
Abstract
Introduction
Critical hand ischemia with advancing gangrene of digits requires urgent intervention to salvage as much tissue as possible. The purpose of this study was to evaluate the efficacy of “palmar arch loop” technique for endovascular management of critical hand ischemia by establishing inline flow to the palmar arch via both radial artery and ulnar artery, in patients with failed antegrade recanalization. To the best of our knowledge, this is the first case series evaluating the efficacy of “palmar arch loop” technique, with retrograde percutaneous transluminal angioplasty of the involved radial artery and/or ulnar artery.
Material and methods
We retrospectively investigated 10 patients (60% female; mean age 42 ± 18 years; mean time of presentation post-acute event 24 ± 11 days) with critical hand ischemia undergoing endovascular intervention using “palmar arch loop” technique at a single center in northern India between April 2017 and March 2019. All patients were followed up at regular intervals (weekly for a month, fortnightly for 3 months, and then at 6 and 12 months) with clinical assessment and SpO2 measurement. Study end points were technical success rate, hand healing, and primary patency rate at one year.
Results
Causes for critical hand ischemia were iatrogenic injuries due to inadvertent intra-arterial injection in 50% (n = 5) and thromboembolic events in 50% patients (n = 5). Vessels involved were: both radial artery and ulnar artery along with the PA in 50%; radial artery and palmar arch in 30%; ulnar artery and palmar arch in 20%. All of them had total occlusion of the involved vessel (>2/3rd of total length) with occlusion/diffuse disease of palmar arch as well; 70% technical success rate was achieved ensuring inflow to palmar arch via both the arteries with improved flow distally to the common and proper digital arteries. Retrograde percutaneous transluminal angioplasty of radial artery in 50% (n = 5) and ulnar artery in 20% (n = 2) was done successfully by looping the guidewire across the palmar arch; 90% showed subjective improvement in pain with healing of the lesions and/or formation of clear line of demarcation with reversal of pregangrenous changes proximally. Out of the eight patients with gangrene of fingers, three underwent minor amputation of the gangrenous digits and five underwent auto-amputation of the gangrenous tissue with complete healing of the stump. Primary patency rate was 85.7% at one year. There was no access site-related complication or mortality in the follow-up period.
Conclusions
Endovascular management of critical hand ischemia by “palmar arch loop” technique is an efficient technique to deal with occluded forearm vessels, particularly when antegrade recanalization fails. This technique, with good technical success and patency rates, is potentially a unique tool in the endovascular armamentarium for salvaging hand.
Introduction
Critical hand ischemia (CHI) with advancing gangrene of digits requires urgent intervention to salvage as much tissue as possible. Endovascular intervention strategies aim at establishing inline flow to the palmar arch (PA) preferably via both radial artery (RA) and ulnar artery (UA) to safeguard digital perfusion. Frequently, antegrade recanalization of the RA or UA fails due to flush occlusion at brachial artery bifurcation or dense fibrotic occlusions precluding antegrade guidewire negotiation. The purpose of this study was to evaluate the efficacy of “palmar arch loop” technique for endovascular management of CHI by establishing inline flow to the PA via both RA and UA. To the best of our knowledge, this is the first case series in the world evaluating the efficacy of “palmar arch loop” technique, with retrograde percutaneous transluminal angioplasty (PTA) of the involved RA and/or UA.
Material and methods
The Uttar Pradesh University of Medical Sciences – Peripheral Artery Disease Registry contains meticulous records of all patients with a clinical diagnosis of peripheral arterial disease that underwent diagnostic peripheral angiography or therapeutic endovascular intervention in the Department of Cardiovascular and Thoracic Surgery since 2015. For this study, we retrospectively investigated the subset of patients in the registry presenting with CHI undergoing endovascular intervention using “palmar arch loop technique” at our center (n = 10) between April 2017 and March 2019. The procedure was explained to all the patients, as well as the possible complications, and written informed consents were obtained.
All patients were assessed clinically and investigated with a combination of imaging (duplex ultrasound, digital subtraction or computed tomography angiography) and physiologic measurements (peripheral capillary oxygen saturation, SpO2) prior to treatment. Selective subclavian arteriography/brachial arteriography were done via the right common femoral artery (CFA) access and antegrade revascularization was initially attempted in all the patients by the same access. Only those patients were included in this study that had diffuse involvement of the PA along with either or both of the arteries supplying it, with attempted retrograde PTA of the involved RA and/or UA by “palmar arch loop” technique.
