
Abstract
Objectives
Endovascular repair (ER) of popliteal artery aneurysm (PAA) is an alternative to open repair. However, there is no standardized protocol for when to opt for ER and the decision is therefore at the discretion of the clinician. This study aims to evaluate the adherence to the Instruction For Use (IFU) in patients undergoing ER for PAA and factors associated with stent graft patency at one year.
Methods
The adherence to IFU provided by the manufacturer in 55 patients treated with Gore Viabahn® Endoprosthesis with Heparin Bioactive Surface for PAA between 2009 and 2019 were retrospectively analyzed. Duplex follow-up was performed at 30 days and one year.
Results
The two groups of patients treated within (n = 10) and not within (n = 45) IFU did not differ in patient demographics, diagnostic assessment, treatment or outcome. Forty-five patients (81.8%) received stent graft placement with at least one deviation according to IFU. Distal oversizing >20% was the most frequent deviation against IFU (n = 22, 40.0%). Primary patency at one year was 72%. Diameter size difference >1 mm between overlapping stent grafts (6/14 [43%], p = 0.013) and renal insufficiency (5/12 [42%], p = 0.0086) were associated with lower primary patency at one year. Age-adjusted analysis of tortuosity index (HR 1.78/SD, 95% CI 1.17–2.71; p = 0.0071) and maximal PAA angle (HR 1.73/SD, 95% CI 1.018–2.95; p = 0.043) were associated with major amputation/mortality at end of follow-up.
Conclusion
The majority of patients undergoing ER for PAA were not treated within IFU. Diameter size difference >1 mm between overlapping stent grafts was associated with a higher loss of primary patency at one year. Multi-center studies with larger sample size and long-term follow up of patency are warranted.
Keywords
Introduction
Open surgical repair (OR) with bypass graft has long been considered the gold standard for treating popliteal artery aneurysm (PAA), but since the introduction of endovascular repair (ER) there is a possibility to treat patients with a less invasive method also showing satisfying results. 1 One small randomized trial published in 2005 showed similar patency rates between OR and ER for asymptomatic PAA at one year. 2 However, some reports have indicated lower primary patency and a higher risk of major amputation after ER compared to OR,3,4 which could be seen as an argument for reserving ER to patients with high age and high level of comorbidities. Still, there is a lack of contemporary randomized controlled trials comparing outcome after ER and OR and there is an ongoing debate regarding which patients should be offered ER.
At Vascular Center, Skåne University Hospital, Malmö, Sweden, there has been an increase in the use of ER of PAA during the last decade. 5 Retrospective studies from this center have shown that the decision for choosing ER or OR when treating PAA is based on the discretion of the vascular surgeon in the majority of cases.5,6 Though Instruction For Use (IFU) are provided by stent graft manufacturers, there is no standardized protocol for when to choose ER or OR, respectively.
The aim of this study was to evaluate adherence to the IFU in patients undergoing ER for PAA. A secondary aim was to evaluate factors associated with patency at one year.
Methods
Study design
Patients undergoing ER for PAA between 1 January 2009 and 1 February 2019 at Vascular Center, Skåne University Hospital, Malmö were retrospectively identified by searching the International Classification of Diseases, 10th revision (ICD-10) diagnosis code I72.4 (aneurysm of lower extremity artery). Criteria for inclusion were true aneurysms within the popliteal artery and treated by at least one Gore Viabahn® Endoprosthesis with Heparin Bioactive Surface (W. L. Gore & Associates, Inc, Flagstaff, Arizona). The study complies with the Strengthening the Reporting of Observational studies in Epidemiology (STROBE) statement for cohort studies (Appendix, Table 1). In total, 55 patients were included in this single-center study (Figure 1). Data were collected from patients’ medical charts.
Descriptive variables according to IFU.
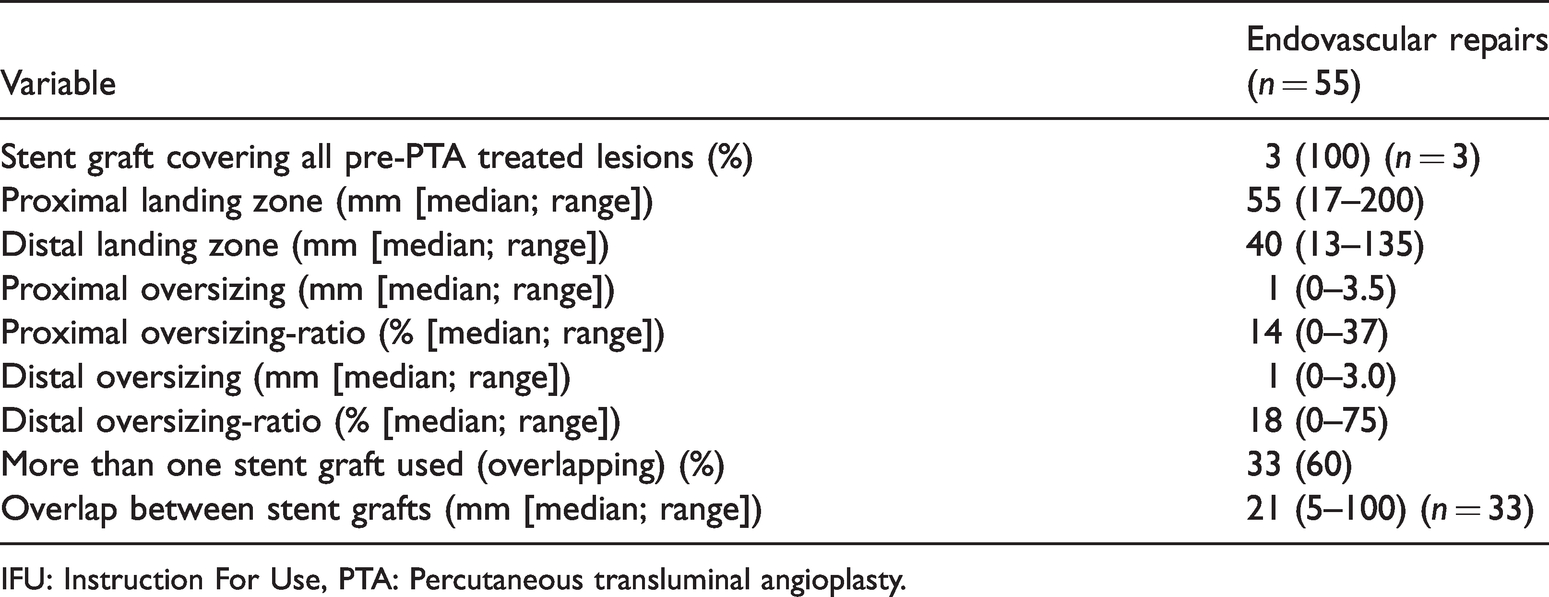
IFU: Instruction For Use, PTA: Percutaneous transluminal angioplasty.
