thoracic endovascular aortic repair (TEVAR) for ruptured thoracic aortic aneurysms (rTAA), before and after.
As with endovascular repair of abdominal aortic aneurysm, some experts have preferred TEVAR over open surgical repair of rTAA. In a study by Minami et al. 7 , TEVAR has a success rate of over 90%. However, others have suggested that TEVAR for rTAA still carries a significant mortality and morbidity risk including cardiac, neurologic, and renal complications.8,9 At our institution, we have noted that respiratory complications from hemothorax continue to be an important cause of morbidity and mortality even after successful treatment of the aortic rupture.
In order for us to ensure the continued efficacy of TEVAR for rTAA, we need to study our management of hemothorax in the presence of rTAA. We hypothesize that early hemothorax decompression after TEVAR for ruptured aneurysms decreases the rate of postoperative respiratory complications and increases rate of survival.
Methods
Patient cohort
We performed a single institution retrospective chart review of all adult (≥18 years old) patients who underwent TEVAR for rTAA from 1 July 2004 to 30 June 2012. Patients who underwent open surgical repair, had an acute aortic dissection, or died prior to repair were excluded from the study. The study was approved by our Institutional Review Board.
Patient demographics such as age, sex, race, and comorbidities were identified through chart review. Being a tertiary medical center, transferring status was also of interest. Anesthesia type, access, devices, and concurrent procedures were obtained from operative reports and nursing records. Postoperative course including morbidities, mortalities, and discharge dispositions were examined using patient records and Social Security Death Index.
Hemothorax: Immediate vs. delayed or no decompression
Presence of hemothorax prior to TEVAR was identified per preoperative computed tomography (CT) imaging and hemothorax thickness was measured in the transverse plane. Previous parameters described by Piffaretti 10 were used to categorize hemothoraces by size, which included: < 2 cm, between 2 and 3 cm, or >3 cm. Patients who underwent TEVAR for rTAA but did not have a hemothorax were not included in