
Abstract
Renal artery aneurysm (RAA) concomitant with a renal arteriovenous fistula (RAVF) has been infrequently reported in the literature. We report a case of a 42-year-old man suffering from a giant RAA combined with a congenital high-flow RAVF. The contrast-enhanced CTA showed a 12.7-cm RAA synchronous with an RAVF between the right renal artery and a draining vein. After a comprehensive preoperative assessment, an endovascular approach was decided. Successful embolization was performed using an Amplatzer vascular Plug, and multiple coils. Completion angiogram demonstrated no flow into the RAA. The results of longterm follow-up demonstrate that endovascular techniques are safe and effective for the management of RAAs combined with high-flow RAVF.
Introduction
Renal artery aneurysms combined with renal arteriovenous fistula are rare lesions. Primary reasons include congenital abnormality, trauma-biopsy, tumor, and inflammation.1–3 Clinical presentation is usually silent or may include pain, hematuria, and retroperitoneal hemorrhage. 4 Giant RAAs combined with high-flow RAVF are difficult to treat. Open surgery is associated with significant morbidity and mortality. 4 In recent years, endovascular therapy has become the standard treatment for unruptured RAAs because of minimal invasiveness, high success rate, and fewer complications.4,5 Herein, we describe the case of a 42-year-old male with a congenital right renal AVM, which was successfully treated with embolization.
Case presentation The case pertains to a 42-year-old Caucasian male, who was admitted to our department as a referral to a tertiary medical center for management of a right RAA with AVF. Symptoms at presentation included only episodic right flank pains. His surgical history included heart valve replacement with a mechanical one and left inguinal hernia repair. There was no history of drug abuse or smoking. Physical examination revealed the presence of a palpable pulsatile mass and an abdominal bruit. ECG and chest radiography were normal. His medication included acenocoumarol and metoprolol. Before admission, acenocoumarol was discontinued and low molecular weight heparin was initiated. The routine laboratory values were within normal limits on admission with Hct: 41.1%, urea: 62.6 mg/dL, creatinine: 1.1 mg/dL, and INR: 0.97. Cardiac echocardiography showed normal systolic function (left ventricular ejection fraction: 55%) and normally functioning prosthetic valve. A contrast-enhanced computed tomography angiography scan using 0.75-mm cuts with delayed images demonstrated a 12.7-cm aneurysm of the right main renal artery (Figures 1 and 2). There was an arteriovenous fistula between the aneurysmal right renal artery and the draining renal vein. No other vascular anomaly was documented. Since there was no previous history of trauma, surgery, or any interventional manipulation in the right kidney, this was considered likely to be a congenital AVM. Νonetheless, before heart valve replacement, patient had undergone an interventional procedure with right transfemoral cardiac catheterization. Therefore, the possibility that our event was a result of a previously misplaced wire cannot be excluded. The patient underwent a digital subtraction angiography in order to plan treatment. Following a multidisciplinary discussion with interventional radiologists, an endovascular approach was decided. The patient was fully informed for the endovascular repair and the possible complications of the operation. After written consent, the patient was admitted for intervention. The procedure was performed under local anesthesia, arterial access was gained with ultrasound-guided percutaneous retrograde puncture of the left axillary artery and retrograde puncture of the right common femoral artery, using 10F sheaths and catheterization of the right renal artery. Our primary attempt through the femoral approach was unsuccessful since the advance of the devices to the desirable point was unfeasible. Furthermore, a radial or brachial access was impractical because the diameter of these vessels did not allow the passage of the interventional equipment. Antegrade right renal arteriography showed the large intrarenal aneurysm concomitant with the high-flow AVF and visualizing the inferior vena cava (Figure 3). Embolization was performed using a 22-mm Amplatzer Vascular Plug (AVP) deployed into the main trunk of the renal artery. Coil embolization was performed with multiple (six used in total), retrievable metallic coils (20, 18, 14, and 12 mm). Completion angiography demonstrated complete obliteration of the RAVF and the aneurysm (Figure 4). In clinical examination following embolization, the palpable pulsatile mass was gone. The post-interventional period was uneventful, the patient maintained good urine output without hematuria. Although, he had a brief elevation in serum creatinine on the fourth postoperative day, was treated with adequate hydration, and had returned to normal level on the seventh postoperative day. By the time of discharge, his biochemical and coagulation parameters were within normal limits with Hct: 30.9%, urea: 22.1 mg/dL, and creatinine: 1.3 mg/dL. He was discharged on the seventh postoperative day in good physical conditions under acenocoumarol. Postoperatively, a renal color duplex ultrasound was performed showing complete occlusion of the RAA. The follow-up involves duplex ultrasound every 6 months.
