
Abstract
Objectives
To evaluate long-term outcome and quality of life after open and endovascular repair of ruptured abdominal aortic aneurysms.
Methods
All consecutive ruptured abdominal aortic aneurysm patients at the St. Antonius Hospital treated for ruptured abdominal aortic aneurysm between January 2005 and January 2015 were included. Mortality, morbidity, and re-interventions within 30 days and during follow-up were registered. Quality of life was measured with Short Form-36 questionnaire among survivors. Additional subgroup analysis between open repair and endovascular repair was performed.
Results
A total of 192 patients with ruptured abdominal aortic aneurysm were included: 76.6% (147/192) underwent open repair and 23.4% (45/192) endovascular repair. All-cause 30-day mortality rate was 31.3% (60/192), and 30-day morbidity rate was 70.3% (135/192). Median stay at the intensive care unit was two days for endovascular repair and four days for open repair (p = 0.002). No other statistically significant differences between endovascular repair and open repair were observed. After a mean follow-up period of 62 months (range 9–126), 72.4% (76/105) of the responders had equivalent Short Form-36 scores as compared to the age-matched general Dutch population, and 84.2% (64/76) of the responders would choose surgery again if they would have a ruptured abdominal aortic aneurysm.
Conclusions
Survivors of ruptured abdominal aortic aneurysm have similar long-term quality of life scores compared to the age-matched general population. The majority of all survivors would choose to undergo acute abdominal aortic aneurysm repair again.
Introduction
Ruptured abdominal aortic aneurysm (rAAA) remains one of the most common vascular emergencies with an overall mortality rate of 48.5% (95% CI 48.1–48.9%). 1 Thirty-day mortality rates after rAAA repair is reported to be up to 40%, with no significant differences between open and endovascular repair (EVAR).2–4 Admissions for rAAA have declined due to the increases in elective AAA repair. 5 Both endovascular as well as open rAAA repair have been associated with substantial morbidity rates such as cardiac complications, renal failure, ischemic colitis and need for reoperation. 6 Considering this a burden for patients and health care systems, quality of life (QoL) is an important outcome measure. There are many studies focussing on short- or midterm outcome after rAAA. 7 There are also multiple studies comparing short-term QoL after endovascular and open repair.8–10 However, long-term outcomes and QoL after rAAA repair is relatively underexposed in currently available literature, which led to the aim of this study. To contribute to current discussions on open vs. EVAR for rAAA we added subgroup analyses of open vs. endovascular rAAA repair.
Materials and methods
All consecutive rAAA patients at the St. Antonius Hospital, treated between January 2005 and January 2015, were included. Required data were retrieved retrospectively. The Local Research Ethics Committee granted approval for this study.
Management of rAAA included full primary survey at the emergency department by a vascular surgeon, radiologist, and anesthesiologist. An ultrasound was performed at the emergency department to confirm the presence of rAAA and eventual retroperitoneal hematoma. If rAAA was present, permissive hypotension (systolic blood pressure at least 70 mmHg) was accepted. Hemodynamic unstable patients with confirmed rAAA were directly transported to the operation theater for open repair. If patients were hemodynamic stable, a computed tomography (CT) scan was performed. If the anatomy was suitable for EVAR, this was consequently performed in the hybrid operating room. Criteria for anatomical suitability for EVAR were based on a local multidisciplinary (vascular surgeons and interventional radiology) protocol. Patients were considered unsuitable for EVAR based on neck characteristics defined as the presence of one or all of the following characteristics: neck length <10 mm, diameter >30 mm, and infrarenal neck angulation >75°, or the need to embolize and overstent both internal iliac arteries. Of all patients with a CT scan, center lumen line reconstructions were made, and measurements performed during the time a patient was transported from the CT scan back to the emergency department or to the hybrid operating room.
EVAR was performed under general or local anesthesia with percutaneous or open femoral access. This choice was dependent of the operating team and the patient’s anatomy. All endovascular patients had a bifurcated endograft.
Open repair was performed under general anesthesia. With open repair the approach to the aorta was transperitoneal. Aortic clamping included infra-, juxta-, or suprarenal clamping. A cell saver was used during all open procedures. If possible a tube graft was implanted. In case of iliac artery aneurysms (>3 cm) or iliac rupture, a bifurcated graft was inserted.
The following baseline characteristics were registered: age, gender, blood pressure at the time of admission, hemoglobin, creatinine, acute myocardial ischemia on electrocardiogram at the time of admission, consciousness and Glasgow Coma Scale (GCS), Hardman index, Glasgow Aneurysm Scale (GAS), maximum aortic diameter, type of surgery (open or EVAR). The duration of the operation and blood loss were scored for all procedures.