the final analysis. Patients who underwent hemothorax decompression with chest tube thoracostomy on the day of TEVAR were categorized as “immediate decompression.” Respiratory complications and mortalities were examined among patients who had “immediate decompression” as compared to those who had “delayed or no decompression”. Respiratory failure was defined as any unplanned reintubation or prolonged intubation (greater than 48 h).
Statistical analysis
Categorical variables (frequencies) were compared with chi-square statistics. If the sample size was less than five per cell, then Fisher’s exact test was utilized. Continuous variables (means) were compared using two-tailed student t-test.
All data manipulation and analyses were done using SAS statistical software (Release 9.4, SAS Institute Inc., Cary, NC, USA). Criteria of statistical significance were set at an alpha level of 0.05, which correlates to P = 0.05 and 95% confidence interval.
Results
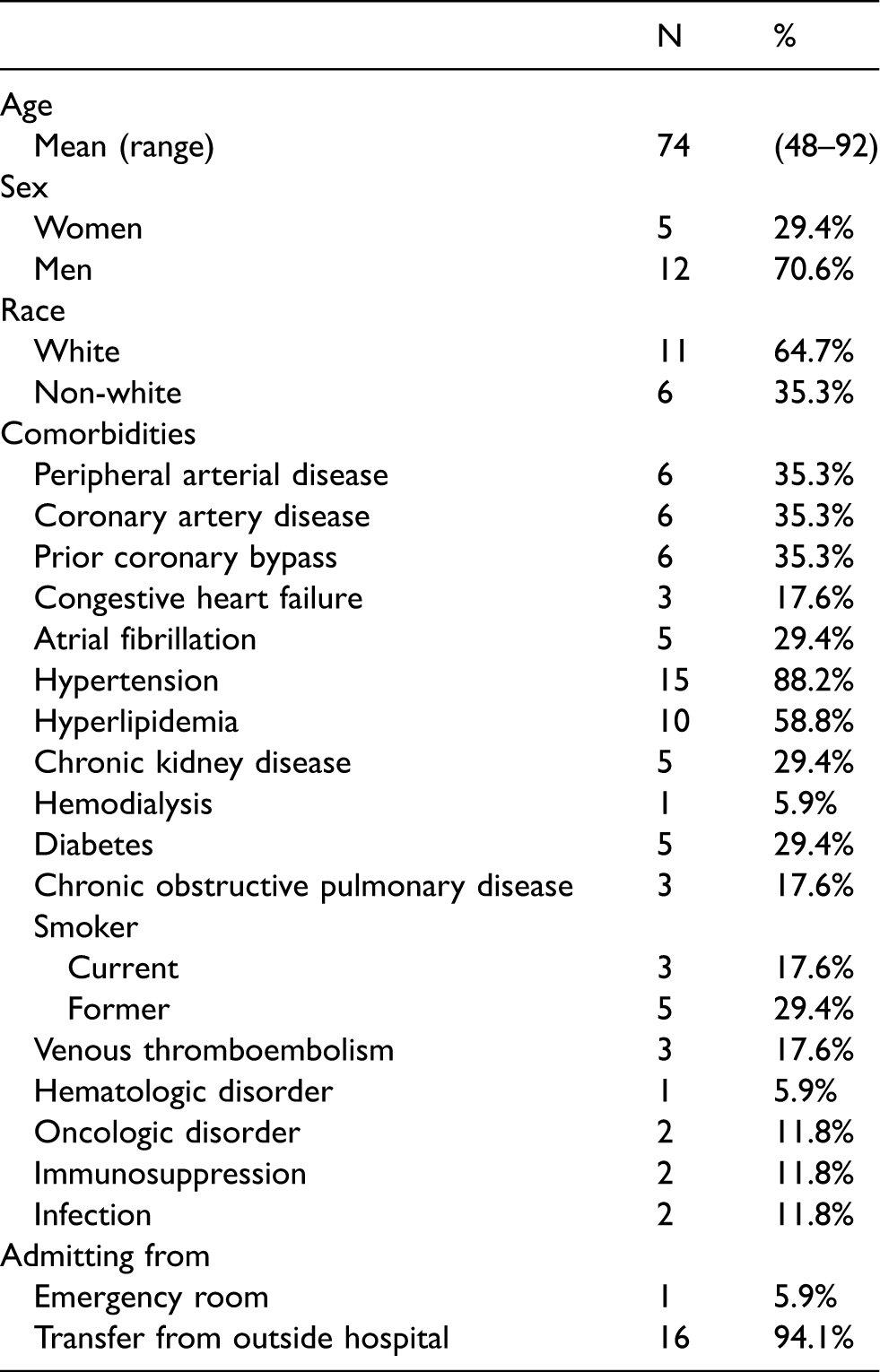
Seventeen patients presented with ruptured degenerative thoracic aortic aneurysms over the eight-year period. All of the patients underwent emergent TEVAR successfully. The mean age was 74 years (range from 48 to 92 years old) among the 5 (29.4%) women and 12 (70.6%) men treated. The majority of the patients were white (n = 11, 64.7%). Patient comorbidities were those expected of aneurysm patients, as seen in Table 1. Almost all of the patients (n = 15, 88.2%) had history of hypertension. Three (17.6%) patients were current smokers, while five (29.4%) had quit prior to presentation. Sixteen patients (94.1%) were transferred from another institution, and one (5.9%) patient was taken directly to the operating room from our emergency room.
Demographics of patients who underwent thoracic endovascular aortic repair for ruptured thoracic aortic aneurysms.
The aneurysm size ranged from 4.0 to 8.0 cm with mean of 5.9 cm. Two (11.8%) patients had a history of chronic dissection with progressive aneurysmal degeneration of the aorta. Five (29.4%) patients had previous aneurysmal repair including aortic root repair, open TAA repair, open infrarenal abdominal aortic aneurysm repair, and TEVAR (Table 2).
Ruptured thoracic aortic aneurysms characteristics.