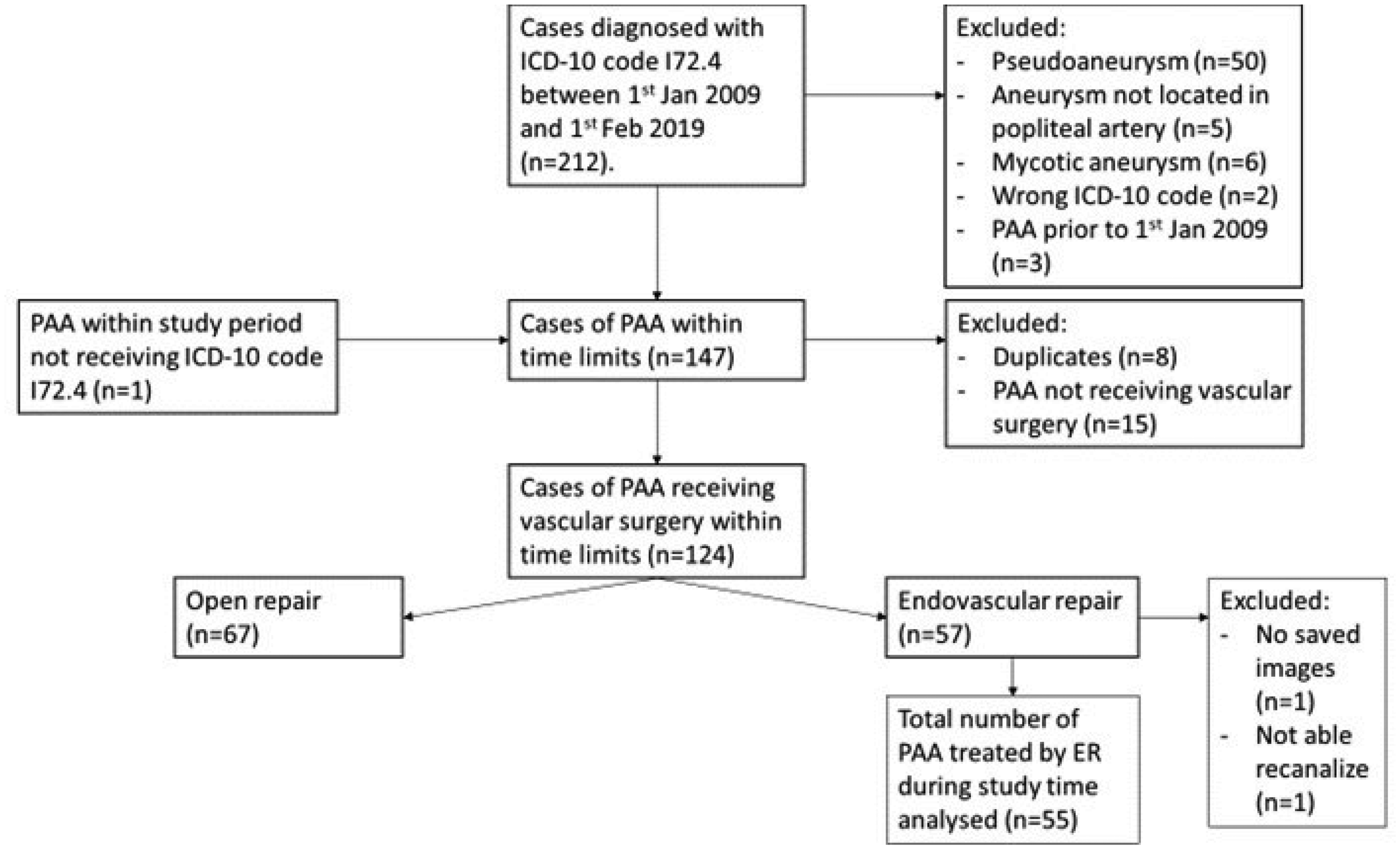
Flow chart illustrating inclusion and exclusion of patients.