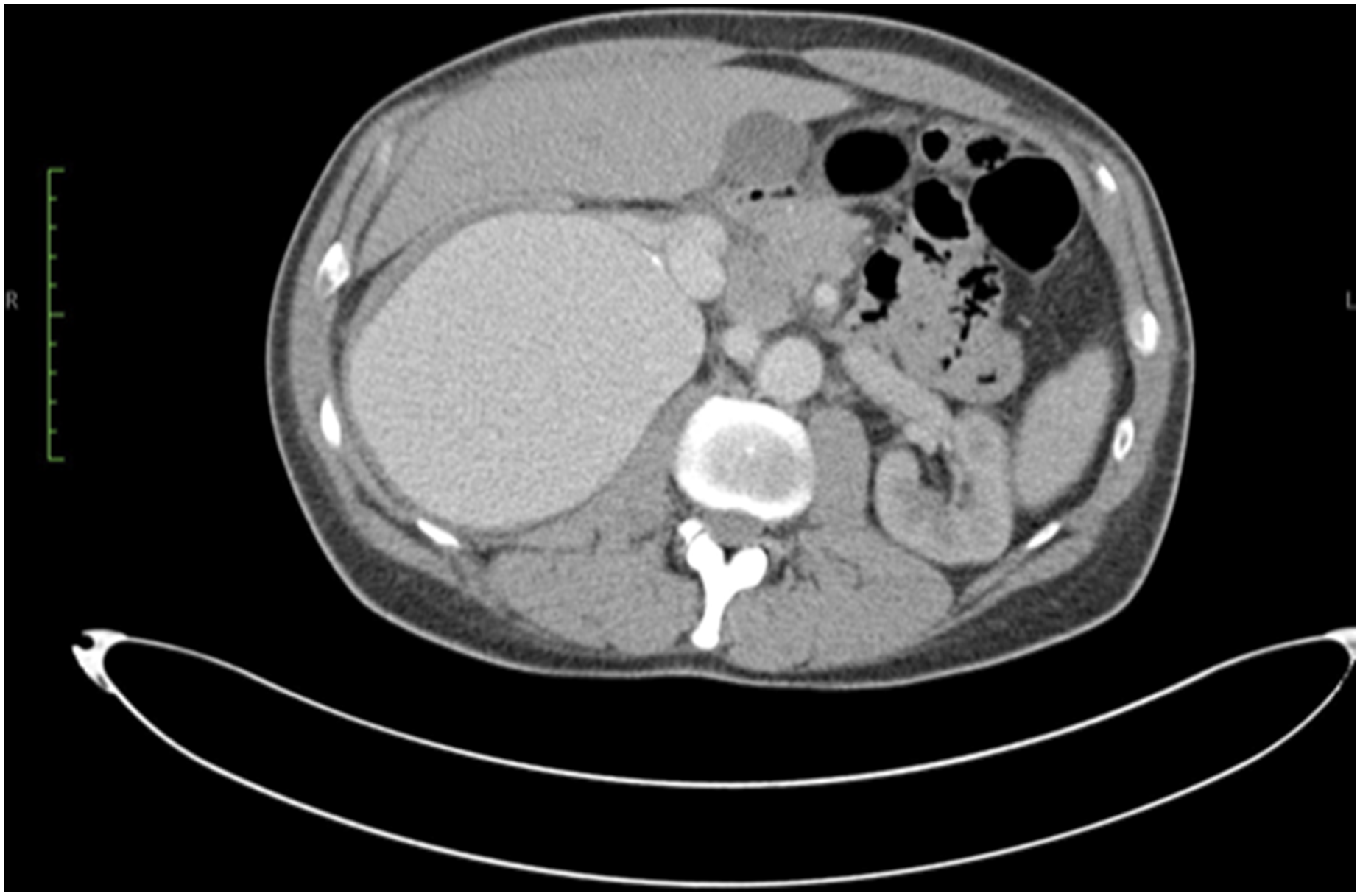
Pre-operative CT-angiography depicting.
