
Abstract
Objectives
To analyze the association between blood groups (ABO and Rh) and long-term outcomes following abdominal aortic aneurysm (AAA) repair.
Methods
Retrospective cohort study including all patients submitted to elective AAA surgery between 2009 and 2019. Outcomes were mortality and major adverse cardiac events (MACE).
Results
Of the 333 patients included in this study, 49.5% had blood type A, followed by 39.3% with type O, 8.1% with type B and 3.1% with type AB. Regarding Rh factor, 82.4% were Rh+ and 17.6% were Rh-. The distribution of the blood phenotypes was similar between AAA patients and the Portuguese population. The median follow-up time was 75.4 months (interquartile range 65.8–81.6). Patient survival rates at 1 and 5 years were 89.3% (95% Confidence Interval 86.0–92.7) and 61.9% (56.2–68.2), respectively. MACE-free survival at 1 and 5 years was 85.7% (81.9–89.5) and 57.6% (51.9–64.0), respectively. Survival and MACE-free survival rates were similar across blood group types. Age, maximum aortic diameter, peripheral arterial disease and chronic obstructive pulmonary disease were independent predictors of mortality. Maximum aortic diameter, estimated glomerular filtration rate, cerebrovascular disease and type of surgery were independent predictors of MACE.
Conclusion
We found no association between the blood types and the prevalence of AAA or adverse outcomes following AAA repair.
Keywords
Highlights
ABO and Rh blood groups of AAA patients were similar to the Portuguese population. Patient survival was 61.9% and MACE-free survival 57.6% at 5 years. Age, aortic diameter, PAD, COPD were independent predictors of mortality. Aortic diameter, GFR, cerebrovascular disease, surgery type were predictors of MACE. Survival and MACE-free survival rates were similar across blood group types.
Introduction
The prevalence of abdominal aortic aneurysms (AAA), the most common type of aortic aneurysm, ranges from 1.7% to 12.7%.1,2 Most AAA remain asymptomatic until rupture, a complication associated with high mortality. The risk of rupture increases with aneurysm size and European guidelines recommend surgery when the aneurysm diameter exceeds 5 cm in women and 5.5 cm in men. 3 The pathophysiology of AAA is complex and multifactorial, involving both environmental and genetic factors. Major risk factors include age over 65 years, male sex, hypertension, smoking and atherosclerosis. 4 Research continues to identify additional risk factors for AAA development.
The ABO blood group is the major human antigen system, classified by the presence of A and B antigens on the surface of erythrocytes. ABO glycosyltransferases, also modify surface glycoproteins on platelets, vascular endothelium, epithelium and other cell types, suggesting potential roles beyond blood typing. 5 In 1939, Levine and Stetson described the first human example of an antibody against another antigen that exists on the surface of the erythrocyte, the later called antigen D. Rh(D) blood group has been associated with hemolytic disease of the newborn and it is unknown if it plays a role in vascular disease. Associations between ABO blood group and vascular diseases have been identified including venous and arterial thromboembolic events,6,7 coronary artery disease (CAD),8–10 myocardial infarction, 11 stroke11,12 and peripheral artery disease. 13
The role of blood groups in the development of complications after cardiovascular repair has also been studied. Differences in blood product use and mortality were observed in relation to the ABO blood groups of patients that underwent coronary artery bypass surgery.14,15 This finding was not confirmed in adult patients who underwent surgical aortic valve replacement with porcine bioprosthetic valves. 16 In these patients, no significant association was found between patient ABO blood type and clinical manifestations of structural valve deterioration, heart failure or death.
Evidence linking ABO blood group or Rh factor to aortic aneurysms is limited. A recent meta-analysis 17 suggests the association of blood group O with reduced AAA prevalence, whereas blood group non-O was associated with a statistically significant increase in AAA prevalence. While an association between blood groups with AAA has been proposed, there are not enough studies to investigate the role of blood groups in the development of complications after AAA repair.
The goal of this study is to analyze the association between blood groups and the prevalence of AAA, as well as outcomes following AAA repair, within the Portuguese population.
Methods
Study design and participants
This retrospective cohort study included consecutive patients who underwent elective AAA surgery, either open surgery repair (OSR) or endovascular aneurysm repair (EVAR), at São João University Hospital between January 2009 and December 2019. Exclusion criteria included additional interventions other than AAA repair, non-infrarenal AAA (juxtarenal, pararenal, paravisceral, thoracoabdominal and thoracic aortic aneurysms), ruptured or symptomatic AAA. After surgery, patients were followed according to European guidelines. 3 The study was approved by the Ethics Committee for Health at São João University Hospital (n.º 287/21) and complies with the Declaration of Helsinki.