Instructions for use
In order to determine if the placement of a stent graft was consistent with IFU a series of variables were extracted from the document “Instructions For Use For: Gore Viabahn® Endoprosthesis” provided by W. L. Gore & Associates, Inc, Flagstaff, Arizona. 7 Variables extracted were: (1) stent graft covering all stenotic lesion, if pretreated by percutaneous transluminal angioplasty (PTA) prior to stent graft placement; (2) landing zone at least 20 mm both proximal and distal to the aneurysmal lesion; (3) stent graft diameter being 5–20% larger than the healthy vessel diameter immediately proximal and distal to the lesion (oversizing); (4) if two or more stent grafts are used, stent graft should overlap at least 20 mm; (5) if stent grafts of different sizes are used, stent graft with larger diameter should be telescoped into stent graft with a smaller diameter; (6) the diameter of two overlapping stent grafts should not differ more than 1 mm (exception when using a 13 mm diameter stent graft to overlap with a 11 mm diameter stent graft); (7) an overlapping stent graft should not end in the “No Overlap Zone”.
Definitions
The popliteal artery was considered aneurysmal (PAA) if the artery’s maximal diameter was wider than 15 mm or wider than 1.5 times the adjacent proximal/distal arterial segment. The PAA’s maximum diameter was measured through the shortest diagonal distance at the broadest segment of the popliteal artery by either computed tomography angiography (CTA) or magnetic resonance angiography (MRA). Maximal PAA angle was defined as the greatest angle able to measure by analyzing either pre-operative CTA or MRA images (Figure 2). Tortuosity index (TI) was defined as the ratio between the distance of the Euclidean line (between the end of Hunter’s canal and the branching of the anterior tibial artery) and the actual length of the popliteal artery 8 (Figure 3). The landing zone was defined as the length of non-aneurysmatic artery covered by stent graft, either proximal or distal. Oversizing was defined as the ratio between maximal stent graft diameter and maximal diameter of the artery at which the stent graft ended, either proximal or distal. Overlap was defined as the length of stent graft covered by another stent graft, when treating a PAA with more than one stent graft. If there were more than one overlap (three or more stent grafts), the shortest overlap was documented. “No Overlap Zone” was defined as a segment of the popliteal artery starting 3–4 cm proximal to the radiographic knee joint and extending another 4 cm proximally.

Image in DSA with measurement of maximum angle of 60°.
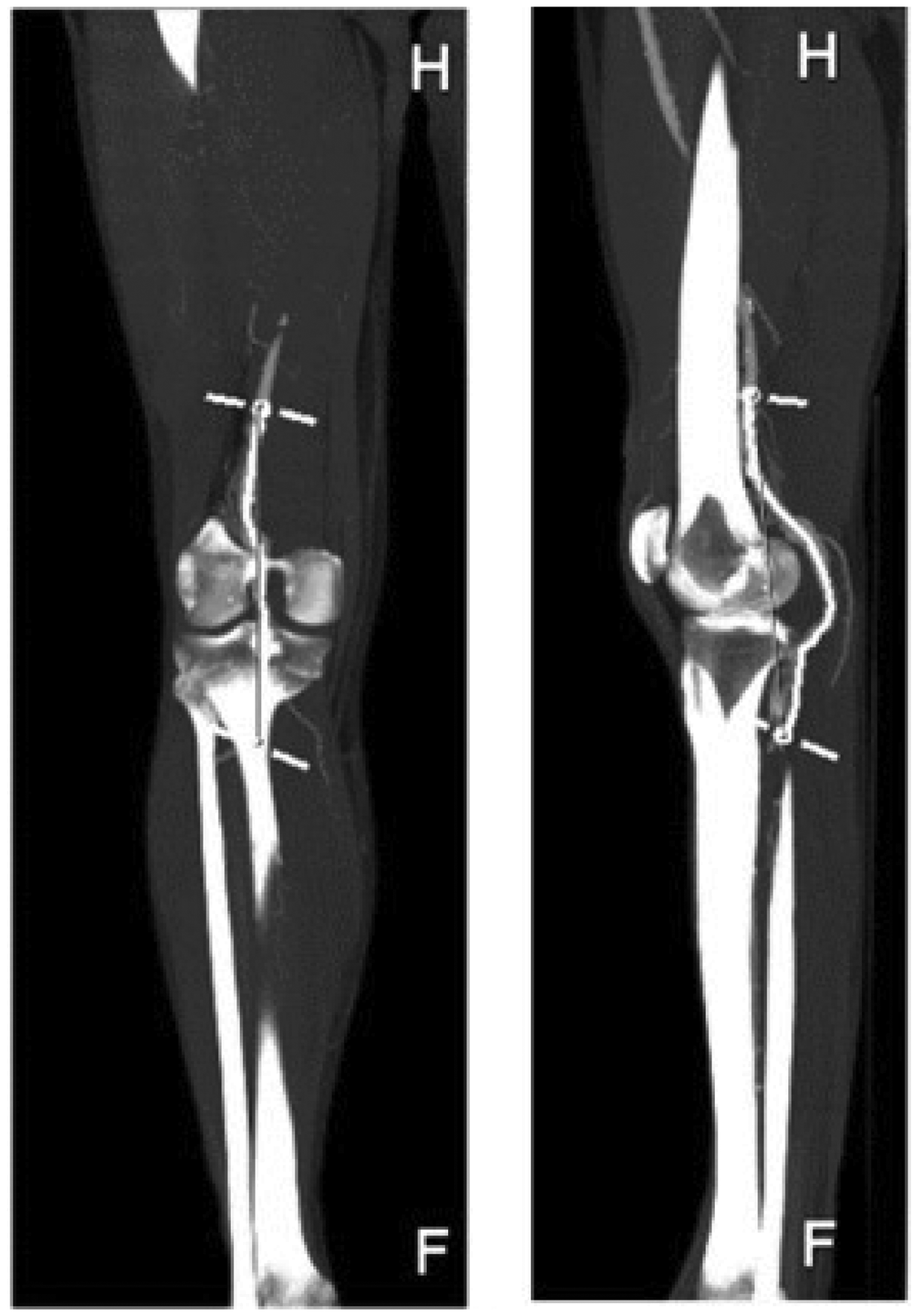
Measurements of TI in TeraRecon. The curved, thick white line marks the center line (natural course of the vessel); the straight, thin grey line marks the Euclidean line.