All the patients were on dual anti-platelet therapy (DAPT) comprising of Ecospirin 150 mg plus Clopidogrel 75 mg and Cilostazol 100 mg for at least 12 days pre-intervention with minimal or no symptomatic improvement. All the patients had received low molecular weight heparin (LMWH) for at least a week post-acute event. None of them had undergone systemic or catheter-directed thrombolysis.
Retrograde PTA of RA in 50% (n = 5) and UA in 20% (n = 3) was done successfully by looping the guidewire across the PA, along with PTA of PA in all the patients. In patients with occlusion of both RA and UA, at least one of the two arteries could be engaged antegradely, followed by retrograde PTA of the other artery by looping the guidewire across the PA. All patients were followed up at regular intervals (weekly for a month, fortnightly for 3 months, and then at 6 and 12 months) with clinical assessment and SpO2 measurement. Study end points were technical success (defined as successful wire and balloon negotiation across the occlusion followed by uncomplicated angioplasty with residual stenosis ≤30%), hand healing (defined as ulcer healing and/or stump healing after amputation of necrotic/gangrenous tissue), and primary patency rate (defined as freedom from target vessel occlusion and reintervention of the target lesion during follow-up) at one year.
Intervention procedure
Endovascular procedures were performed in a dedicated angiographic suite under local anesthesia, sterile draping, and continuous monitoring. Right CFA access was initially performed in all cases (5 F, 10 cm long femoral sheath). Selective subclavian arteriography/brachial arteriography were done with 5 F multipurpose diagnostic catheter to delineate the lesions. Heparin was given intra-arterially to maintain an activated clotting time of 200–250 s.
An antegrade revascularization was initially attempted, in all the patients, using 0.014″/0.018″ guidewire (“V14/V18,” Boston Scientific/ “Fielder XT,” Asahi) with the support of either a low profile PTA balloon catheter (2 mm × 80 mm × 150 cm, “Sterling,” Boston Scientific) or support catheter (Rubicon 14/18, Boston Scientific) or both. Despite attempts with multiple guidewires/support catheters combinations, antegrade intraluminal/subintimal negotiation of the involved arteries failed. In patients with occlusion of both RA and UA, at least one of the two arteries could be negotiated antegradely intraluminally/subintimally.
Ipsilateral brachial artery (BA) access was established for attempted retrograde PTA of the involved RA and/or UA by “palmar arch loop” technique (5 F, 7 cm long radial sheath). Under DSA guidance/roadmap of the palmar arch, the patent RA/UA was selectively catheterized using balloon/support catheter mounted 0.014″ guidewire (V14, Boston Scientific). Once the guidewire was manipulated through the palmar arch, the distal part of the occluded RA/UA could be successfully engaged; then the balloon mounted guidewire was advanced proximally to the elbow and retrograde recanalization with sequential balloon angioplasty was performed with appropriately sized angioplasty balloon with inflation at nominal pressure for 2 min. PA angioplasty was done with either the same balloon that was used for support or a 1.5 mm × 80 mm PTA balloon catheter as per the vessel diameter (Figures 1 to 4).