Participants’ characteristics
Baseline demographic characteristics (gender, age), blood type (ABO and Rh) and cardiovascular risk factors were collected retrospectively from the electronic health records. Smoking represented past or present cigarette consumption. Body mass index (BMI) was calculated (weight in kg divided by the square height in m2) and the patient considered obese if BMI ≥30 kg/m2. Coronary artery disease (CAD) was defined as angina, previous myocardial infarction or previous revascularization procedure, either percutaneous coronary intervention or coronary artery bypass graft. Congestive heart failure was based on clinical and echocardiogram findings. Cerebrovascular disease (CVD) was defined by previous stroke or transient ischaemic attack (TIA) or if asymptomatic carotid stenosis >50%. Glomerular filtration rate (GFR) was calculated based on preoperative plasmatic creatinine levels and Chronic Kidney Disease diagnosed when GFR <30 mL/min. 18 Peripheral artery disease (PAD) was considered if patient had intermittent claudication (Fontaine IIa/b or Rutherford 1–3) or critical limb ischaemia (Fontaine III/IV or Rutherford 4–6). Chronic obstructive pulmonary disease (COPD) was assumed if listed as a medical problem by the physician or if pulmonary function tests showed an obstructive pattern. Other characteristics included maximum diameter of the AAA, American Society of Anesthesiologists (ASA) physical status classification system, drugs that the patient was taking at admission, previous abdominal surgery and type of surgery.
Data regarding the distribution of blood types in the Portuguese population was collected from the Portuguese Blood Institute. 19 We estimated the proportion of ABO and Rh blood types assuming that ABO alleles and Rh alleles are inherited independently. 20
Outcomes
The primary outcome was patient survival. We collected the clinical status (dead or alive) and the date of death. The secondary outcome was freedom from major adverse cardiovascular events (MACE) defined as acute myocardial infarction, stroke or all-cause death. 21 Outcomes were collected retrospectively from electronic records of our institution and from integrated records for events occurring outside our center, including primary care, other secondary and tertiary care institutions.
Statistical analysis
Descriptive statistics were expressed as mean ± standard deviation (SD), except when normality could not be assumed, in which case we used median and interquartile range (IQR). Categorical variables were expressed with absolute frequencies (n) and relative frequencies (%). Missing values ranged from 0 to 9%. Proportions of ABO and Rh distributions in our sample were compared using the one-sample test of proportions, comparing against the reference value. 19 Survival curves were obtained with the Kaplan–Meyer model. In life table graphs, lines were truncated when the standard error exceeded 10%. Differences between Rh+ and Rh- or between O and non-O types were ascertained with the log-rank test or with ratio of Restricted Mean Survival Time (RMST) that is the population average of the amount of event-free survival time experienced during a predefined follow-up time, that can be estimated by the area under the Kaplan–Meier curve up to that timepoint. RMST is used when difference between the two survival curves is not constant over time, violating the proportional hazards assumption. Multivariate models were created for mortality and MACE. Variables were included in the model if clinically relevant and presented a p-value in the univariate analysis of <0.200. Statistical analysis was performed using Stata 15 (StataCorp, 4905 Lakeway Dr College Station, TX 77845 USA) and R 4.1.1 (2021-08-10) for Windows®. A p-value of less than 0.05 was used to determine statistical significance.
Results
Participants’ characteristics
Participants’ characteristics (overall and per ABO and Rh blood groups).