To report outcome after surgery the following endpoints were registered with medical records: 30-day morbidity and mortality. Thirty-day mortality included all causes of death within 30 days of surgery.
For 30-day morbidity, all adverse events during the first 30 days after surgery were reported. Pneumonia was defined according to the guidelines of the American Thoracic Society. 11 Cardiac failure or myocardial infarction was scored based on the conclusion reported by the cardiologist, with documented electrocardiography changes or elevated cardiac enzymes, according to the Joint European Society of Cardiology and the American College of Cardiology Committee. 12 Renal failure was defined as an eGFR<15 ml/min/1.73 m2, or permanent need for dialysis, according to the National Kidney Foundation (KDOQI) guidelines. 13 Stroke was defined as neurologic deficit lasting >24 h; transient ischemic attack was defined as neurologic deficit lasting <24 h, all documented by a neurologist. In addition, the number of postoperative days at the intensive care unit (ICU), and the number of hospital admission days were registered.
All surgical or endovascular secondary interventions during the first 30 days were reported, including re-bleeding requiring surgery, bowel ischemia, wound dehiscence revisions for graft infections, graft occlusions, or endoleak.
During follow-up, all-cause mortality and AAA related re-interventions were registered using medical records. If patients were discharged from follow-up or did not visit the hospital the past years, the general practitioner was contacted for current status and address.
Patients who were alive at the time of the current study were contacted and were asked to complete and return a Dutch version of the Short Form-36 (SF-36) questionnaire to evaluate their QoL. 14 The SF-36 is a validated instrument to evaluate the QoL and comprises 36 questions studying eight domains of health: physical functioning, social functioning, role limitations due to physical problems, role limitations due to emotional problems, mental health, pain, vitality, and general health perception. Each domain scores from 0 to 100, with higher scores representing a better QoL. The validity and reliability of the SF-36 have been confirmed, and its use in the assessment of vascular and aneurysmal disease has been recommended.15,16 It is commonly accepted that QoL decreases with increasing age. We therefore compared the current QoL data to age-matched data from the general Dutch population. 14 An additional question was included in the SF-36: whether the patient would choose to undergo surgical repair again in case of a ruptured AAA.
The SF-36 scores were calculated and statistical analysis was performed with SPSS version 22.0 (SPSS Inc., Chicago, IL, USA). The Pearson’s chi-square test was used for statistical analysis between two categorical variables. The