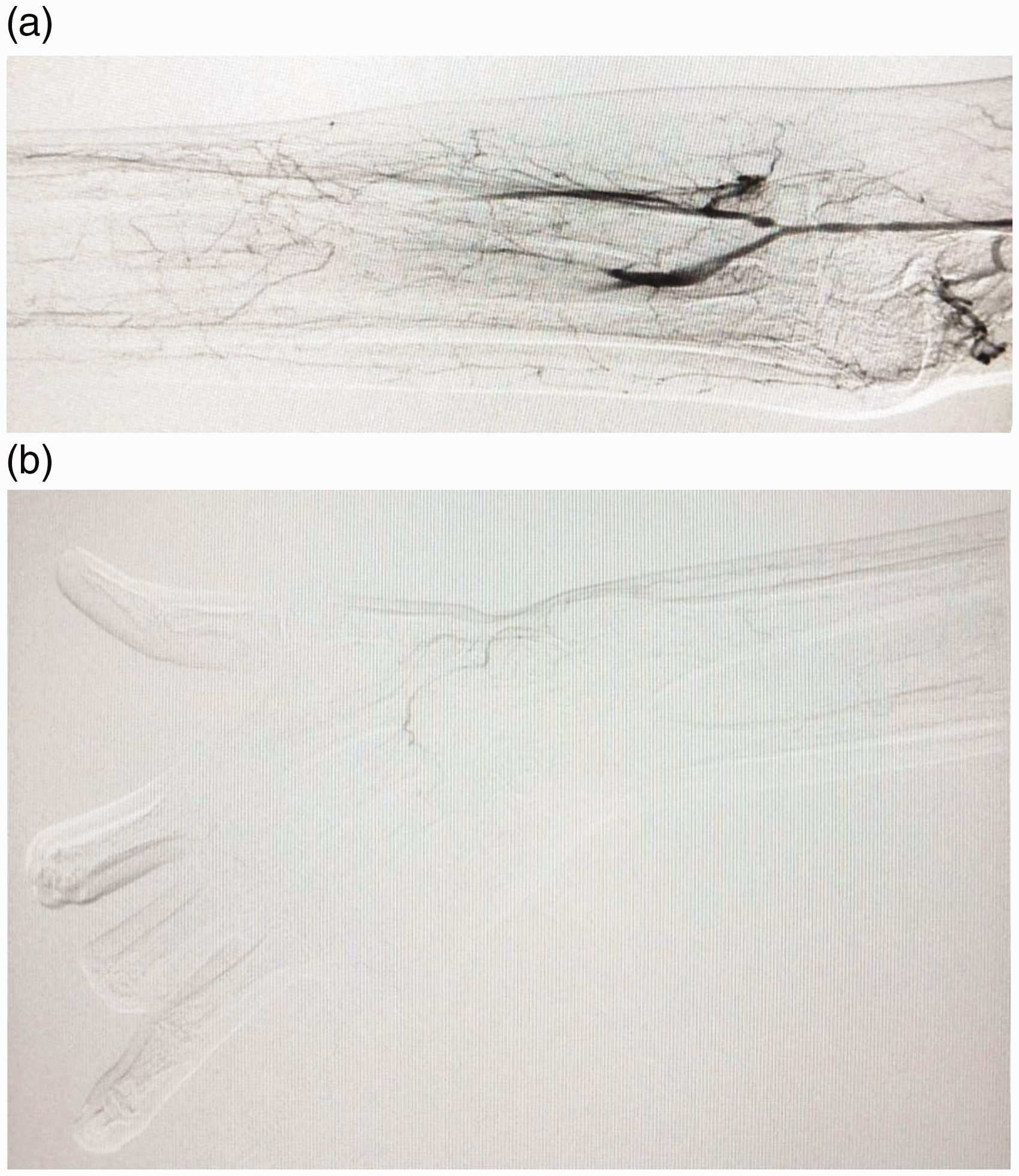
(a) Digital subtraction angiography of Rt. upper limb of a patient, with iatrogenic vascular injury due to inadvertent intra-arterial injection, revealing total occlusion of mid-distal RA & UA with tight stenosis of RA flush with BA (precluding antegrade guidewire negotiation for revascularization of RA). (b) Digital subtraction angiography of Rt. hand of the same patient revealing markedly reduced below-the-wrist collateral flow into the diffusely diseased deep palmar arch with no visible flow in the common and proper digital arteries.