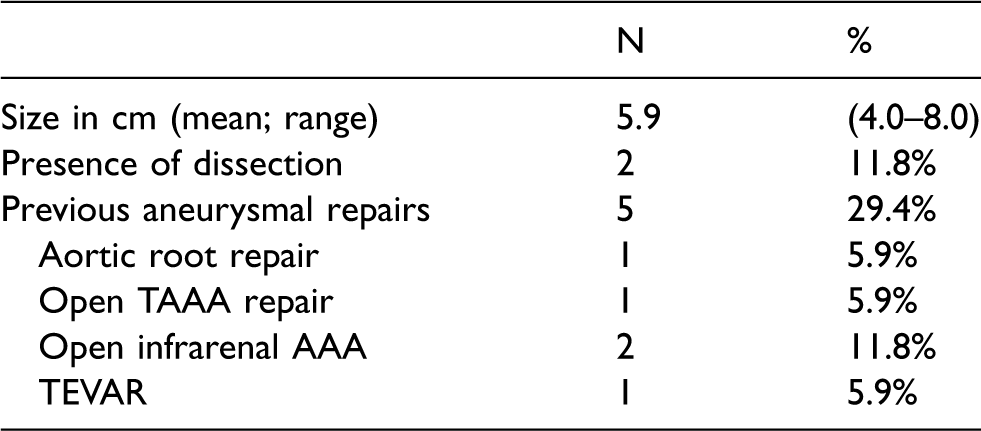
TAAA: thoracoabdominal aortic aneurysm; AAA: abdominal aortic aneurysm; TEVAR: thoracic endovascular aortic repair.
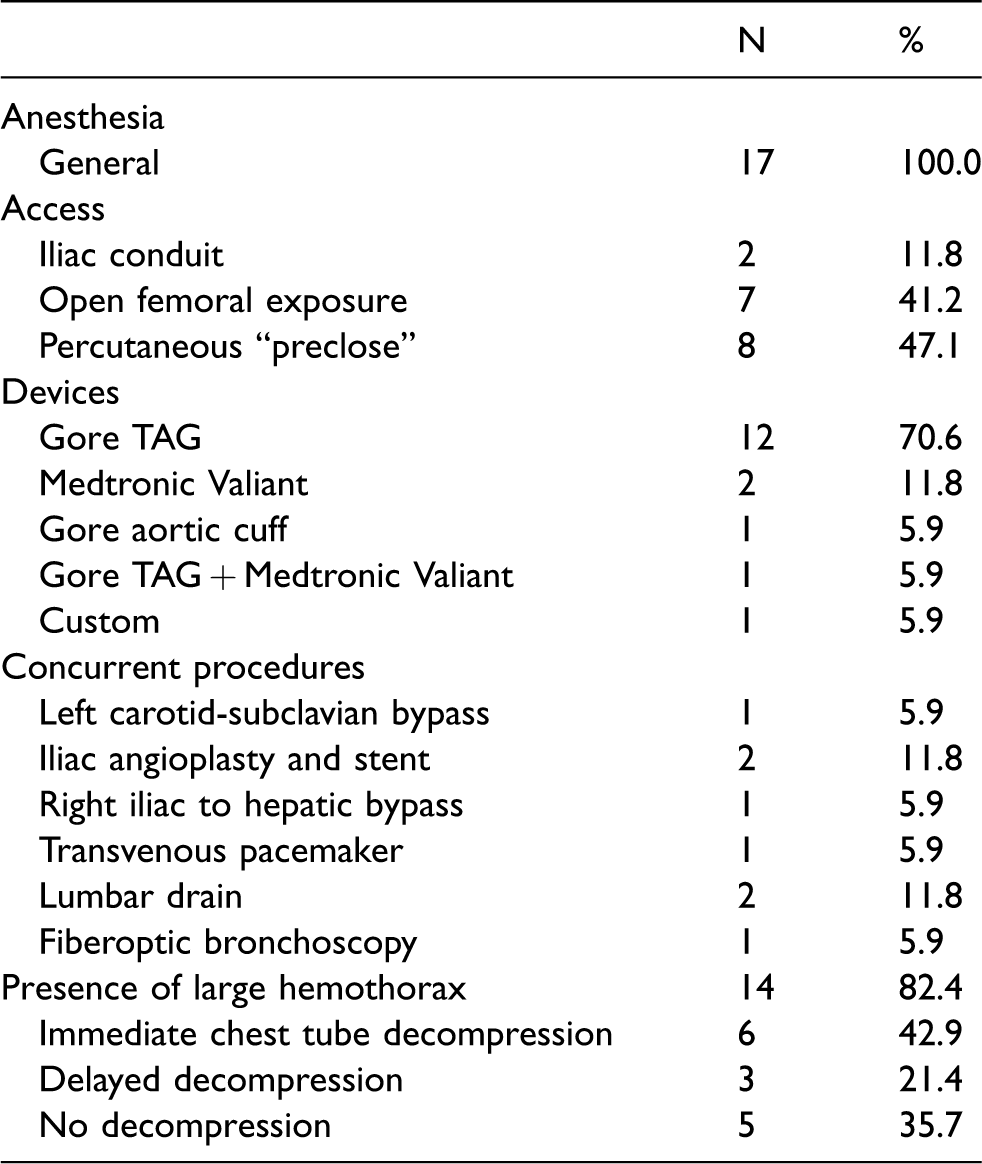
All procedures were performed under general anesthesia in an operating room hybrid suite. Access was as follows: two (11.8%) iliac conduits, seven (41.2%) open femoral exposures, and eight (47.1%) percutaneous suture-mediated “preclose” technique. While the majority of the cases (n = 12, 70.6%) were performed using Gore TAG device, Medtronic Valiant was used in two (11.8%) and Gore aortic cuff was used in one (5.9%) case. A combination of Gore TAG and Medtronic Valiant devices was used for one (5.9%) patient and another patient received a custom-made device with four 35 × 100 stents and a Gore Excluder.