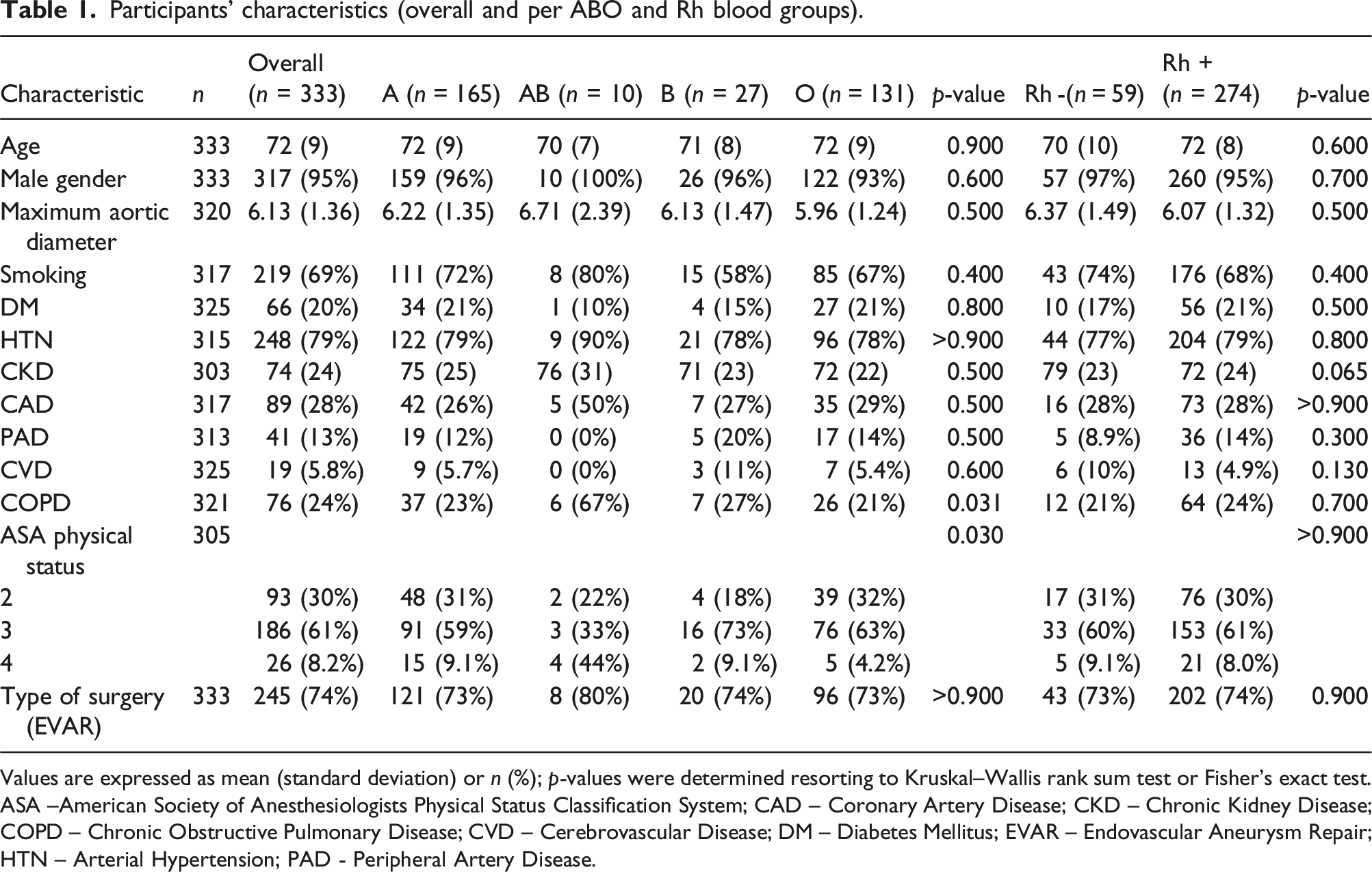
Values are expressed as mean (standard deviation) or n (%); p-values were determined resorting to Kruskal–Wallis rank sum test or Fisher’s exact test. ASA –American Society of Anesthesiologists Physical Status Classification System; CAD – Coronary Artery Disease; CKD – Chronic Kidney Disease; COPD – Chronic Obstructive Pulmonary Disease; CVD – Cerebrovascular Disease; DM – Diabetes Mellitus; EVAR – Endovascular Aneurysm Repair; HTN – Arterial Hypertension; PAD - Peripheral Artery Disease.