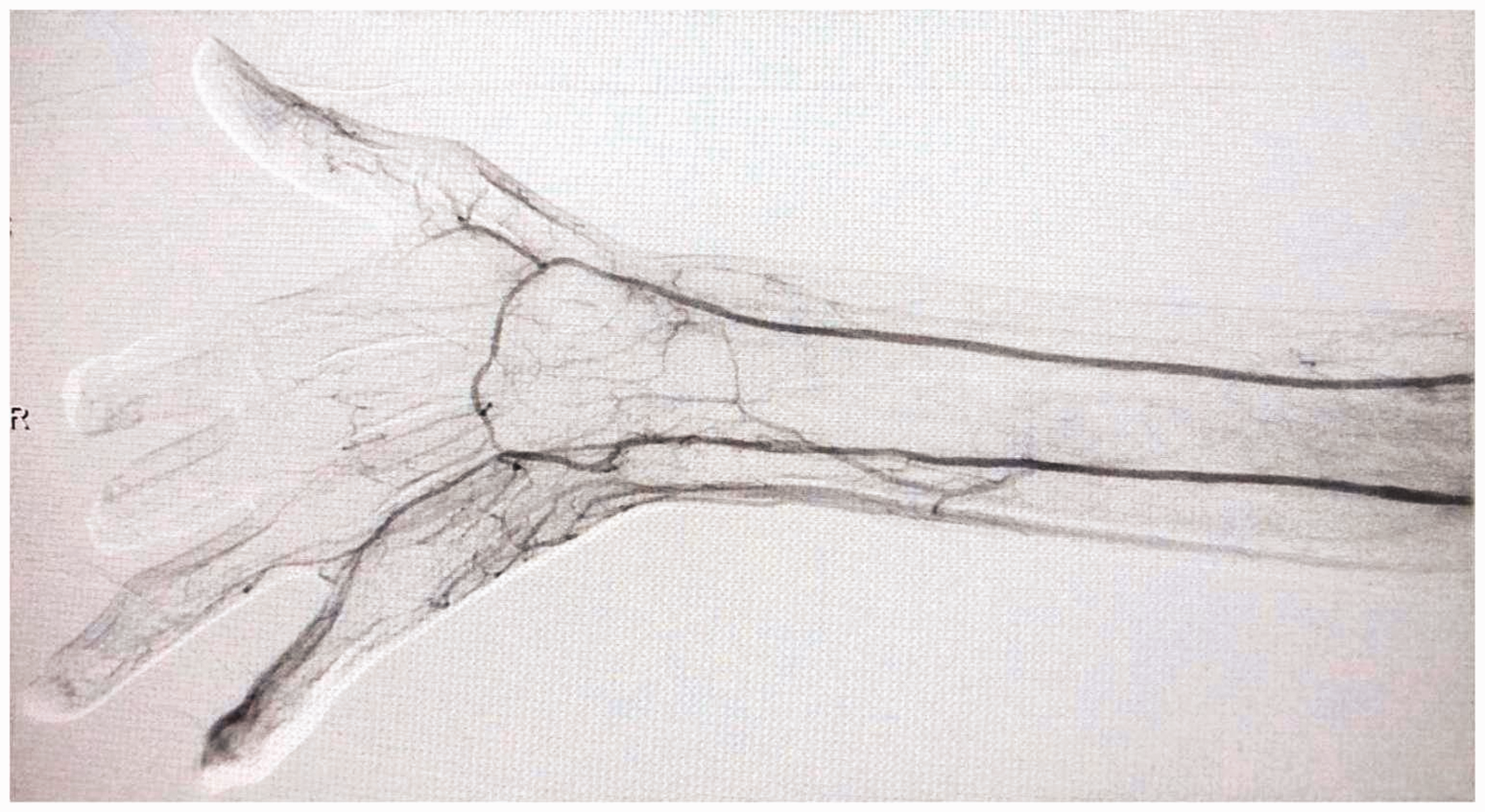
(a) and (b) Antegrade PTA of the UA done with good flow up to the wrist but poor flow in the palmar arch and distally.

(a) and (b) “Palmar Ach Loop” technique-0.014″ guidewire with the support of a low profile PTA balloon catheter was manipulated through the palmar arch and the distal part of the occluded RA could be successfully engaged; then the balloon mounted guidewire was advanced proximally to the elbow and retrograde recanalization of the RA and PA with sequential balloon angioplasty was performed.
Completion angiography confirming recanalization of the RA with good antegrade flow to the patent palmar arch, common and proper digital arteries via both the forearm arteries.
Intra-operative real time SpO2 monitoring of the digits was performed which revealed an increase (from 0 to 70% preoperative to 90 to 100% postoperative in all but one patient). After completion of angiography, confirming recanalization of the involved artery with good antegrade flow to the palmar arch and better visualization of common and proper digital arteries, the sheaths were removed and manual compression was applied for 10 min, followed by a non-occlusive pressure bandage for a day.
Post procedural care
DAPT (tablet Ecospirin 150 mg plus Clopidogrel 75 mg) was prescribed for 12 weeks followed by Ecospirin 150 mg thereafter. Cilostazol was continued in all the patients for 12 weeks. All the three patients with atrial fibrillation (AF) received oral anticoagulation (Warfarin) plus Ecospirin 150 mg with regular monitoring of International Normalized Ratio (INR). Aggressive risk factor modification therapy for diabetes, hypertension, dyslipidemia, and smoking was advised. Wound care protocol was strictly adhered to. All patients were followed up at regular intervals (weekly for a month, fortnightly for 3 months, and then at 6 and 12 months) with clinical assessment and SpO2 measurement. Conservative amputations of the gangrenous fingers were done in three patients after the establishment of clear line of demarcation. Duplex imaging of the target vessel was done in patients with recurrent ischemic symptoms or non-palpable arteries.