independent-samples t-test was used to compare means of parametric data of two groups. The Mann–Whitney U test was used to compare medians of non-parametric data of two groups. p-Value <0.05 was considered statistically significant.
To contribute to current discussions on open vs. EVAR for rAAA, we added subgroup analyses of open vs. endovascular rAAA repair.
Results
Overall
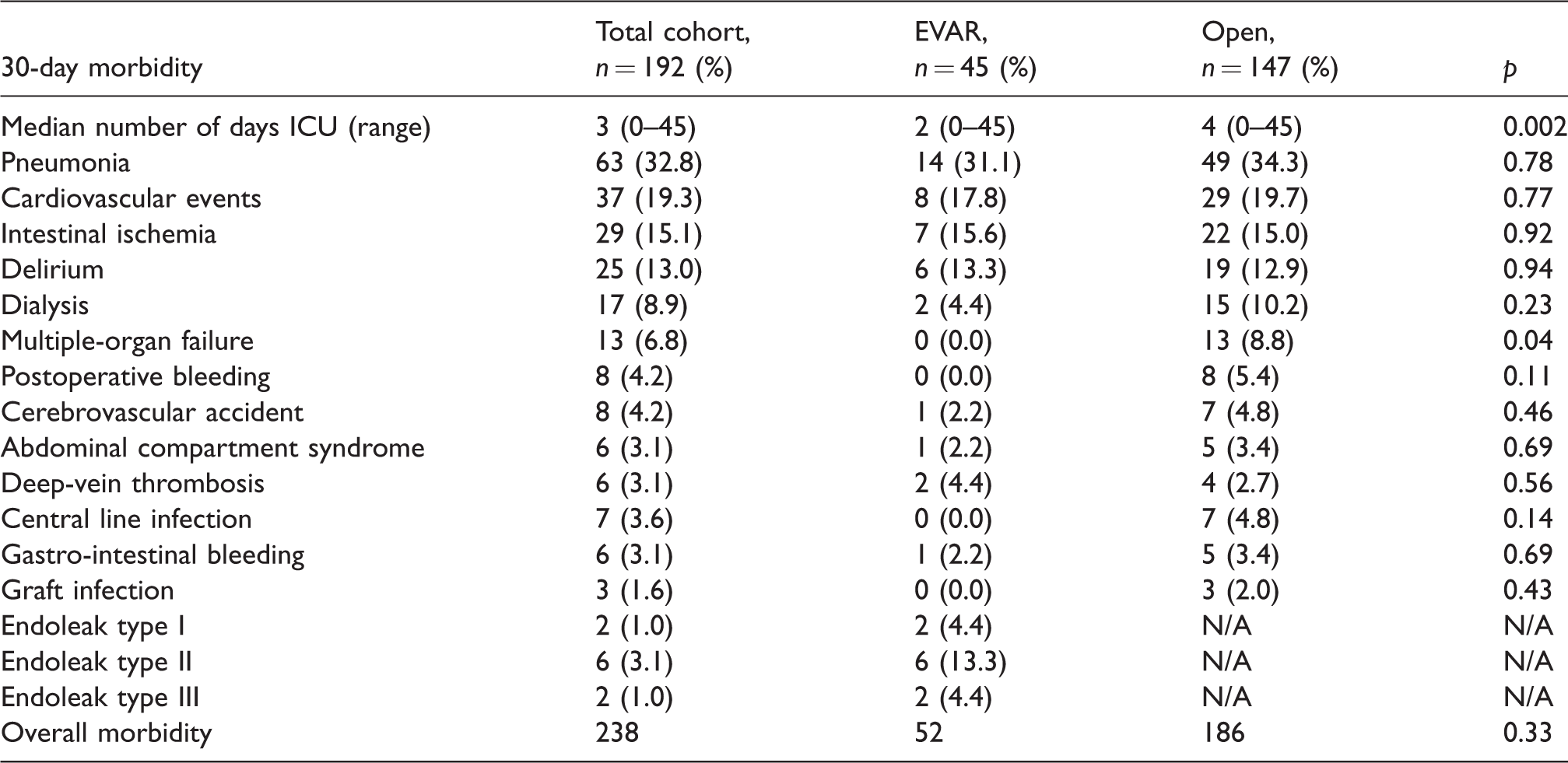
A total of 192 patients with rAAA who underwent surgical repair during the study period were included. One hundred and sixty-eight (87.5%) were male and mean age was 72.6 years (±8.4). Some patients (147/192, 76.6%) underwent open surgical repair and 23.4% (45/192) were treated with EVAR. Baseline characteristics on admission are presented in Table 1 for the total cohort. The 30-day mortality and morbidity rates are shown in Table 2. All-cause 30-day mortality rate was 31.3% (60/192), and 30-day morbidity rate was 70.3% (135/192). Adverse events are shown in Table 3. The median number of days at the ICU was three days (0–45). A total number of 238 adverse events were scored for 135 patients. The most frequently observed 30-day adverse events (Table 3) were pneumonia (32.8%), cardiac arrhythmia and cardiac ischemia (19.3%), intestinal ischemia (15.1%), and permanent dialysis (8.9%).
Baseline characteristics of patients with ruptured AAA.
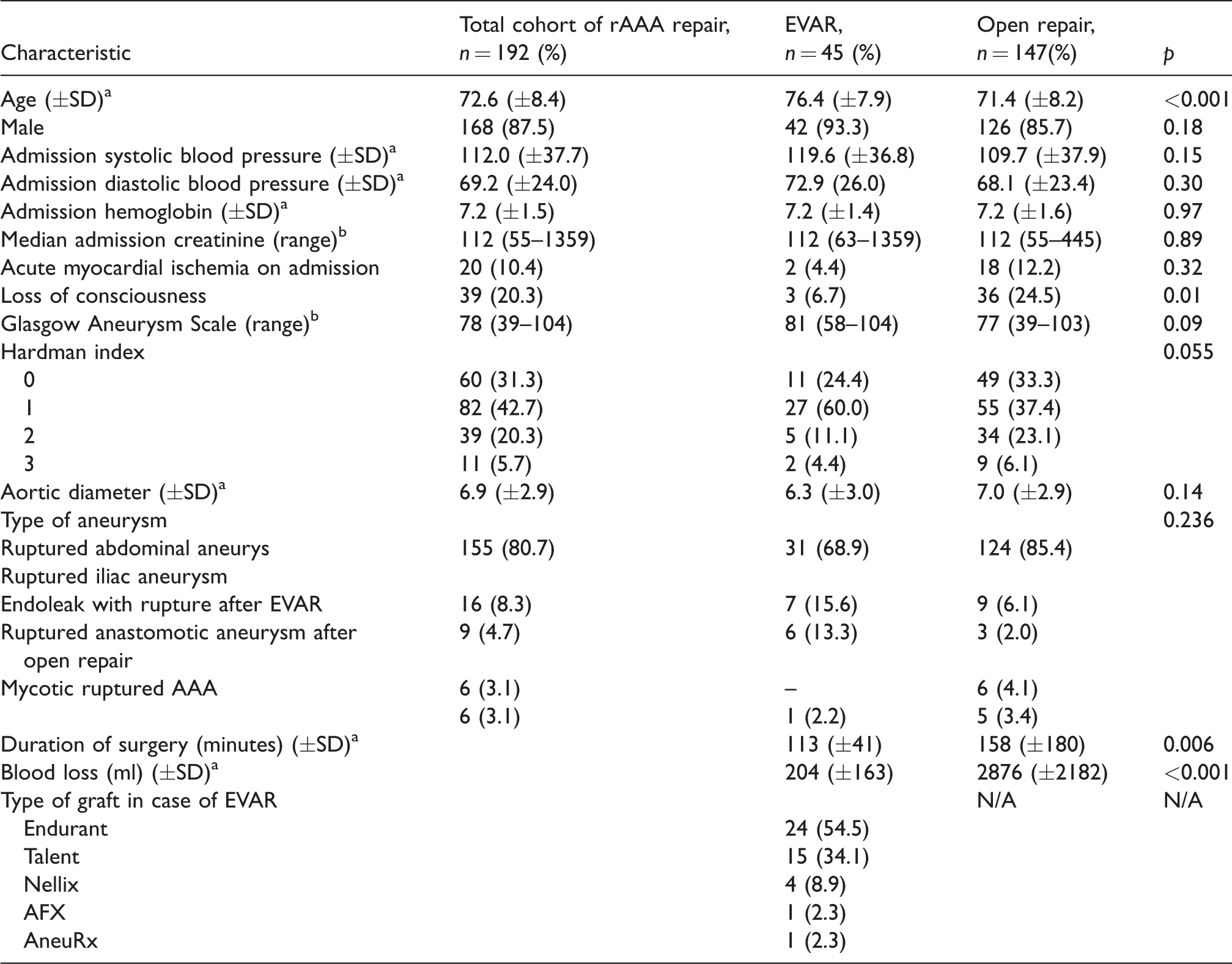