Blood groups distribution
The distribution of ABO (Figure 1(A)) and Rh blood phenotypes (Figure 1(B)) in AAA patients was representative of the Portuguese population (39.9% versus 38.9% for A Rh+, p = .736; 9.6% versus 7.7% for A Rh-, p = .232; 2.7% versus 2.9% for AB Rh+, p = .989; 0.3% versus 0.6% for AB Rh-, p = .775; 6.6% versus 6.4% for B Rh+, p = .974; 1.5% versus 1.3% for B Rh-p= .897; 33.0% versus 35.3% for O Rh+, p = .422 and 6.3% versus 7.0% for O Rh-, p = .699). Distribution of ABO blood group (A) and of Rh blood group (B) in our sample comparing to distribution in the Portuguese population.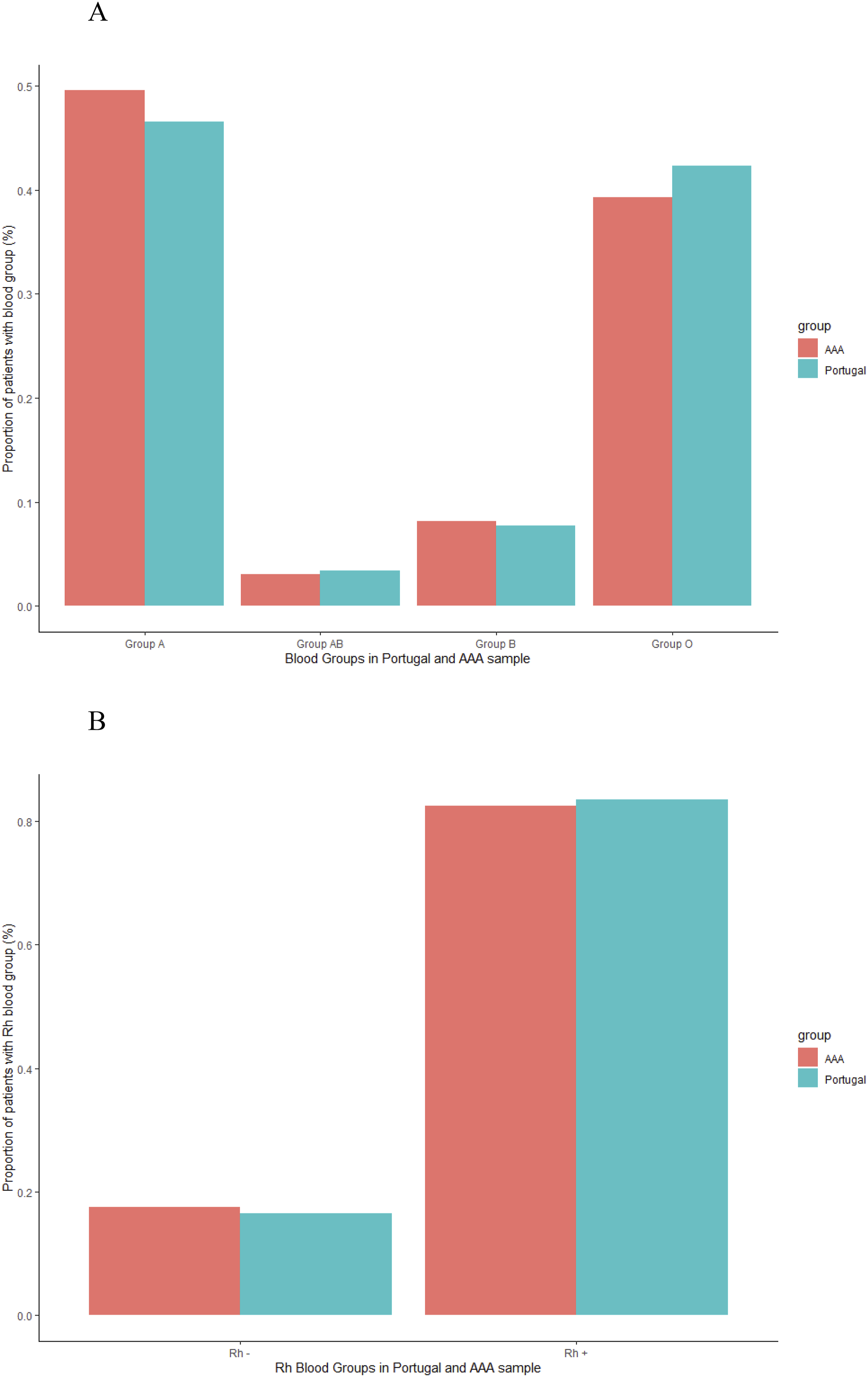
Patient survival