In three (17.6%) cases, the left subclavian artery was covered by the proximal aspect of the stent graft and left carotid-subclavian bypass was performed in one case to preserve perfusion to a left internal mammary artery-coronary bypass. In one (5.9%) case that required coverage of the celiac artery, an ilio-hepatic artery bypass was performed. Other concurrent procedures included iliac angioplasty and stent, transvenous pacemaker, lumbar drain, and fiberoptic bronchoscopy (Table 3).
Intraoperative data from thoracic endovascular aortic repair for ruptured thoracic aortic aneurysms.
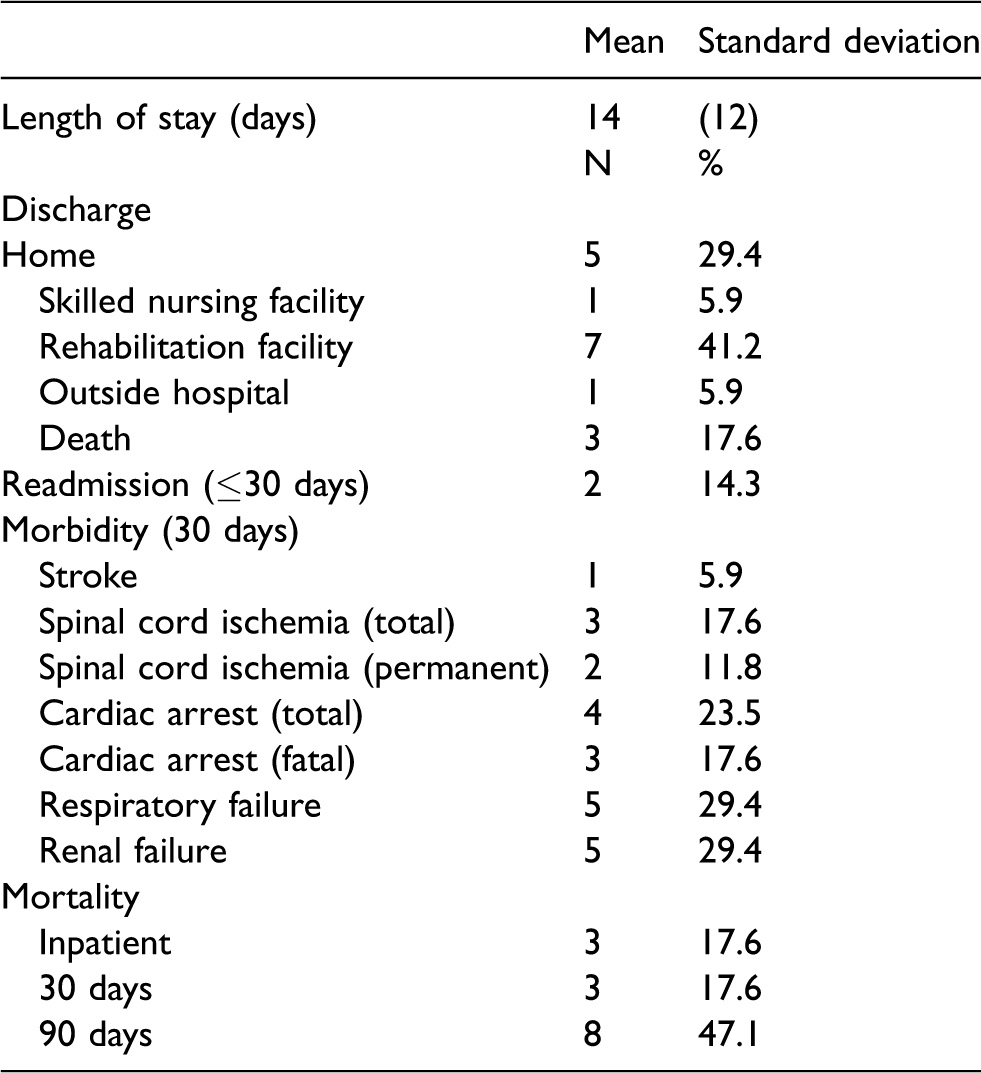
The average length of stay was 14 days (standard deviation 12 days). Only five (29.4%) patients were discharged home (Table 4). Thirty-day morbidities of the entire cohort included stroke (n = 1, 5.9%), spinal cord ischemia (n = 3, 17.6%; one was temporary), cardiac arrest (n = 4, 23.5%; 3 were fatal), respiratory failure (n = 5, 29.4%), and renal failure (n = 5, 29.4%). Two (14.3%) patients were readmitted less than 30 days from discharge, both for infectious etiology, which were attributed to an aspiration pneumonia and an infected central venous catheter, respectively. Inpatient and 30-day mortality rates for the entire cohort were both 17.6% (n = 3). The 90-day mortality rate increased markedly to 47.1% (n = 8).