EVAR: endovascular repair; rAAA: ruptured abdominal aortic aneurysm.
aMean (SD).
bMedian (range).
Thirty-day mortality and morbidity.

EVAR: endovascular repair.
Thirty-day morbidity, data for open repair and EVAR separately.
EVAR: endovascular repair; ICU: intensive care unit.
Numbers and reasons for re-interventions (n = 52) within 30 days after rAAA repair are shown in Table 4. Most re-interventions were due to (suspected) intestinal ischemia (44.2%) and postoperative bleeding (15.4%). Ten patients (19.2%) had no ischemia during laparotomy and no other intervention was needed. Thirteen patients (25%) had a (partial) colon resection.
Re-interventions within 30 days after rAAA repair.
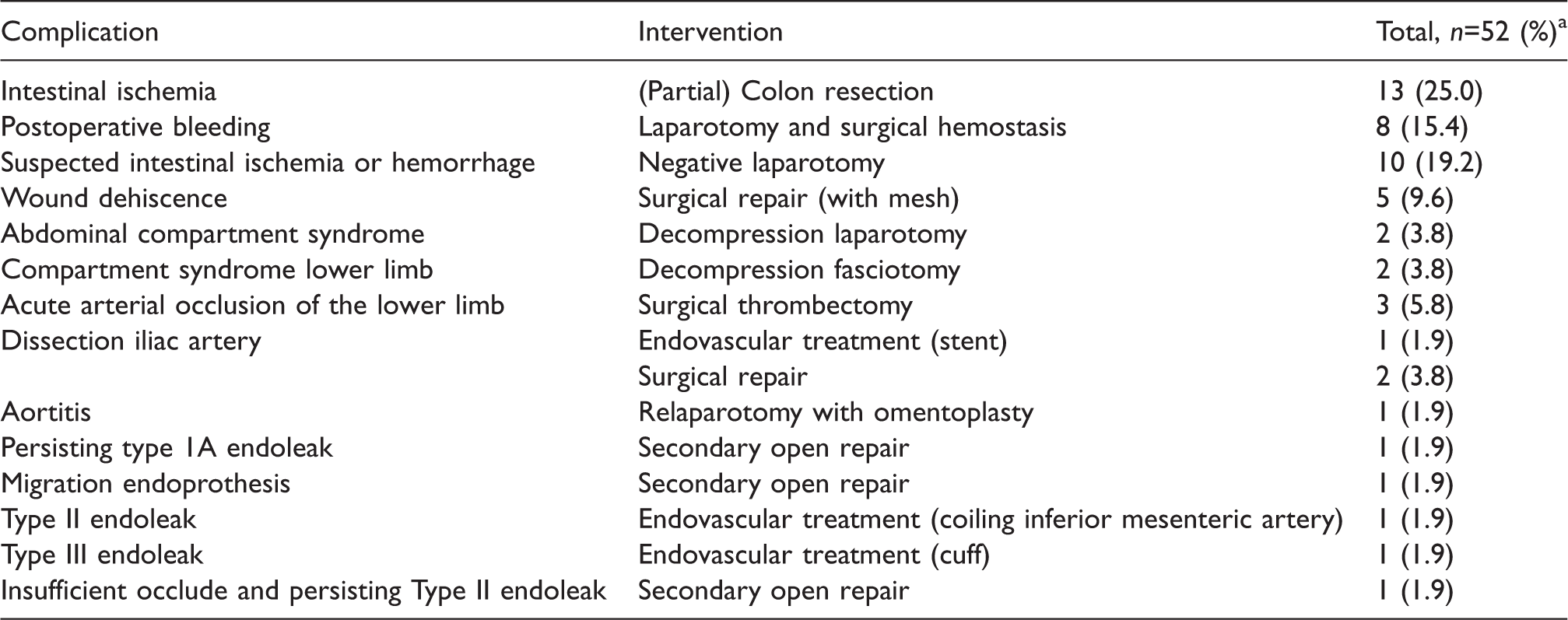
EVAR: endovascular repair; rAAA: ruptured abdominal aortic aneurysm.
a42 (28.6%) re-interventions after open repair were performed and 10 (22.2%) after EVAR (p=0.40).
During a mean follow-up period of 62 months (range 9–126), all-cause mortality was 45.3% (87/192). Some patients (17/192, 8.8%) required secondary interventions during follow-up. Eight (47.1%) of these interventions were due to an incisional hernia.
A total of 105 SF-36 questionnaires were sent to all currently living patients. Response rate was 72.4% (76/105). Twenty-five patients (17.1%) did not respond or could not be reached. Five patients (4.8%) were contacted, but could not participate due to: dementia (n = 3), cerebral ischemia (n = 1), and cognitive impairment (n = 1). Six patients (5.7%) were not willing to participate. A flowchart of the total cohort is provided in Figure 1. The mean follow-up period among responders was 46 months after the primary ruptured AAA repair (range 9–126). Mean age among patients who completed the SF-36 questionnaire was 74 years. The results were compared to the QoL of the general Dutch population aged 70 years or older. 14 The data are shown in Table 5, which displays that there were no statistically significant differences between QoL in the current cohort and the general Dutch population >70 years.
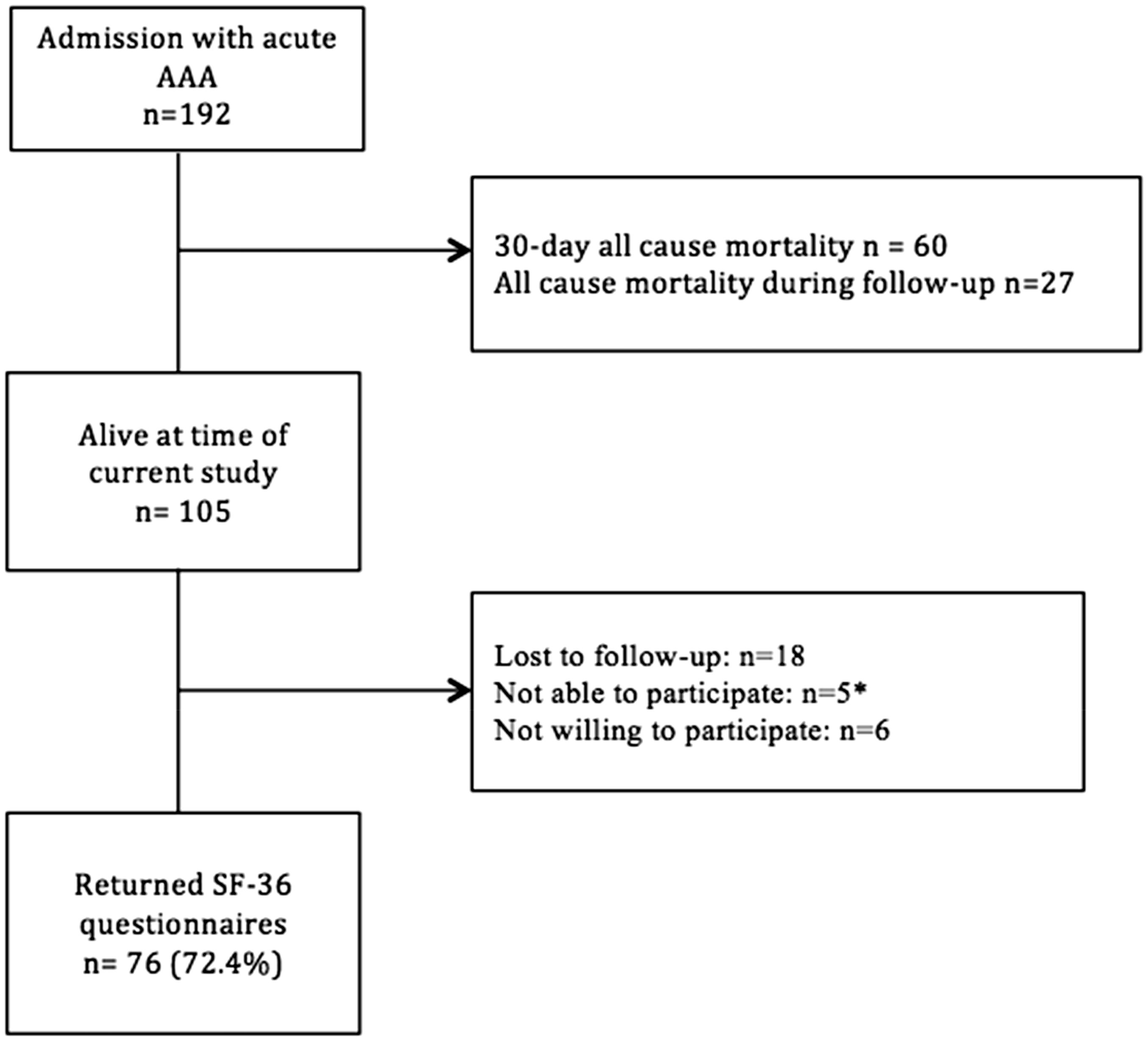
Flow chart of patient cohort. The number of admissions was 192. Patients alive at the current time of the study were 105. The number of returned SF-36 questionnaires was 76.
Quality of life assessment with SF-36 questionnaire after mean follow-up time of 46 months (9–126) after ruptured AAA-repair and age-matched data from general Dutch population.
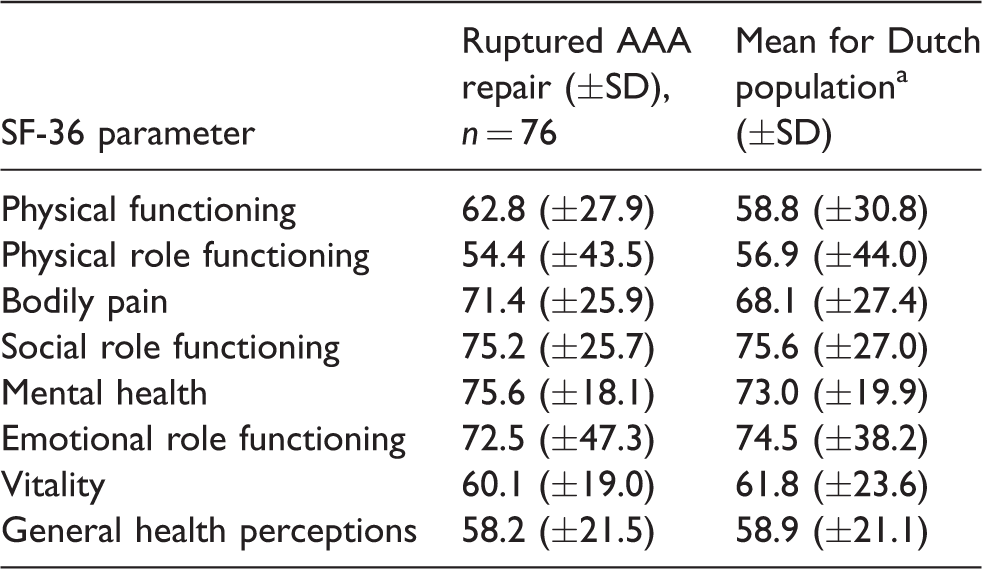
Note: Values presented as mean (±SD).
AAA: abdominal aortic aneurysm; SF-36: Short Form-36.
aBased on Aronson et al. 14 age-corrected data.
Respondents (95%) also responded to the additional question if they would choose to undergo surgical repair again if they would suffer an rAAA again. Sixty-four patients (84.2%) would choose to undergo rAAA repair, four (5.3%) would not want to undergo repair again, and four (5.3%) were in doubt.