Patients had a median follow-up time of 75.4 months (IQR 65.8–81.6), during which 144 patients died. Patient survival rates were 89.3% at 1 year (95% Confidence Interval [CI] 86.0–92.7), 84.7% at 2 years (80.8–88.8) and 61.9% at 5 years (56.2–68.2) (Figure 2(A)). At 60 months, RMSTs did not differ between patients with blood type O and non-O (48.1 [45.6–50.7] vs 45.7 [45.1–52.4] months, p = .796) (Figure 2(B)). Similarly, at 60 months, RMSTs were comparable between patients with Rh- and Rh+ blood types (48.5 [46.2–50.8] vs 47.4 [42.0–52.8] months, p = .713) (Figure 2(C)). Patient survival after elective surgery of AAA (A), and for blood type versus non-O blood type (A, AB and B) (B) and Rh blood type (C).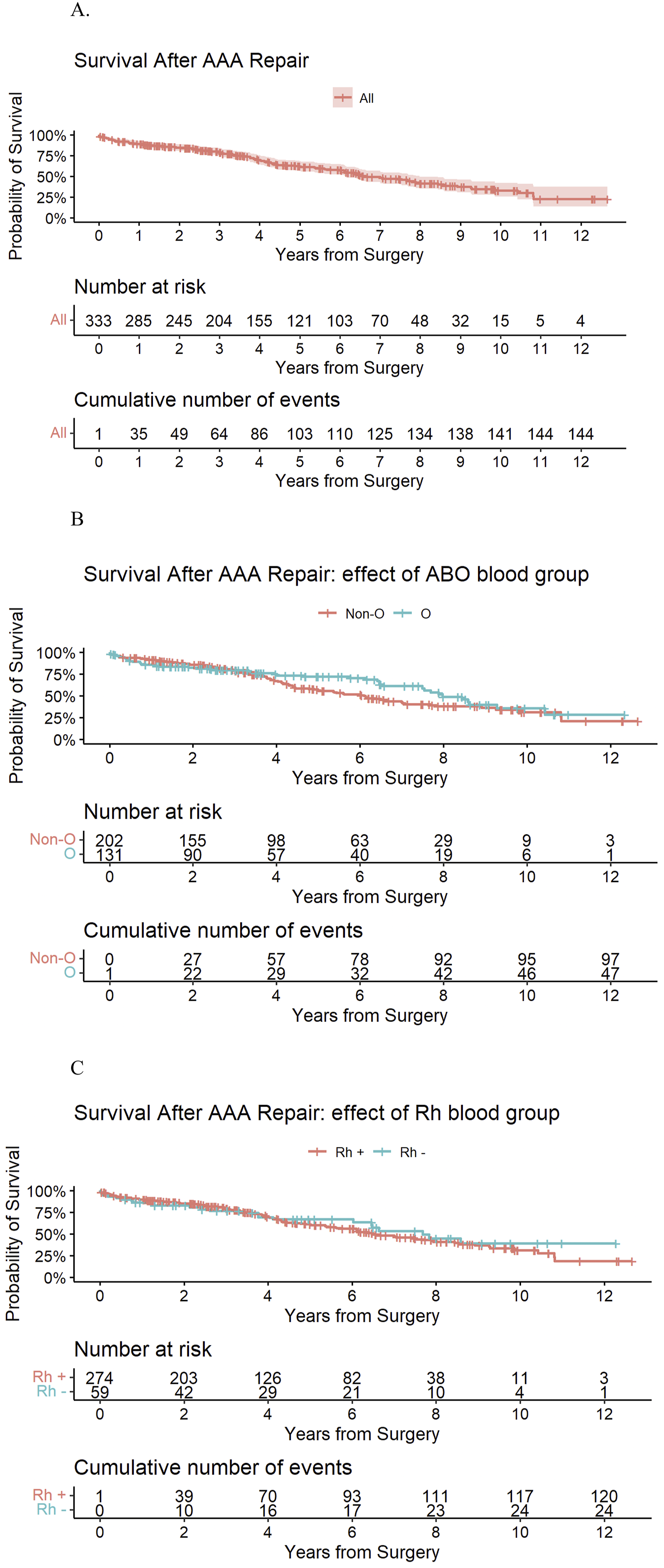
Univariate and multivariate Cox regression analysis for the outcomes mortality and MACE.