Postoperative data of patients who underwent thoracic endovascular aortic repair for ruptured thoracic aortic aneurysms.
Hemothorax: Immediate vs. delayed or no decompression
Using the parameters described by Piffaretti, 10 a large hemothorax with thickness of >3 cm on a single CT slice (Figure 2) was identified in the majority of patients (n = 14, 82.4%). These 14 patients were included in the final analysis, and the 3 who did not have a hemothorax were not included in the final analysis. While six (42.9% of 14) patients had immediate decompression with chest tube thoracostomy on the day of index procedure, three (21.4% of 14) patients had delayed decompression on postoperative day 1, 4, and 7, respectively. The other five (35.7% of 14) patients had no decompression. Further analysis included patients who underwent decompression at the time of the index procedure (immediate decompression group = 6) compared to patients who did not undergo drainage at the index procedure (delayed or no decompression = 8).
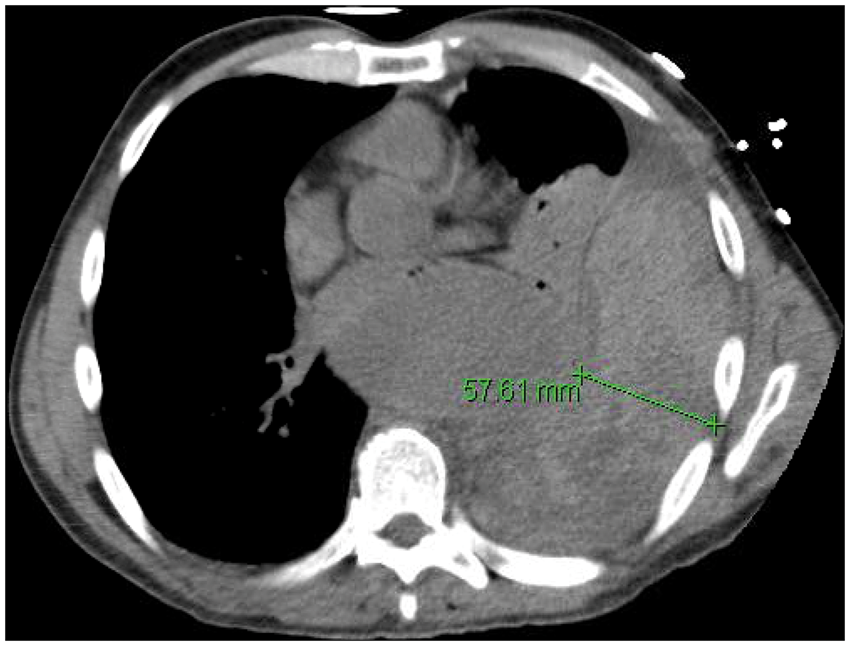
Transverse slice of CT scan showing large hemothorax.