The distal run-off was defined as having either three, two, one or none calf arteries/artery patent, and was assessed by either duplex ultrasonography, CTA or MRA.
A list of definitions9–11 is outlined in Appendix; Table 2.
Reasons to why the ER was not consistent with the IFU.
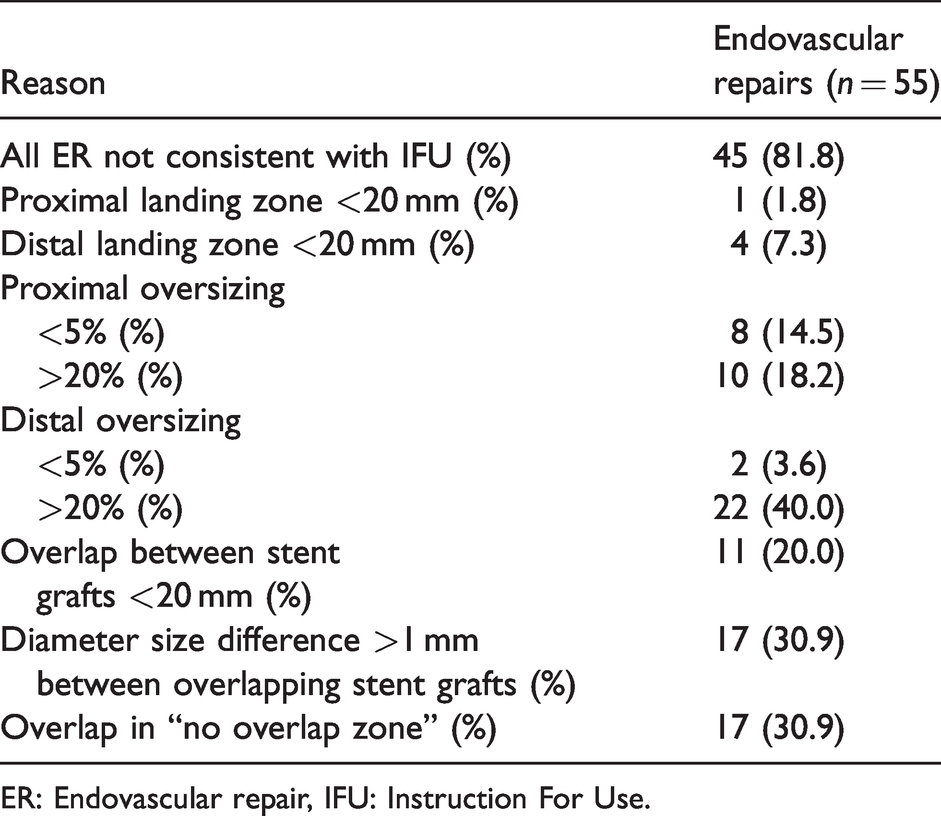
ER: Endovascular repair, IFU: Instruction For Use.
Pre-operative imaging
Pre-operative imaging was done with computed tomography angiography (CTA) (n = 32) or with magnetic resonance angiography (MRA) (n = 23). All CTA studies were performed with iodinated contrast media, and MRA studies were performed with gadolinium contrast media. In both imaging modality protocols, scanning was done from hemidiaphragms to the forefoot. The systems used for CTA were Siemens Somatom Definition Flash (Siemens Healthineers, Erlangen, Germany) or Canon Aquilion One (Canon Medical Systems, Ōtawara, Tochigi, Japan). The MRI scanners were Siemens Magnetom Symphony 1.5 Tesla or Siemens Magnetom Avanto 1.5 Tesla (Siemens Healthineers, Erlangen, Germany).
Follow-up
Termination of follow-up was defined by either major amputation of the treated leg, death or the defined end of follow-up date (11 March 2020). At this date, all patients were checked for survival in the national population registry.
Data on patients treated for PAA are entered into the Swedvasc registry, as well as the results from a routine clinical and duplex-ultrasound (DUS)-based surveillance program, at both 30 days and one year post intervention.