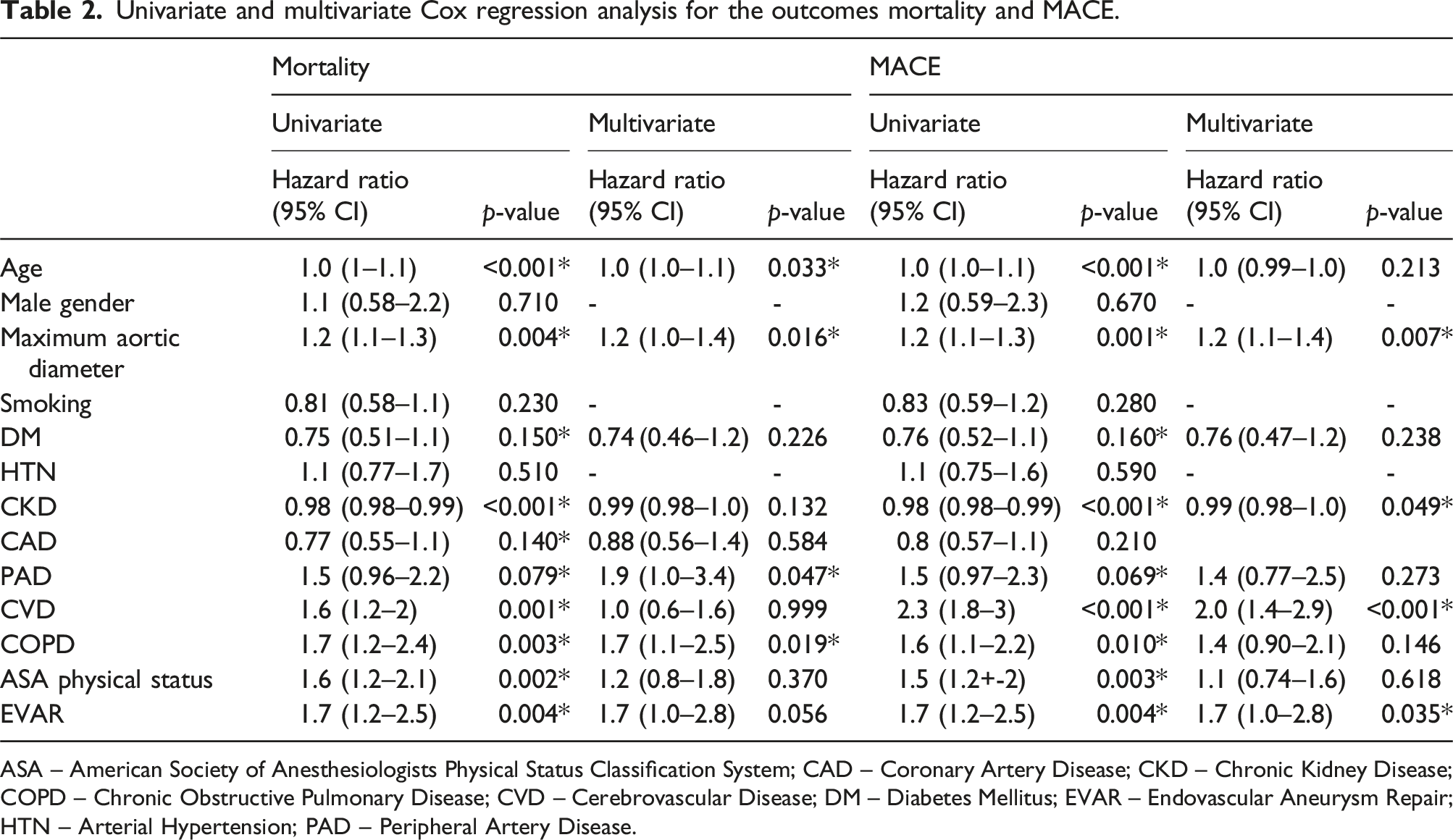
ASA – American Society of Anesthesiologists Physical Status Classification System; CAD – Coronary Artery Disease; CKD – Chronic Kidney Disease; COPD – Chronic Obstructive Pulmonary Disease; CVD – Cerebrovascular Disease; DM – Diabetes Mellitus; EVAR – Endovascular Aneurysm Repair; HTN – Arterial Hypertension; PAD – Peripheral Artery Disease.