In the immediate decompression group, five patients had a chest tube placed on the left side and one patient had a chest tube placed on the right side. Chest tube sizes used in this group ranged from 28 to 36 Fr, and the recorded volumes of fluid removed ranged from 500 to 3000 mL. Hemothorax resolution was assessed by daily chest plain film X-rays. Only one (16.7%) patient in the immediate decompression group developed pneumonia and respiratory failure. This patient had required video-assisted thoracoscopic decompression for a retained left-sided hemothorax, delayed chest tube thoracostomy for right-sided hemothorax, and eventually tracheostomy. Two (33.3%) patients died within 90 days of the index procedure: one as inpatient secondary to cardiac arrest on postoperative day 22 and another at home for unknown reason on postoperative day 50.
In the group that did not undergo immediate decompression, three (37.5%) patients had delayed drainage for respiratory failure. Overall, there were two left-sided and one right-sided chest tube thoracostomies performed with one 8 Fr pigtail catheter, one 32 Fr chest tube, and one 24 Fr chest tube, respectively. In the combined delayed or no decompression group, four (50.0%) patients developed respiratory failure with two eventually requiring tracheostomy. Five (62.5%) patients died within 90 days from index procedure: three from multisystem organ failure (two as inpatients and one after readmission for bacteremia) and two from unknown reasons as outpatients.
Although not statistically significant, when compared to patients with immediate hemothorax decompression, there were trends toward higher rates of respiratory failure (50.0% vs. 16.7%, P = 0.198) and 90-day mortality (62.5% vs. 33.3%, P = 0.280) for patients with delayed or no hemothorax decompression (Figure 3).
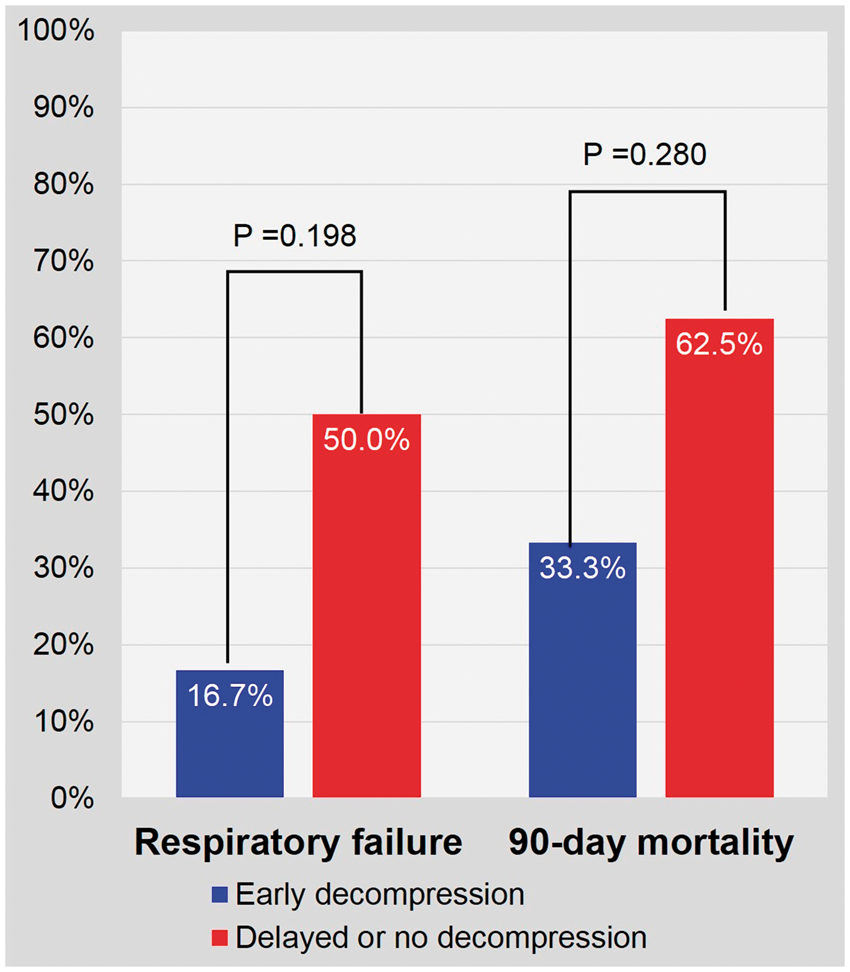
Respiratory failure and 90-day mortality for immediate (six patients) vs. delayed or no (eight patients) decompression of known large hemothorax (14 patients in total). Three patients without large hemothorax were excluded.