Statistical analysis
All statistical analyses were done through SPSS (version 25.0, IBM, Chicago, IL, USA). Nominal and ordinal data were presented as frequencies together with percentages. Continuous variables were presented as median together with either range or interquartile range (IQR). Evaluation of group differences was analyzed using Pearson’s Chi-Square or Fisher’s Exact test when analyzing nominal data. Evaluation of group differences was done using Kendall’s Tau-b test when analyzing ordinal data. For continuous data, group comparisons were analyzed using Mann-Whitney U test. Amputation-free survival between groups was analyzed using Log Rank test. A Cox Regression analysis was used to investigate possible association between age-adjusted tortuosity index or age-adjusted maximal angle, respectively, and major amputation/mortality, and expressed in terms of Hazard ratios (HR) with 95% confidence intervals (CI). TI and maximal PAA angle were evaluated with the Kolmogorov-Smirnov test for distribution characteristics. TI and maximal PAA angle were found to be skewed distributed and were log-transformed. TI and maximal PAA angle were expressed per one standard deviation (SD) increment in the multivariable Cox proportional hazard models. No imputation of data was performed due to loss of follow-up or when data was missing. All available data was used when performing the calculations. Hence, patients were not excluded if there was no full data set. For all analyses, a p-value of 0.05 or less was considered significant.
Results
Variables according to IFU
Among 55 patients, 10 (18.2%) were treated within IFU. Descriptive variables of all 55 patients are outlined in Table 1. Among 45 patients not treated within IFU, distal oversizing > 20% was the most frequent deviation from IFU (n = 22, 40.0%), followed by overlapping stent graft in “No Overlap Zone” and size difference > 1 mm between overlapping stent grafts (for both variables n = 17, 30.9%) (Table 2).
Patient demographics
There was no demographic difference between patients treated within versus not within the IFU (Appendix; Table 3).
Diagnostic assessment prior to ER of PAA in relation to IFU.
ALI: acute limb ischaemia; IFU: Instruction For Use; IQR: interquartile range; PAA: popliteal artery aneurysm.
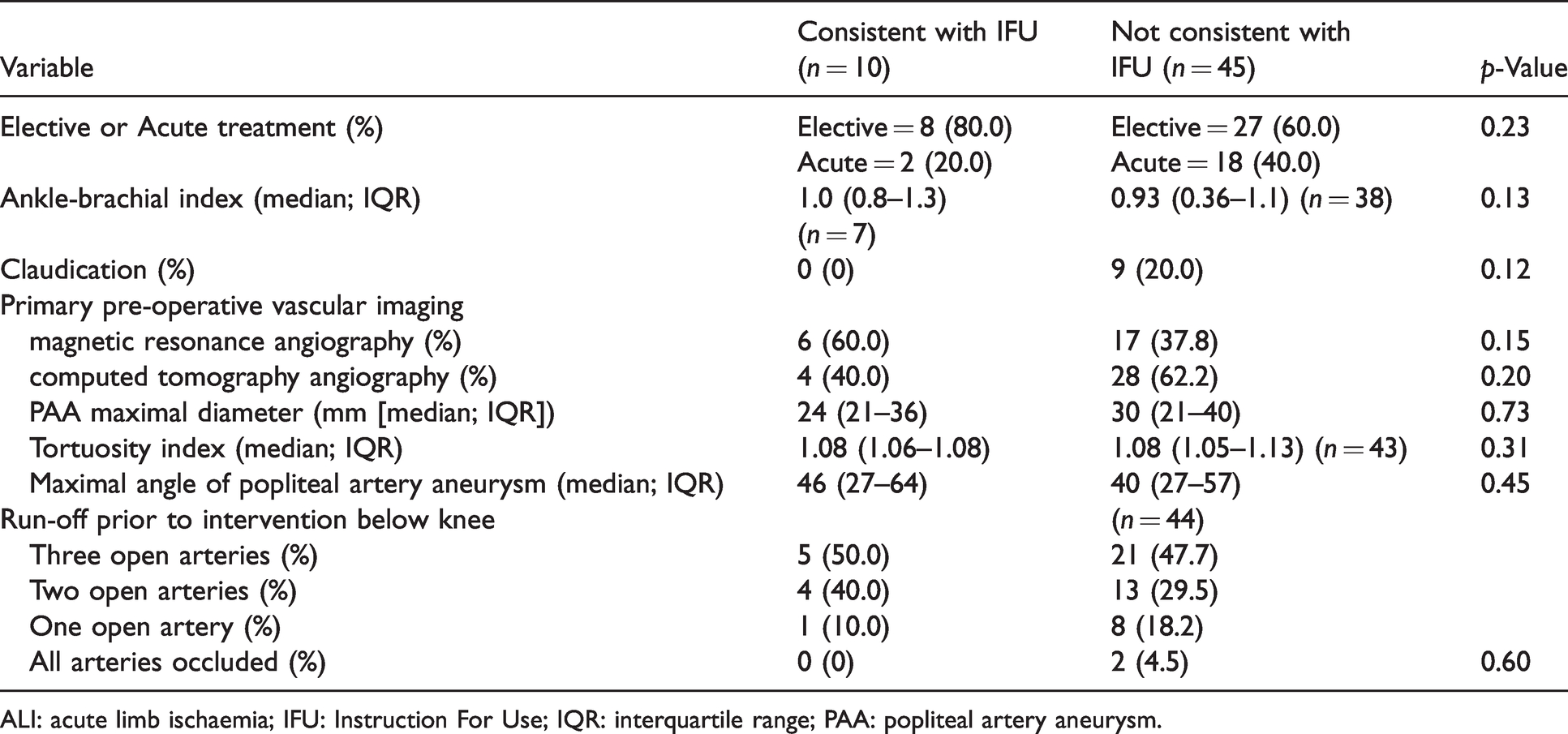
Diagnostic assessment
The proportion of patients suffering acute limb ischaemia (ALI) did not differ between patients treated within versus not within IFU (Table 3). One patient (10.0%) in the group treated within IFU, and one patient (2.2%) in the group not treated within IFU underwent ER due to ruptured PAA.