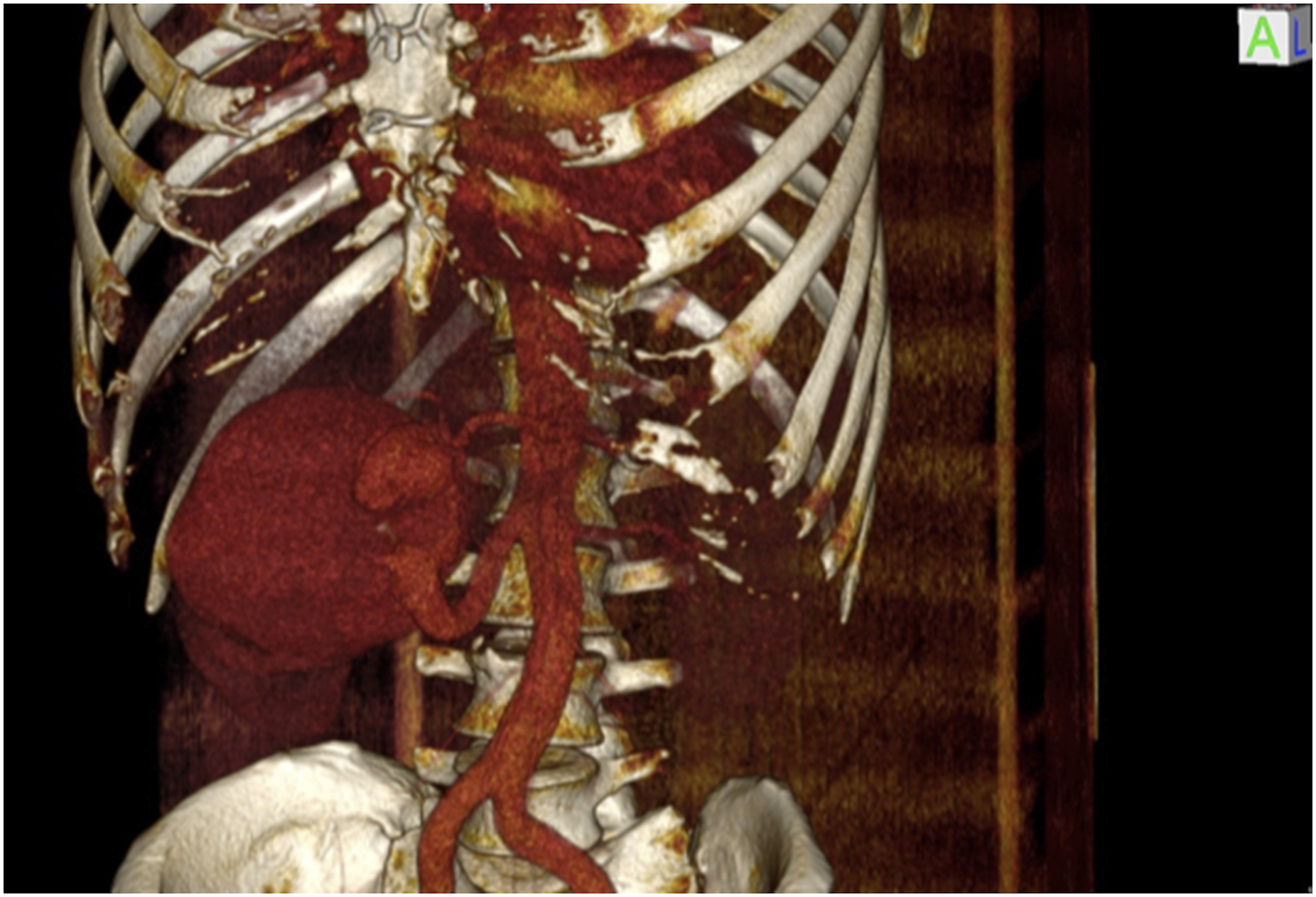
3D reconstruction depicting the giant aneurysm, the feeding right renal artery, and part of the venous outflow.