Results
Between April 2017 and March 2019, 10 patients (60% female; mean age 42 ± 18 years; mean time of presentation post-acute event 24 ± 11 days) underwent endovascular intervention using “palmar arch loop” technique at a single center in northern India.
Comorbidities were hypertension, diabetes, hyperlipidemia, and rheumatic heart disease (20% each); 40% were smokers/tobacco chewers, highlighting this significant health problem in developing countries.
Causes for CHI were: Iatrogenic injury due to inadvertent intra-arterial injection in 50% (n = 5) and thromboembolic event in 50% patients (n = 5). All the patients had unilateral limb involvement. In the study, vessels involved were: both RA and UA along with the PA in 50%; RA and PA in 30%; UA and PA in 20%. All of them had total occlusion of involved RA and/or UA (> 2/3rd of total length) with occlusion/diffuse disease of PA as well. All the patients had some degree of tissue loss/gangrene of one or more fingers and all of them had rest pain; 50% had ischemic changes over the palm and forearm as well (Table 1).
Baseline patient characteristics.
PTA of 12 forearm vessels was performed (7 RA and 5 UA) with antegrade PTA of 5 vessels (3 UA and 2 RA) and retrograde PTA by looping across the PA of 7 vessels (5 RA and 2 UA) along with PTA of PA in all the patients; 80% (n = 4) of the antegrade PTA performed were subintimal, whereas 70% (n = 5) of the retrograde PTA performed were intraluminal (Table 2).
Angiographic and procedural data.
Three patients with post angioplasty elastic recoil or residual stenosis (>30%) were managed successfully by repeat ballooning with prolonged inflation up to 3–4 min. No stent was deployed in our study. In two patients with coexistent significant BA stenosis (and subclavian artery stenosis in one of these), PTA was performed via the femoral approach before addressing the distal lesions. Post procedure subjective improvement in pain, improved warmth, and SpO2 at fingertips with palpable RA and/or UA at the wrist was observed in nine patients. All the patients were discharged in five to seven days.
Seventy percent technical success rate was achieved ensuring inflow to PA via both the arteries with improved flow distally to the common and proper digital arteries. In a patient with occlusion of both RA and UA along with PA, antegrade revascularization of RA and PA was successful but retrograde negotiation of guidewire through the occluded UA failed. Retrograde PTA failed in a patient with occlusion of RA and another patient with occlusion of UA, though PTA of diffusely diseased PA was done successfully in both the patients.
Primary patency rate was 85.7% in one year. A patient with significant restenosis of RA four months post procedure underwent reintervention with successful antegrade PTA with drug-coated balloon (DCB).
Ninety percent showed subjective improvement in pain with healing of the lesions and/or formation of clear line of demarcation with reversal of pregangrenous changes proximally. In a female patient with ulceration at the 4th and 5th fingertips, retrograde recanalization of occluded UA failed and despite PTA of the diffusely diseased PA no clinical improvement was seen; she was managed conservatively and is under follow-up. All the five patients with ischemic changes over the palm and forearm showed complete improvement.
Out of the eight patients with gangrene of fingers, three underwent minor amputation of the gangrenous digits and five underwent auto-amputation of the gangrenous tissue with complete healing of the stump. No access site-related complication or mortality was encountered during the study period (Figures 5 and 6).

(a) and (b) Patient-1 (pre intervention): Gangrene of fingertips with pregangrenous changes up to the metacarpo-phalyngeal joints; discoloration over the hypothenar eminence, mid palm, wrist and distal forearm. (c) and (d) Patient-1 (post intervention – 2 months): Formation of clear line of demarcation at the distal interphalangeal joints, healing of all other lesions with salvage of the hand.

(a) and (b) Patient-2 (pre intervention): Ascending gangrene of the 2nd and 3rd finger, ulceration at the 4th and 5th fingertips with pregangrenous changes over the fingers, palm and mid-forearm. (c) and (d) Patient-2 (post intervention – 6 months): Complete healing of stump and fingertips ulcers, reversal of changes over the fingers, palm and forearm with salvage of the hand.