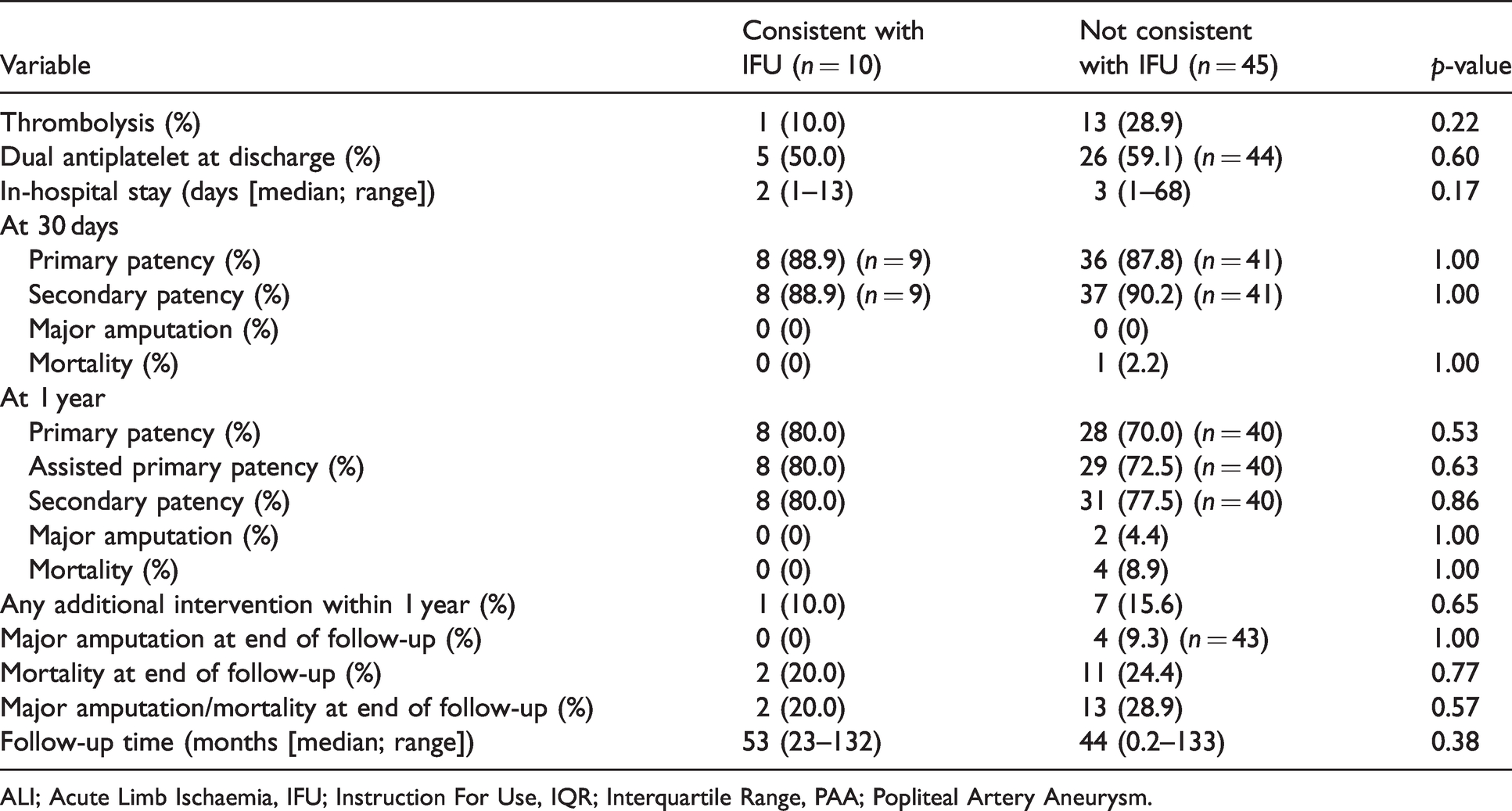
Treatment and stent grafts
In total, 96 Viabahn stent grafts were used to treat 55 PAAs. There was no difference in numbers of stent grafts used per PAA between the group treated within IFU (median = 1, range 1–2) and the group not treated within IFU (median = 2, range 1–3, p = 0.11). Antegrade and retrograde puncture were performed in 23 and 31 patients, respectively. One patient was first treated with thrombolysis through retrograde puncture and then received two stent grafts through antegrade puncture. Fourteen patients (25.5%) with ALI were treated with intra-arterial thrombolysis prior to stent graft placement. Dual antiplatelet therapy (DAPT) at discharge was prescribed to 31 (56%) patients (Table 4).
Treatment and outcome in patients treated consistent/not consistent with the IFU.
ALI; Acute Limb Ischaemia, IFU; Instruction For Use, IQR; Interquartile Range, PAA; Popliteal Artery Aneurysm.