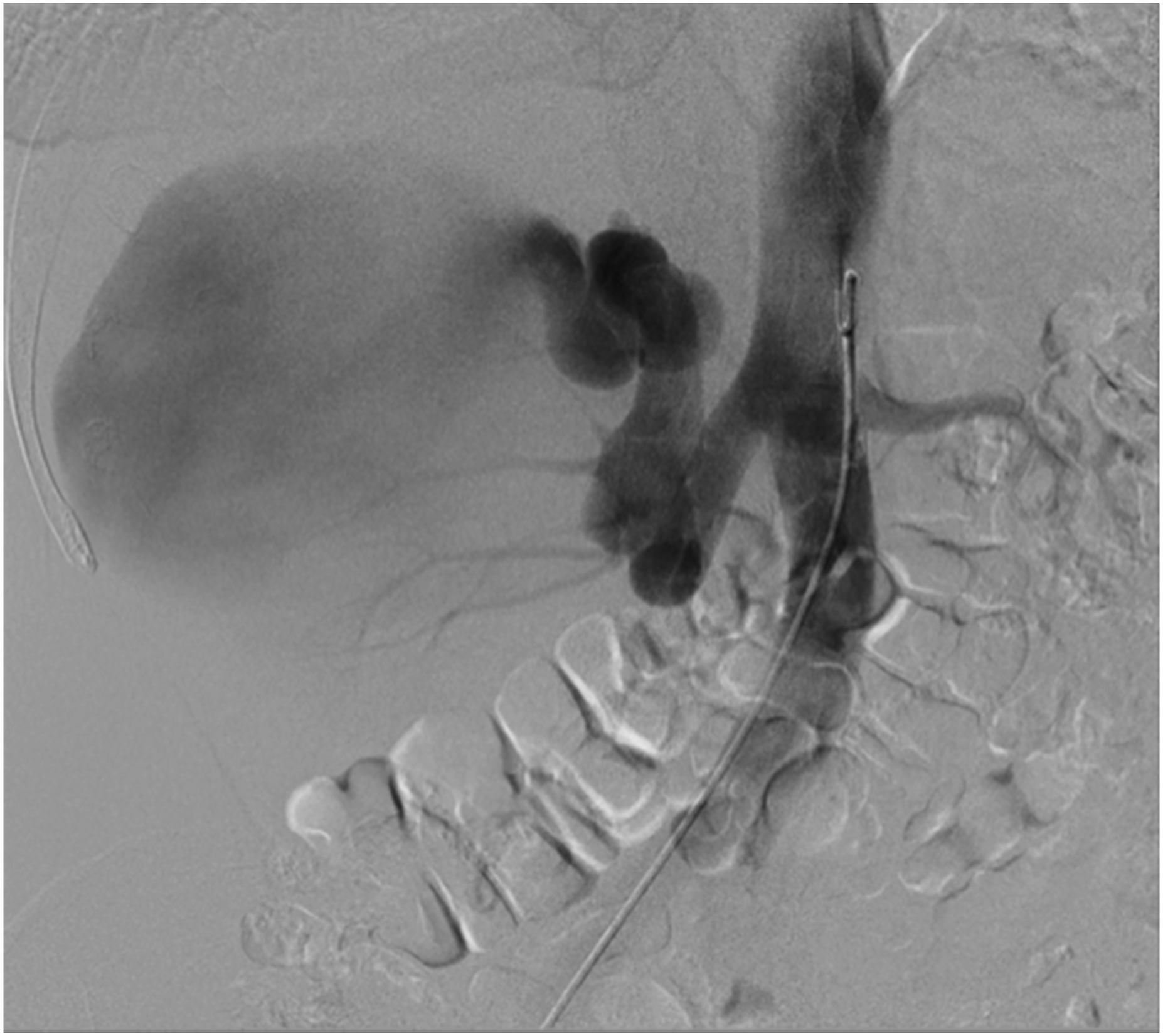
Initial digital subtraction angiography demonstrating in detail the arteriovenous high-flow communication and the large venous outflow.
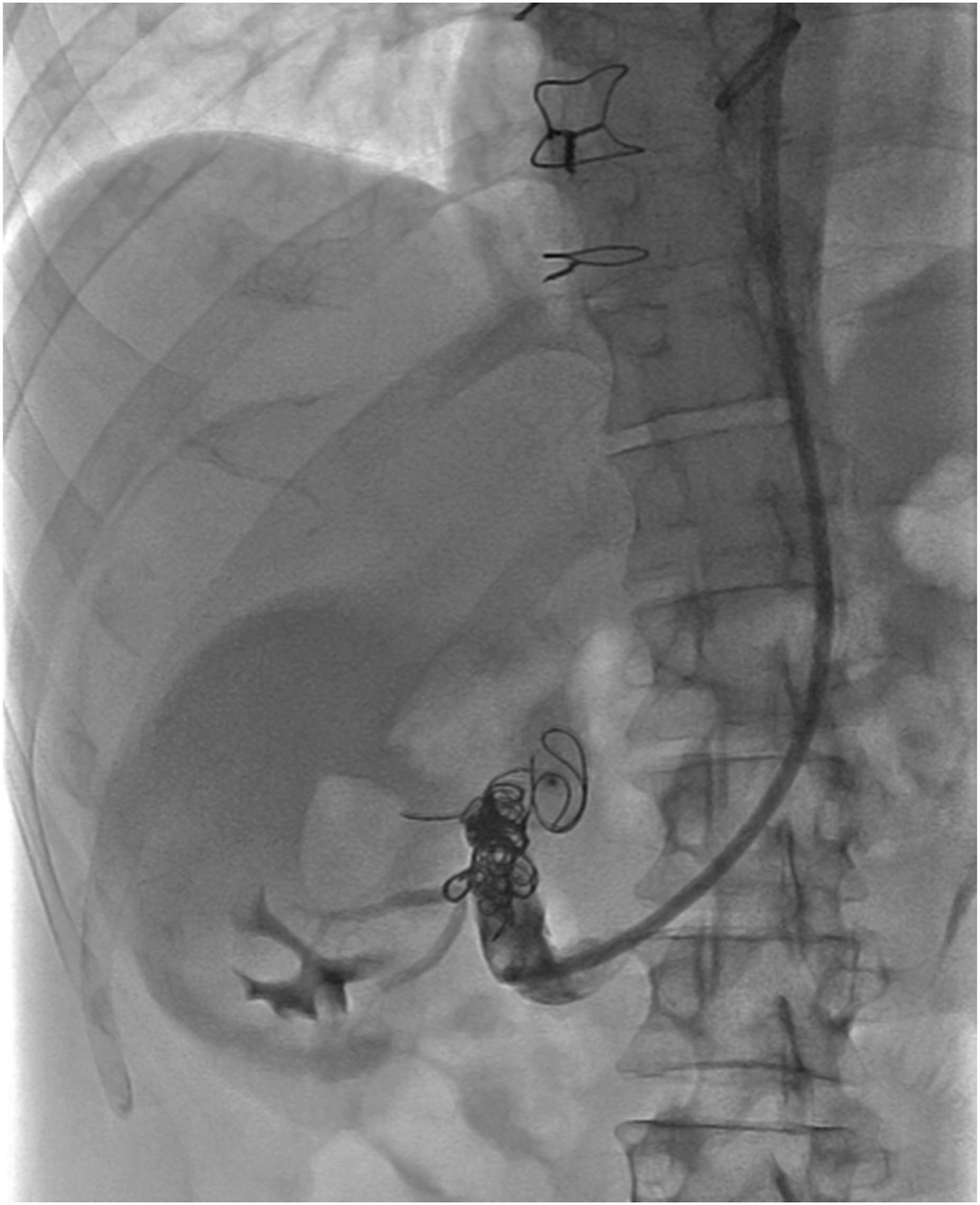
Final selective digital subtraction angiography from the right renal artery, demonstrating the complete occlusion of the lesion.
Discussion
Renal artery aneurysm (RAA) is a rare disease accounting for about 1% of all aneurysms, with an incidence less than 1% in the general population.6–8 It was first reported in 1770 by Rouppe, who described the death of a sailor due to rupture of a large false aneurysm. 9 Conditions associated with RAA include fibromuscular dysplasia, arteritis, atherosclerosis, and trauma. 10 Renal artery aneurysms are considered giant with a diameter exceeding 5cm. 11 Renal arteriovenous malformations (AVM) are defined as aberrant direct vascular connections between the renal arterial and venous systems, bypassing the usual capillary bed.1,2 The first report of arteriovenous fistula was made by Varela in 1928. 11 There are three types of AVM: acquired, congenital, and idiopathic. The acquired renal arteriovenous fistula (AVF) is the most common and accounts for approximately 70% of renal arteriovenous abnormalities.1,2 The incidence of acquired renal AVF is increasing due to the increase in percutaneous interventions, such as biopsy, renal angioplasty, and nephrostomy placement. Other causes of acquired AVFs include trauma, surgery, tumor, or inflammation.1–3 The congenital type is