Discussion
Despite technically successful treatment of rTAA with TEVAR, the morbidity and mortality rates remain high in our study. Postoperative complications included those expected with a ruptured thoracic aorta, which included stroke, spinal cord ischemia, cardiac arrest, renal failure, and respiratory failure. It was noted that the majority of patients presented preoperatively with large hemothoraces. With immediate decompression of these large hemothoraces, there were trends toward reduction of respiratory complications and improvement in survival. Additionally, 37.5% of the patients not drained at the time of the index procedure received delayed tube thoracostomy.
In our experience, hemothorax was identified in more than 80% of our patients who underwent TEVAR for rTAA, which is much higher than previously reported. For example, in a 15-year multicenter retrospective review study, hemothorax was present in more than 40% of patients who underwent TEVAR and more than 50% of patients who underwent open repair for rTAA. 3 This discrepancy highlights previous underestimation of presence of hemothorax in patients presenting with rTAA. Although the number of patients is small in our series, we were able to review every patient’s preoperative images, which may not be feasible with other studies. In addition, as a tertiary center, most of our patients were transferred from outside hospitals, which could introduce selection bias for much sicker patients.
The rate of postoperative respiratory failure was found to be almost 30%, which is consistent with published literature of 16–41%.9–11 However, the rate was much lower with patients who had immediate chest tube decompression of large hemothorax (16.7%) vs. those who had delayed or no decompression (50.0%). Inpatient and 30-day mortality rates of patients who presented with rTAA and underwent successful TEVAR were both around 18%, which is also consistent with published literature of 17–48%.3,9,12 However, mortality rate increased dramatically when examining mortality at 90 days, which we found to be at least 47% overall. As suspected, 90-day mortality rate among patients who had immediate chest drainage was much lower at 33.3% compared to 62.5% for those who had delayed or no drainage. This trend highlights the importance of early chest drainage for hemothorax.
It is well established that an undrained hemothorax is associated with respiratory distress, respiratory failure, pneumonia, empyema, and fibrothorax.13,14 However, the majority of literature discussing complications from hemothoraces—found primarily in thoracic and trauma publications—is focused on patients who have a retained hemothorax after initial tube thoracostomy. Among these patients with retained hemothoraces, the incidence of pneumonia and empyema has been published to be as high as 20% and 4–33%, respectively.15–18 While these statistics are from a different cohort of patients, the alarmingly high numbers of pneumonia and empyema give reason to encourage prompt drainage of a hemothorax in relation to a rTAA, where the patient population is, on average, older and has more medical comorbidities than the population of patients with rupture secondary to thoracic aortic trauma.19,20
Despite the increased risk for pneumonia and empyema, the data are not clear on what size hemothorax warrants drainage over observation. In a retrospective study by Jonker et al. 21 , after adjusting for age among 87 patients who underwent TEVAR for rTAA, hemothorax at admission had an odds ratio of 6.65 for 30-day mortality. A recommendation for prompt drainage was made when accounting for care of these critically ill patients. However, no discussion was made regarding intervention for patients with hemothoraces and parameters used for intervention. Additionally, in a single-center study by Shu et al. 22 outcomes of 45 patients who underwent endovascular repair of a complicated acute type-B aortic dissection were evaluated. Six patients were categorized as ruptured and 27 patients had hemothorax with impending rupture. It is recognized that radiographic evidence of dense pleural effusions in the presence of an acute aortic dissection is oftentimes a reactive effusion rather than a true hemothorax or rupture. This makes comparison with a true rupture and associated hemothorax difficult. Nevertheless, among these patients, thoracentesis was utilized in five patients and tube thoracostomy was performed once to improve respiratory function. Again, the authors did not mention a threshold for intervention, including size of the hemothorax or clinical criteria.