The diameter of the Viabahn stent grafts used were 6 mm (n = 9), 7 mm (n = 19), 8 mm (n = 28), 9 mm (n = 6), 10 mm (n = 26), 11 mm (n = 3) and 13 mm (n = 5). The lengths of stent grafts used were 25 mm (n = 2), 50 mm (n = 13), 100 mm (n = 50), 150 mm (n = 13) and 250 mm (n = 18).
Outcome after endovascular repair in relation to IFU
There were no differences in 30-days or one-year patency, major amputation or mortality between the group treated within IFU and the group not treated within IFU. There was no difference in follow-up time between patients treated within and not within IFU, respectively (median 53 vs. 44 months, p = 0.38) (Table 4).
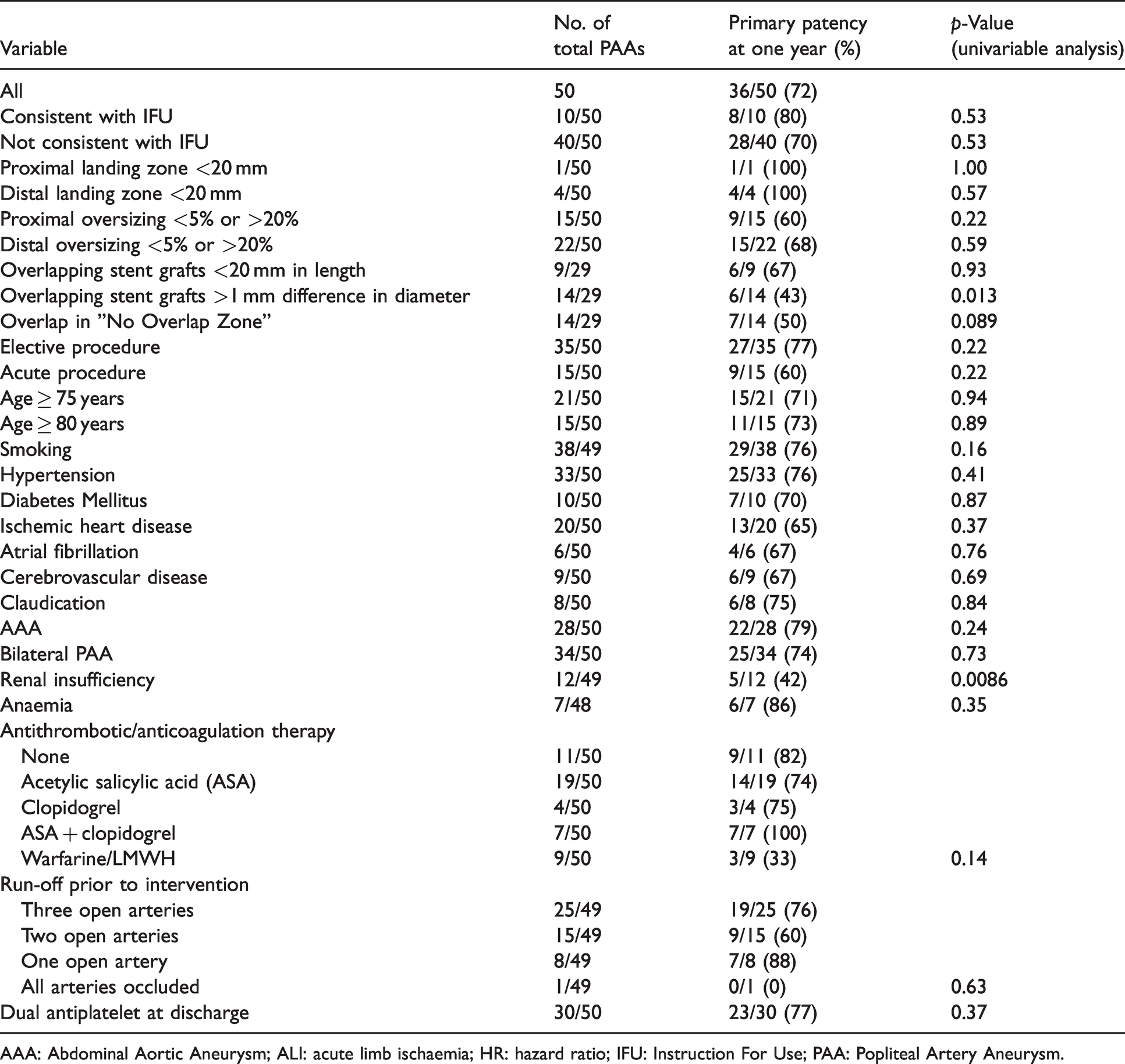
Factors associated with primary patency at one year
TI (p = 0.41) and maximal PAA angle (p = 0.62) were not associated with primary patency at one year. Patients treated with overlapping stent grafts with >1 mm difference in diameter had a higher loss of primary patency at one year than patients treated with overlapping stent grafts having ≤1 mm difference in diameter (p = 0.013). Renal insufficiency was associated with higher loss of primary patency at one year (p = 0.0086) (Table 5).
Factors associated with primary patency at one year.
AAA: Abdominal Aortic Aneurysm; ALI: acute limb ischaemia; HR: hazard ratio; IFU: Instruction For Use; PAA: Popliteal Artery Aneurysm.