relatively rare with prevalence estimated at less than 0.04%, encompassing only 25% of renal AVF, but represents a potential cause of significant morbidity.3,12 Based on the size, location, and number of vessels involved, congenital RAVFs have been classified into three categories: cirsoid, angiomatous, and aneurysmal.12,13 Aneurysmal AVFs are believed to occur as a result of the close proximity of a vein, which first becomes compressed and then stretched by the adjacent aneurysm. Eventually, the fistulization is considered to be a result of gradual erosion and aneurysmal rupture into the vein.8,11
Renal AVM is usually asymptomatic but can result in gross hematuria, which is the most common symptom and can be fatal; hypertension of unknown cause; abdominal or flank pain; cardiac failure; and left ventricular hypertrophy.1,3,14 The risk of spontaneous rupture is small; however, it may be sudden, and dramatic, associated with mortality rates of up to 80%, presenting as massive retroperitoneal hemorrhage requiring emergency intervention.10,15 Symptoms of RAA consist of flank pain, hematuria, renal infarction, and uncontrolled hypertension. 16 A rupture of the aneurysm is suspected when the triad of hematuria, flank mass, and abdominal pain occurs. 17 Diagnosis of renal AVFs can be made by color duplex ultrasound which is the noninvasive test of choice for screening patients.3,18 The use of DUS is limited by the difficulty in distinguishing an AVF from an aneurysm. 3 Computed tomography angiography using 2.5-mm cuts with delayed imaging and magnetic resonance angiography provides good visualization of the feeding and draining vessels. 18 However, digital subtraction angiography (DSA) remains the definitive diagnostic modality for renal AVF. 3