Discussion
CHI is most frequently caused by thromboembolic disease and acute traumatic or iatrogenic arterial injury. Occlusive disease of the infrabrachial arteries is rare even in patients with diabetes and chronic renal failure. 1 In developing nations, iatrogenic arterial injuries are frequently encountered as patients in rural areas are often treated by non-physician health care workers or even quacks, who inadvertently inject drugs into the brachial artery instead of a vein. The patients suffer from acute onset pain, discoloration, ulceration, necrosis starting at the fingertips and ascending gangrene of the fingers. 2 , 3 The problem is accentuated by delayed referral to higher/tertiary centers as the perpetrator unwisely tries to manage the patient conservatively in fear of medico-legal implications. There is no definitive surgical management protocol in this particular subset of patients. In this world of medico-legal litigations, even surgeons refrain from taking up high risk vascular cases with ascending gangrene lest the onus of amputation is shifted on them instead of the primary culprit or even patient’s carelessness.
In our study, 50% of the cases were due to such iatrogenic injury with diffuse involvement of both the forearm vessels causing CHI. These patients were managed conservatively by physicians at the primary health centers and referred to our tertiary center equipped with endovascular intervention facilities after the onset of gangrene or tissue necrosis. It is a well-known fact that the endovascular world is transgressing the open surgical boundaries and foraying into extreme revascularizations at such prolific a pace that many primary health care professionals have not been able to keep themselves abreast of these contemporary innovations. For example, finger gangrenes are often referred to plastic surgeons since they have been taking care of finger amputations with microsurgical anastomosis. Likewise, as happened in our study, diabetic patients with digital gangrene are usually treated for spreading cellulitis and hyperglycemia for days before even a Doppler is performed and referred to vascular surgeons after the window period ruling out open surgical intervention.
Urgent embolectomy is the standard of care in patients with thromboembolic events and most of the patients are in fact managed accordingly. The unlucky few, particularly poor patients from rural background, resort to taking consultation from village quacks or even local pharmacists who load them with analgesics which conveys a false sense of recovery for a few days. Only when they start noticing ulceration or frank gangrene do they contemplate medical consultation. The delay, in days, renders them a poor candidate for successful embolectomy of distal forearm vessels.
The onus lies on the vascular fraternity to propagate the results of these technological innovations on reputed platforms as a confidence building measure for the healthcare practitioners as well as the patients. Developing countries with an overburdened health care system due to population overload often face these issues which need to be addressed systematically.
CHI with advancing gangrene of digits requires urgent intervention to salvage as much tissue as possible, as conservative therapy is often inadequate to address the ischemia appropriately, particularly in patients with delayed presentation. In our study, the mean time of presentation post event was 24 ± 11 days, precluding catheter-guided thrombolysis or thromboembolectomy. Most of the patients were already on low molecular weight heparin and/or antiplatelets which were ineffective in containing ascending gangrene of the fingers.
Conventionally, open surgical procedure to bypass the forearm arteries may be performed but concomitant diffuse involvement of the arteries along with the PA would limit the procedural efficacy due to improper landing zone or inadequate distal run-off. Bypass procedures are not feasible in the setting of complete occlusions of both the forearm arteries along with the palmar arches. Only a few cases have been reported regarding PTA of below-the-elbow (BTE) occlusions.4–11
Ferraresi et al. 5 evaluated the outcomes of PTA of BTE disease causing critical hand ischemia in 28 patients. The inter-osseous artery was disease free in all the cases with involvement of both RA and UA in 90% cases with mean lesion length greater than 10 cm. They reported a technical success rate of 82% and hand healing rate of 65%.
Gandini et al. 6 reported percutaneous transluminal angioplasty for treatment of critical hand ischemia by retrograde recanalization of the UA using radial-to-ulnar artery loop technique, with complete healing of fingertip ulceration at six months (Table 3).
Summary of different endovascular revascularization techniques in CHI.