Currently, the most thorough vascular study evaluating hemothorax management after TEVAR in thoracic aortic rupture is by Piffaretti. 10 Fifty-six patients were treated in a multicenter review, and hemothoraces were graded by thickness: < 2 cm, 2–3 cm, or > 3 cm. The authors noted the decision for intervention was made after individual case review by the surgical team and intensive care unit physicians using clinical parameters that included respiratory index (Pao2/Fio2) < 200 or signs of respiratory or cardiovascular compromise. Of note, only 38% of patients underwent hemothorax evacuation by tube thoracostomy (16) or surgical evacuation (6). The authors recommended prompt drainage for thickness >3 cm or respiratory index <200, although only 47% of patients included with thickness >3 cm actually underwent drainage.
At our institution, we do not have departmental respiratory parameters or size guidelines for hemothorax drainage, so hemothorax drainage at the time of the index operation was attending-dependent, whereas chest tube drainage after postoperative day 0 was performed after patients exhibited signs of respiratory failure. The inconsistent use and timing of tube thoracostomy within a single institution highlights the need for further review of this problem and better treatment guidelines. While the actual numbers treated in these studies as well as our own experience remain lower than expected, we agree with the previous literature that the improved survival and decreased respiratory failure with early chest drainage for hemothorax have been documented and we recommend prompt treatment of hemothoraces in rTAA.
Limitations
Limitations of this study are similar to those of retrospective chart reviews. Lists of comorbidities and complications were constrained by clinical documentation, especially when the complications and deaths occurred at another institution or as an outpatient. However, we felt that our mortality rates were close estimations with the aid of Social Security Death Index. The clinical documentation also limited our ability to evaluate long-term follow-up imaging, which would have been ideal to evaluate and compare the clinical course among the treatment and observation groups.
While current vascular literature has compared hemothoraces in thoracic aortic ruptures secondary to trauma, dissection, and aneurysmal degeneration, we chose to select only those patients with ruptures secondary to aneurysmal degeneration, which contributed to our small patient cohort. Additionally, while ultrasound and CT have been used in diagnostic measurements of hemothoraces, there is not a standardized classification system in the literature. With this in mind, we categorized hemothoraces in line with Piffaretti. 10 Finally, this study reflects outcomes in a cohort with large hemothoraces, so these results may not be representative of patients with small and medium hemothoraces.
Conclusions
The morbidity and mortality of ruptured degenerative thoracic aortic aneurysms remain high despite the introduction of TEVAR. Early chest decompression of hemothorax after TEVAR appears to improve respiratory complications and overall survival. However, given the rarity of rTAA, there is currently not a uniform treatment paradigm. An aggregate study, such as a multicenter meta-analysis, may be helpful and allow for further assessment and multivariable analysis in order to assess ideal size, clinical parameters, or timing of hemothorax evacuation.
Footnotes
Acknowledgments
This article has been presented in the Poster Competition at the 2016 Vascular Annual Meeting of the Society for Vascular Surgery, National Harbor, MD, 8–11 June 2016.
Author contributions
Study concept and design: Ju, Rodriguez, Eskandari; Acquisition of data: Ju, Rodriguez, Eskandari; Analysis and interpretation of data: Ju, Rodriguez, Eskandari; Drafting of the manuscript: Ju, Nooromid; Critical revision of the manuscript for important intellectual content: Ju, Nooromid, Rodriguez, Eskandari; Statistical analysis: Ju; Administrative, technical, or material support: Ju; Study supervision: Eskandari.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr Rodriguez has received honoraria from W. L. Gore and Associates, Trivascular Inc, and Abbott as a speaker/consultant. Dr Eskandari has received honoraria from Prairie Education and Research Cooperative (Bard) for service on the LEVANT 2 clinical events committee; from Silk Road Medical, Inc. for service on the Roadster clinical events committee; and from W. L. Gore and Associates as a TEVAR course director.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Research reported in this publication was supported by the National Heart, Lung, and Blood Institute of the National Institutes of Health under Award Number T32HL094293 in the form of partial stipend support for Dr. Michael Nooromid. The content of this publication is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.