Freedom from MACE
There were 159 MACE events, including 16 cases of stroke or TIA, 18 acute myocardial infarctions (AMI) and 125 all-cause deaths. The distribution of MACE events by the blood groups was as follows: 86 in blood type A, 5 in type AB, 12 in type B and 57 in type O. MACE-free survival rates were 85.7% at 1 year (81.9–89.5), 79.7% at 2 years (75.4–84.3) and 57.6% at 5 years (51.9–64.0) (Figure 3(A)). At 60 months, RMSTs in freedom from MACE did not differ between patients with blood type O and non-O (Figure 3(B)), nor between Rh- and Rh+ patients (Figure 3(C)), being 46.8 (44.4–49.2) versus 46.8 (40.8–49.2) months, p = .323 and 48.0 (45.6–50.4) versus 45.6 (39.6–51.6) months, p = .500, respectively. Kaplan–Meyer curves for MACE-free survival after elective surgery of AAA (A), and for -blood type versus non-O blood type (A, AB and B) (B) and Rh blood type (C).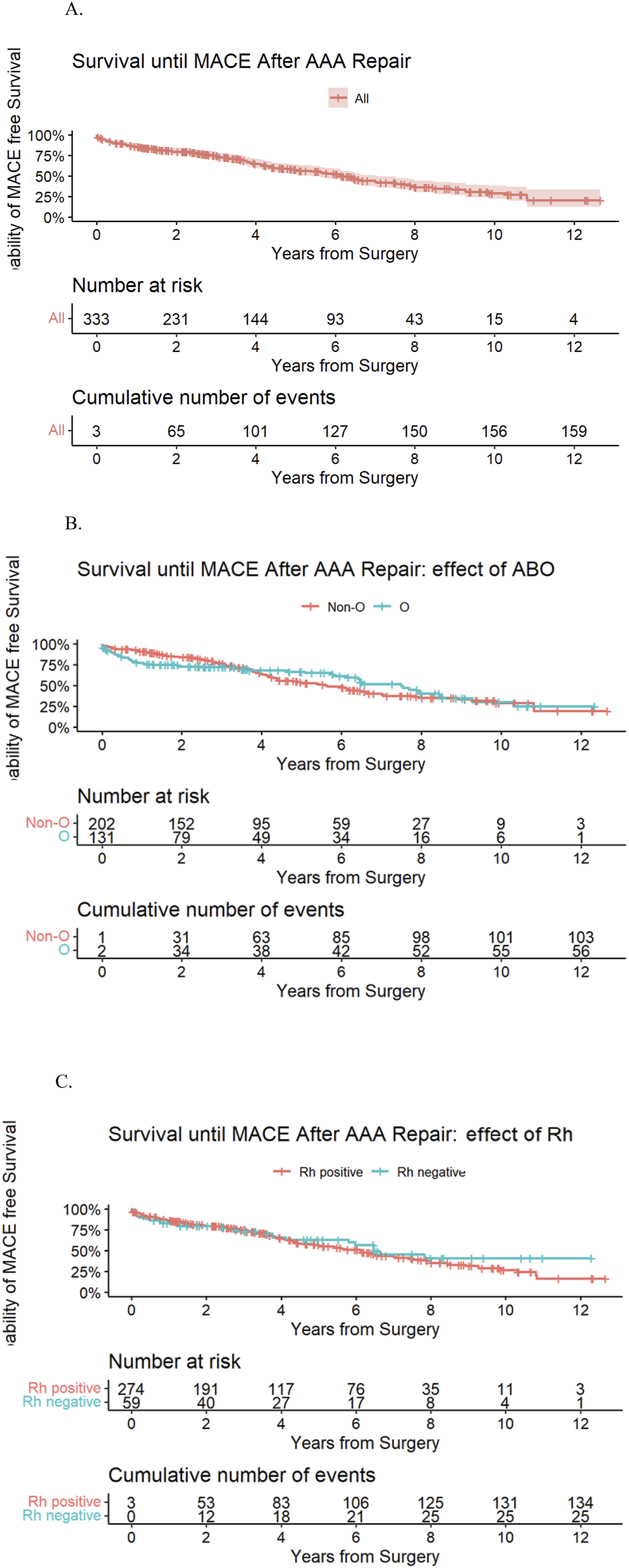
In the univariate Cox regression, age, maximum aortic diameter, diabetes mellitus, CAD, PAD, CVD, CKD, COPD, ASA classification and type of surgery were associated with MACE (p < .200) and were included in the multivariate model (Table 2). The multivariate analysis showed that maximum aortic diameter, CKD, CVD and type of surgery were independent predictors of MACE.
Discussion
We found no association between different blood types and the presence of AAA or adverse outcomes following AAA repair.