Open repair vs. EVAR
Baseline characteristics on admission are presented in Table 1 for the endovascular and open repair cohorts. Mean age among open repair was 71.4 years (±8.2) and 76.4 years (±7.9) among EVAR (p = <0.001). Other significant differences between both groups were loss of consciousness at administration. Three (6.7%) within EVAR vs. 36 (24.5%) within open repair (p = 0.01). Also a shorter operation duration and less blood loss were found when EVAR was performed. Mean operation duration was 113 min (±41) for EVAR vs. 158 min (±180) for open repair (p = 0.006). Mean blood loss was 204 ml (±163) for EVAR and 2876 ml (±2182) for open repair (p = <0.001).
The 30-day mortality and morbidity rates for EVAR and open repair are shown in Table 2. Thirty-day mortality rate for EVAR was 20.0% (9/45) vs. 34.7% (51/147) for open repair (p = 0.06). Thirty-day morbidity rate was 64.4% (29/45) for EVAR vs. 72.1% (106/147) for open repair (p = 0.33).
The median number of days at the ICU was two days for EVAR vs. four days for open repair (p = 0.002). Multiple organ failure was 0% (0/45) after EVAR and 8.8% (13/147) after open repair (p = 0.04). No other significant difference of morbidity rate was found between EVAR and open repair (Table 3).
Numbers and reasons for re-interventions (n = 52) within 30 days after rAAA repair are shown in Table 4. Some patients (42/147, 28.6%) had a re-intervention within 30 days after open repair and 22.2% (10/45) after EVAR (p = 0.40). All-cause mortality after open repair was 44.2% (65/147) vs. 48.9% (22/45) after EVAR (p = 0.582).
The comparison of QoL between EVAR and open repair showed higher rates of QoL after open repair in all components of the SF-36 assessment with significant difference regarding three components (physical role functioning p = 0.02, bodily pain p = 0.01, social functioning p = 0.02). Data are shown in Table 6.
Comparison of quality of life assessment with SF-36 questionnaire after open repair and EVAR.
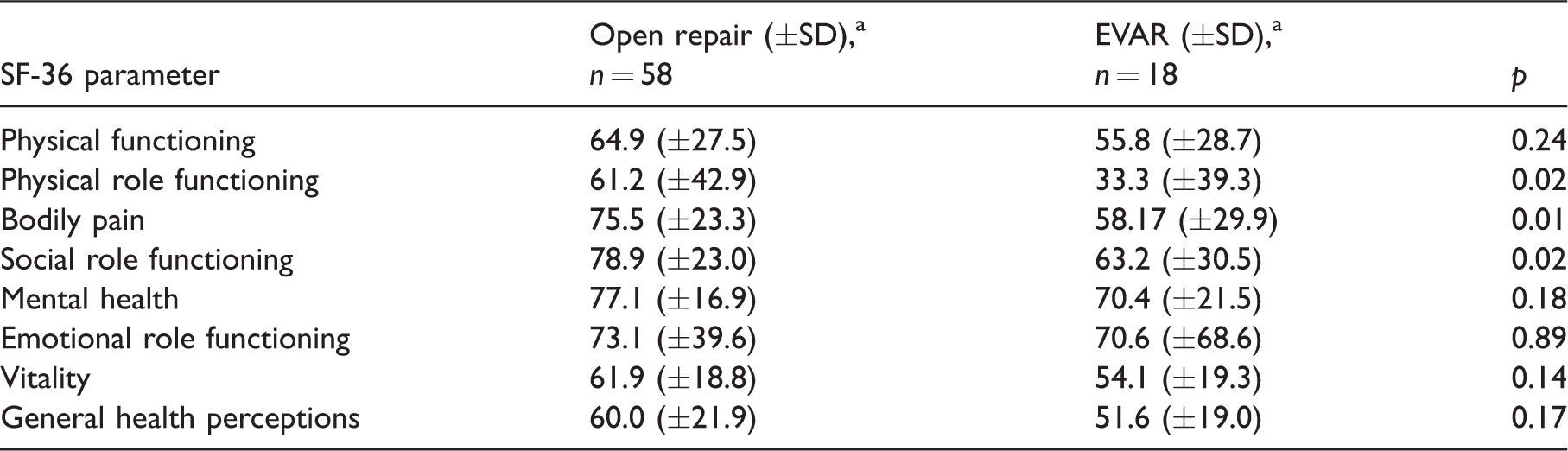
EVAR: endovascular repair; SF-36: Short Form-36.
aValues presented as mean (±SD).
Discussion
Thirty-day mortality rates after rAAA repair is reported to be up to 40%, as found in this cohort study.2–4 The data of this cohort show that most of the re-interventions are within 30 days. Re-interventions after 30 days are mostly due to incisional hernia.