Currently, management options available for RAA-AVFs include a conservative approach, endovascular techniques, or surgical resection. Treatment is indicated for symptomatic and ruptured RAAs, larger than 2 cm, or with rapid expansion, in pregnant women or in women of child-bearing age, and for RAAs with an RAVF.3,5,16 Indications for treatment of RAVFs include the development of symptoms or significant hemodynamic effects. 16 Management depends on size, expansion rate, age, location, presence of renal insufficiency, unilateral kidney, and the patient’s physiological condition.8,10 Conservative treatment with observation and serial evaluation is indicated in asymptomatic or small RAA-AVFs.11,16 Endovascular techniques have been well documented, and renal artery embolization, in recent years, has been the treatment of choice using staged methods such as metallic coils, sclerosis liquid agents (such as alcohol and n-butyl 2-cyanoacrylate), particulate materials (such as gelatin-sponge particles and polyvinyl alcohol), and vascular plugs which reduce flow and cause thrombosis of the fistula.15,19,20 Particle embolic materials have a higher risk of pulmonary embolization with high-flow fistulas and are thus not recommended. 20 In addition, another endovascular therapeutic option involves the use of covered stents in order to exclude the aneurysm or bare metal stents for protection of the main renal artery, while embolization is performed through the interstices using metallic micro-coils. 8 A relatively safe method of closure is the use of releasable balloons mounted on a coaxial microcatheter producing complete fistula occlusion. 15 Endovascular treatment is technically challenging in cases with tortuous, dilated renal arteries and calcified aneurysms. 21 Complications include renal parenchymal infarction, postembolization fever, flank pain, coil migration (particularly in high-flow fistula with a large diameter or wide-neck aneurysms), systemic and pulmonary embolism, erosion of coils into the colon, and incomplete occlusion.10,15 Open surgical techniques have historically been the treatment of choice and include aneurysmectomy, with patch angioplasty or interposition grafting, ligation of feeding vessels, ex-vivo repair and autotransplantation, aortorenal bypass, and extra-anatomic bypass.3,10 Surgical treatment is still performed in case of rupture with hemodynamic instability or after failure/nonfeasibility of endovascular techniques.4,16 Total or partial nephrectomy is an acceptable option for nonreconstructible anatomy, end-stage ischemic nephropathy, and rupture. 10 The main disadvantages of surgical treatment include high morbidity and mortality, potential significant bleeding, and the need for prolonged hospitalization. 4 It is generally accepted that follow-up consists of duplex ultrasound initially at 1 month, then 6 months, and yearly after that. 16 A CTA or MRA should be performed to classify any abnormality. 16