Factors associated with major amputation/mortality during follow-up
There was no difference in long-term amputation-free survival between the group treated within the IFU and the group not treated within the IFU (p = 0.48). Neither was there any association with major amputation/mortality when analysing the IFU variables (proximal/distal landing zone, proximal/distal oversizing, stent graft overlap length, size of overlapping stent grafts and overlap in “No Overlap Zone”) separately. In a univariable analysis, acute procedures (p = 0.042), age >75 years (p = 0.0016), atrial fibrillation (0.0025), abdominal aortic aneurysm (p = 0.0055), anaemia (p = 0.00030), TI > 1.1 (p = 0.019) and maximal angle >60° (p = 0.0025) were all factors associated with major amputation/mortality. Age-adjusted analysis of TI (HR 1.78/SD, 95% CI 1.17–2.71; p = 0.0071) and maximal PAA angle (HR 1.73/SD, 95% CI 1.018–2.95; p = 0.043) showed an association with major amputation/mortality.
Discussion
The present study showed that more than 80% of patients receiving Viabahn® stent grafts due to PAA were not treated within the IFU provided by the manufacturer. One recent report found that 39.3% of PAAs were not eligible for Viabahn® in accordance to IFU. 12 The described discrepancy of non-adherence to IFU might be that the present study reports from a very endovascular-oriented center inherently associated with a higher rate of IFU deviations. The present report appears to be the first to examine the adherence to IFU when treating PAA with stent grafts and analyze the relationship between IFU adherence and outcome. Primary patency at one year was 72%, which is lower than the reported 84% in a recent series. 13 However, this series 13 seemed more selected with a frequency of acute limb ischemia in merely 2.7%.
Deviation from IFU regarding adequate oversizing was most frequent, with proximal and distal oversizing inconsistent with IFU in one-third and nearly half of all cases, respectively. The single most common deviation from the IFU was distal oversizing >20% in 40%, which seems to suggest that clinicians believe in opting for a larger stent graft diameter to achieve better patency rates. Stent graft diameter size difference >1 mm between stent grafts was the second most common deviation from the IFU, alongside overlap being present in the No Overlap Zone. A practical reason for not following the IFU could be a lack of fitting stent graft dimensions available for the clinician at time of intervention, especially since 36% underwent acute ER, despite of a large consignment of Viabahn® stent grafts. Of note, these stent grafts are relatively expensive and theatres may therefore not keep every size in stock. 14 A logistical reason favouring emergent stent graft procedures compared to open vascular surgery for PAA in the present study, inherent with IFU deviations, is the performance under local anesthesia, assistance by own staff and using facilities that is part of the vascular department. Whatsoever, patients not treated within IFU appeared to do as well as those treated within IFU.
Diameter size difference >1 mm between stent grafts was shown to be associated with loss of primary patency at one year in a univariate analysis. This finding underscores the importance of careful pre-operative planning and a wide selection of stent grafts when treating PAA. This also highlights the problems related to the large diameter difference between the healthy proximal and distal popliteal artery: a stent graft placed at the proximal landing zone has to be wider than the stent graft placed at the distal landing zone. Subsequently, there is a risk of overlapping stent grafts with a diameter difference >1 mm. In theory, one way to bridge this obstacle could be to introduce a tapered stent graft. However, this has not been tested, and there is currently no tapered stent graft with the indication for treating PAA.
The found association between renal insufficiency and increased risk of loss of stent graft patency is unknown. Individuals with renal insufficiency may suffer from increased arterial stiffness, a pathophysiological factor linking patients with cardiovascular disease, peripheral arterial resistance and kidney disease. 15 As the association between arterial stiffness and kidney disease may be mutual, a duplex-guided ER of PAA may be an attractive option to avoid use of contrast agents and spare renal function in particular patients with renal insufficiency. 16 , 17
Interestingly, age-adjusted TI and maximal PAA angle were associated with increased risk of combined major amputation/mortality during follow-up. These arterial abnormalities may be seen as markers of arterial disease severity, increased risk of complications and stent graft occlusion after endovascular repair, accelerated aging and mortality.18–22 Patients with very tortous and angulated PAA may perhaps be better treated by open repair. However, research on the consequences of tortuosity in patients treated endovascularly for PAA specifically is scarcely explored 8 and needs to be evaluated in large contemporary studies.
This study is limited by a small sample size and risk of type 2 statistical error. Multivariate analyses were very limited when analyzing factors associated with outcome. It is believed that contemporaneous data from national and international registries 23 and multi-center collaboration in patients undergoing ER for PAA may overcome these shortcomings in a real-world setting. A significant proportion, 77%, of patients undergoing elective ER in the present study did not adhere to the IFU, which implies that carrying through a randomized controlled trial between elective ER with the same strict IFU criteria and OR of PAA would be very challenging.
Conclusion
IFU for endovascularly treated PAA with Viabahn® stent grafts were not met in 82% of all patients. Diameter size difference >1 mm between overlapping stent grafts was associated with higher loss of primary patency at one year. Future multi-center studies with long-term follow-up of patency are warranted to achieve further understanding on the role of endovascularly treated PAA.
Supplemental Material
sj-pdf-1-vas-10.1177_17085381211007312 - Supplemental material for Adherence to instruction for use after endovascular repair of popliteal artery aneurysm
Supplemental material, sj-pdf-1-vas-10.1177_17085381211007312 for Adherence to instruction for use after endovascular repair of popliteal artery aneurysm by Axel Wrede, Leena Lehti, Jonas Peter Eiberg and Stefan Acosta in Vascular
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.