Postoperative QoL is an important factor to decide on whether to perform major surgical interventions. There are only a few studies that reported the validated SF-36 of patients who survived rAAA repair.17–19 Hill et al. compared the health-related QoL (HRQoL) for patients who survived open surgical repair after rAAA with an elective open AAA repair group. After 37.7 months, they reported no significant difference between the rAAA group and the control group. 17 Korhonen et al. 18 used the RAND-36 (which is based on SF-36) to compare rAAA survivors (mean follow-up time 33 months, mean age 72–75 years) with age- and sex-adjusted Finnish population norms and also found no difference in QoL.
Tambyraja et al. 20 evaluated QoL after elective AAA repair and rAAA repair and compared data with individuals from the general population in a prospective observational case–control study with a follow-up time of six months and a mean age of 68 years. No differences could be determined between patients and general population matched for age and gender.
To our knowledge, this study is the first study to report data on QoL with a validated SF-36 questionnaire, at a relatively long-term follow-up time of 62 months after acute AAA repair. Although the study design is a retrospective cohort study, response rate of SF-36 questionnaires reached a satisfactory proportion of 72.4%.
Because of the retrospective design of this study, selection bias may have occurred, despite the relatively high response rate. Subgroup analysis showed that the baseline characteristics of the responders were comparable to the total cohort, suggesting a representative sample. The relatively long mean follow-up time may have caused alterations in QoL due to increasing age-related morbidities. This might have influenced QoL negatively as well as the answers in the questionnaires. Nevertheless, the QoL is not different from the general population after a longer follow-up period following rAAA. Patients with AAA have often co-morbidities like cardiovascular disease, chronic obstructive pulmonary disease, diabetes mellitus, and renal failure. These co-morbidities are reported not to affect the survival after rAAA repair. 21
The percentage of patients with EVAR has increased over the years. In 2005, none of the 13 patients with a ruptured AAA was treated by endovascular means, whereas 11 of 20 patients in 2014 were treated with EVAR. This explains the overall lower rate of EVAR compared to open repair. No significant differences were found between EVAR and open repair considering 30-day mortality and morbidity rates, except for a longer stay at the ICU after open surgery. Previous randomized controlled trials showed no difference in 30-day and one-year mortality rates between EVAR and open repair after rAAA. However, EVAR was associated with less severe complications and a shorter hospital stay.3,4,22,23 Other studies have shown that patients surviving more than 30 days postoperatively have a life expectancy similar to an age- and sex-adjusted population, which is in line with our data.24,25 A recent meta-analysis supports EVAR after rAAA in selected patients. Li et al. compared EVAR with open repair with elimination of the effect of hemodynamic unstable patients. This shows that EVAR is superior over open repair with regard to perioperative mortality. 26
The data shown in this study were collected retrospectively. The fact that patients were not randomized for open repair or EVAR will have resulted in selection bias. Hemodynamic stable patients with ruptured AAA are more often selected for EVAR and hemodynamic unstable patients selected for open repair. 27
Our data show comparable values at presentation at hospital admission. Systolic and diastolic blood pressure at hospital admission is comparable. Loss of consciousness at presentation was higher for open repair. However, not all of these patients were hemodynamic unstable at presentation. Furthermore, mean age was approximately five years lower among patients who underwent open repair for rAAA. Open repair patients had significantly better outcome regarding physical role functioning, bodily pain, and social functioning. This might be due to the difference in age between EVAR and open repair. Therefore, subgroup analysis of the SF-36 domains was made corrected for age. Physical role functioning and bodily pain still showed significant difference after correction.
Despite that bias may have occurred, this data show that EVAR is not inferior to open repair and should remain the first treatment of choice for rAAA in patients with suitable anatomy.
Nevertheless, some limitations of this study should be addressed. This is a single center, non-randomized comparison between endovascular and open repair for ruptured AAAs. Data were collected retrospectively and therefore some patients had missing data. Also the influence of comorbidities was not evaluated in this study. This might affect our data.
The QoL comparison is flawed by the retrospective nature of the study design and the large time range for completing the QoL questionnaires, although conclusions have been drawn on a high response rate of 72.4%. Moreover, there was a difference in the time period of completing the SF-36 questionnaires between open repair vs. EVAR (median 51 months vs. 44 months). Perkins et al. have found in a prospective study of elective repair that a three-month period is required to regain full QoL, which explains why only QoL forms have been included >3 months after ruptured AAA repair. 28
Conclusion
Survivors of rAAA have similar long-term QoL compared to the age-matched general population. The majority of all survivors would choose to undergo acute AAA repair again.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.