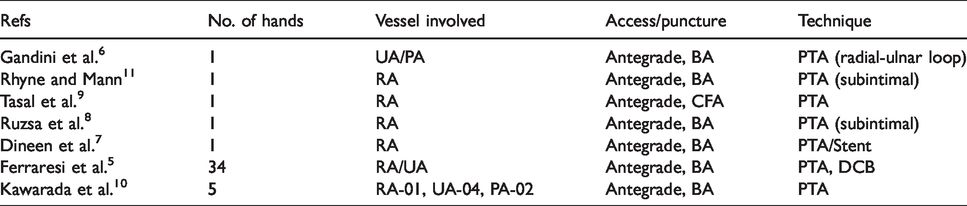
Endovascular intervention strategies aim at establishing inline flow to the PA preferably via both RA and UA to safeguard digital perfusion. The advent of dedicated and improved hardwares (low profile PTA balloons, support catheters, chronic total occlusion guidewires with loaded tips, guidewires with shapeable tips etc.) has established percutaneous intervention as an effective treatment modality for symptomatic upper limb ischemia.7,8
In our experience, it is preferable to recanalize both the forearm arteries, in the presence of PA involvement, since it will serve as an insurance policy in the event of any future restenosis and/or reocclusion of the PA, ensuring perfusion of the common and proper digital arteries by either/both the forearm arteries. The ischemic changes reverted earlier and better in our patients in whom inline flow was established to the palmar arch via both RA and UA. This strategy is also justified in patients of CHI with associated diffuse ischemic changes over the forearm and pain on exertion/rest pain. Our strategy in cases with occlusions of both the arteries was antegrade revascularization regardless of the sequence. First vessel to cross was decided by the ease of wire passage, ascertaining in-line flow up to the palmar arch at least by that single vessel, before focusing on its counterpart.
Frequently, antegrade recanalization of the RA or UA fails due to flush occlusion at brachial artery bifurcation or dense fibrotic occlusions precluding antegrade guidewire negotiation. 3 Such difficult occlusions can be dealt with by advancing the guidewire antegradely via the patent forearm artery up to the PA, with balloon or catheter support, and then negotiating the involved artery retrogradely up to the brachial artery, and performing sequential retrograde PTA. In cases where negotiation of the balloon retrogradely over the guidewire is difficult, the guidewire can be withdrawn up to the BA and renegotiated antegradely into the occluded vessel over the previously created guidewire track and antegrade PTA can then be performed over it. We have used the term palmar arch to denote either of the arches – superficial or deep; though technically it is easier, due to anatomical continuity, to loop across the superficial palmar arch via the UA and the deep palmar arch via the RA. Targeting either of the arches for PTA is effective for hand salvage, as evident from our study, due to extensive collateral circulation between the two.
As shown in our study, 90% of patients showed formation of clear line of demarcation with reversal of pregangrenous changes proximally and healing of the lesions. Our strategy was to refrain from aggressive debridement or early amputation, allowing the healthy granulation tissue to “outgrow” the gangrenous distal part over a few weeks, ensuring maximum tissue salvage. Post revascularization, these patients show immediate subjective improvement in the pain, paraesthesia may persist distally though. Five patients underwent auto-amputation of the gangrenous tissue with complete healing of the stump.
This technique is a natural extension of the experience that has been acquired by performing “pedal-plantar loop technique” for below-the-knee (BTK) endovascular revascularization in critical limb ischemia (CLI). 12 We also have applied the technical skills and experiences that we have gained over the years in BTK interventions for CLI, for salvaging the hands of these CHI patients. To the best of our knowledge, this is the first case series describing the efficacy of “palmar arch loop” technique, with retrograde PTA of the involved RA or UA. The emphasis in this study has not been just on technical or procedural aspect, but the follow-up and approaches to successful hand healing too. These findings and results can be instrumental in providing an objective insight on salvaging tissue in critical hand ischemia due to diverse etiologies.
There were certain limitations to our study. This was a retrospective observational study with a small sample size given the stringent inclusion criteria; hence, the potential for selection and information bias exists. Also since our series represents the experience of one operating endovascular surgeon at a single institution, the results are subject to the influence surgeon experience and patient selection preferences. The pre and post procedure medical management protocol was not uniform; it was rather tailored to specific patient profile. The small sample size, heterogeneity of treated arterial segments and the medium term follow up, should also be considered in the interpretation of these results. The results cannot be extrapolated, until proven safe and efficacious, in the setting of atherosclerotic chronic disease of the below-the-elbow vessels causing significant vascular compromise distally. More study is required to assess the long-term outcomes of this technique in this particular patient subset.
Conclusions
Endovascular management of CHI by “palmar arch loop” technique is an efficient technique to deal with occluded forearm vessels, particularly when antegrade recanalization fails. This technique, with good technical success and patency rates, is potentially a unique tool in the endovascular armamentarium for salvaging hand.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.