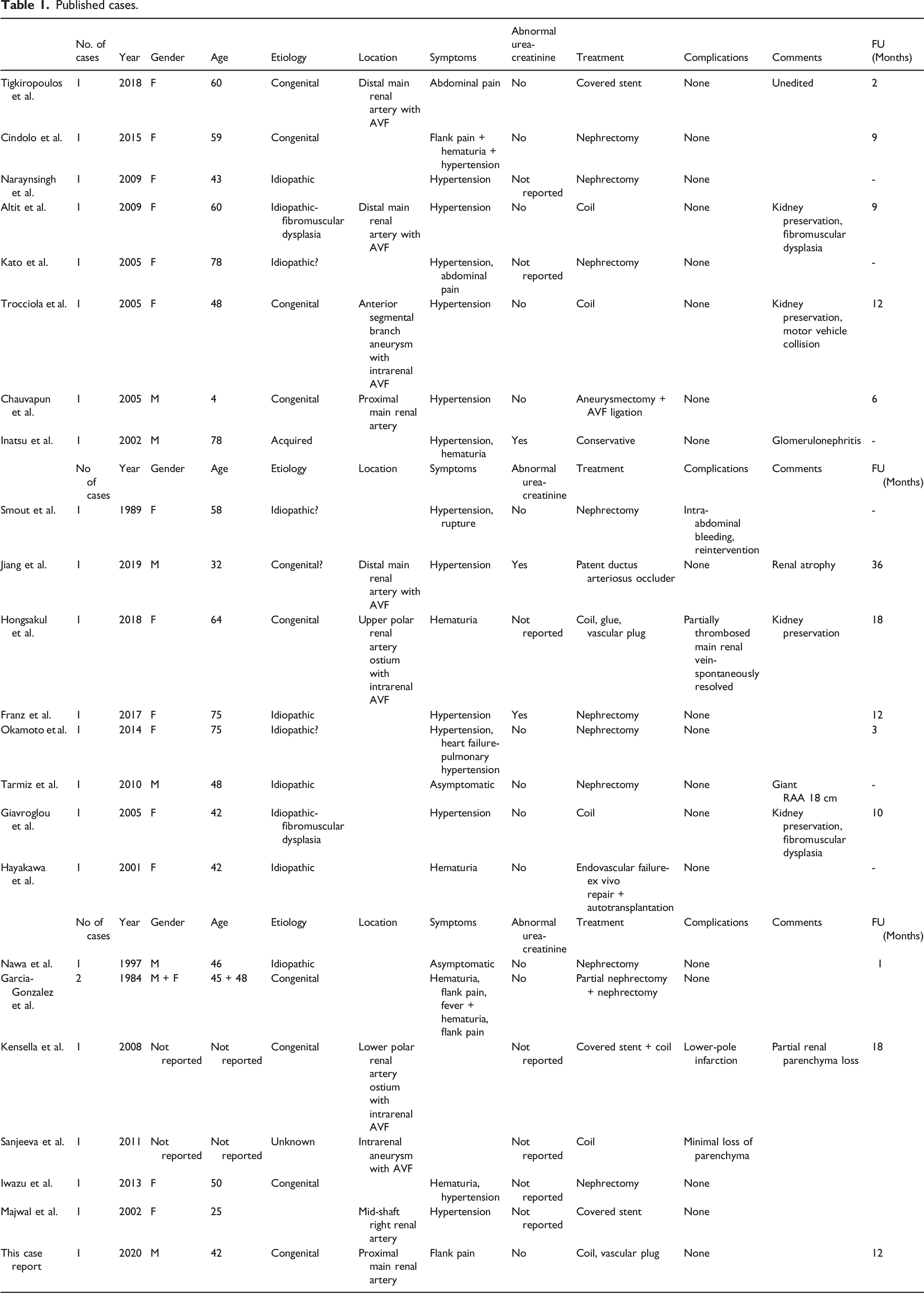
Published cases.
Conclusion
Renal arteriovenous malformation combined with renal artery aneurysm, especially giant RAA, is a rare disease. The first line of treatment is endovascular repair including embolization and stent-grafts’ usage. Endovascular treatment using coil embolization in selected patients is effective and is associated with low incidence of mortality and complications.
Footnotes
Author Contributions
GP was a major contributor in writing the article and contributed with conception, literature review and analysis, drafting, critical revision, and editing. GS contributed to this article with writing, literature review and analysis, drafting, critical revision, and editing. NT contributed to this article with writing, literature review and analysis, drafting, critical revision, and editing. SS contributed to this article with writing, literature review and analysis, drafting, critical revision, and editing. EB contributed to this article with writing, literature review and analysis, drafting, critical revision, and editing. GG contributed to this article with writing, literature review and analysis, drafting, critical revision, and editing. All authors read and approved the final article.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Written informed consent was obtained from the patient for publication of this case report and accompanying images.