The putative pathophysiological link between non-O blood groups and arterial thromboembolic events involves von Willebrand factor (VWF). Plasma VWF serves two crucial functions in normal haemostasis. First, it facilitates the interaction between platelets and the damaged areas of the blood vessel wall. Second, VWF functions as a carrier for procoagulant Factor VIII (FVIII), helping to localize FVIII to sites of vascular injury. 22 An important factor contributing to the wide variation in normal plasma VWF levels is the ABO blood group phenotype. 23 Orstavik and colleagues 24 discovered that 66% of the total variability in plasma VWF levels is genetically determined, with 30% of this variation attributable to the ABO blood group. A review also highlighted that studies consistently show individuals with blood group O have plasma VWF levels that are 25 to 30% lower than those with non-O blood types. 25 This variation holds clinical importance. Elevated levels of the VWF-FVIII complex are linked to an increased risk of myocardial infarction and venous thromboembolism,26,27 while a deficiency in VWF is the cause of the most common inherited bleeding disorder in humans – von Willebrand disease (VWD). 28
ABO carbohydrate antigenic determinants are expressed on the N-linked glycan chains of circulating plasma VWF. Recent studies suggest that there may be significant heterogeneity in the amount of ABO expression on VWF secreted by endothelial cells from different vascular beds.29,30 The mechanism by which the ABO group determines plasma VWF levels may affect the rate of VWF synthesis or secretion within endothelial cells. Alternatively, it could influence plasma VWF levels by altering the rate of VWF catabolism, including proteolysis and/or plasma clearance. 25
ABO may also influence activated protein C (APC) resistance. In an unselected prospective longitudinal study of 1671 pregnant women, where resistance to APC occurs in the absence of Factor V Leiden, a higher APC sensitivity ratio was observed in subjects with blood group O and in smokers. Conversely, an inverse relationship between the APC sensitivity ratio and age, diastolic blood pressure and total serum cholesterol was noted. 31 Additionally, investigation into the associations between ABO blood groups and platelet activation, coagulation, fibrinolysis, total lipids, cholesterol and triglycerides revealed no consistent relationships.32–34 Finally, no differences were found between rhesus blood groups and serum cholesterol levels. 35
Previous research has shown that non-O blood groups are associated with CAD, stroke, peripheral vascular disease and venous thromboembolism, but with varying magnitudes. Previous meta-analysis showed that the risk of CAD was significantly higher in blood group A (pooled OR 1.14 [1.03–1.26], p = .01) and lower in blood group O (pooled OR 0.85 [0.78–0.94], p = .0008).8,11 In another meta-analysis, the prevalence of non-O blood group was significantly higher in patients with MI (pooled OR: 1.28 [1.17-1.40]; p < .001) and ischaemic stroke (pooled OR 1.17 [1.01–1.35]; p = .03) than in controls. 11 Finally, the pooled OR of 1.45 (1.35–1.56) was documented for the association between non-O blood groups and peripheral vascular disease, and 1.79 (1.56 to 2.05) for venous thromboembolism. 13 In general, these pooled ORs had higher magnitude than those detected for AAA. Non-O blood groups were related to a statistically significant increase in AAA prevalence with a pooled OR of 1.11 (1.01–1.24), p = .04, while blood group O was associated with a statistically significant reduction in AAA prevalence with a pooled OR 0.90 (0.81–0.99), p = .04. 17 The results of this meta-analysis were further challenged by a later study, 36 which included 2 million Swedish blood donors and transfused patients. In this study, non-O individuals had a similar incidence of aortic aneurysms and/or aortic dissections when compared with group O individuals while blood group B conferred a lower risk of aortic aneurysms in the patient cohort compared with blood group O (incidence rate ratio 0.90 [0.85–0.96]). Yang et al. also did not find differences between blood groups in aortic dissections. 37 Our study aligns with these aortic studies that challenge previous meta-analysis, not being able to reproduce an association between blood groups and the prevalence of AAA.
Our study also did not find an association with outcomes following AAA repair. Likewise, in patients who underwent surgery for ascending aortic aneurysm, aneurysm-related mortality was more frequent in blood group A, although this difference was not statistically significant. 38 Three studies have addressed outcomes after aortic repair for acute type A aortic dissection, yielding discrepant results. Gune H et al. 39 found no association between blood groups and the rates of massive bleeding or re-exploration for bleeding in blood group O and non-O patients. In the study by Nozohoor et al., 40 ABO blood groups were not associated with any significant change in risk of 30-day or late mortality, except for blood group A, which was an independent predictor of late mortality. Finally, Huang et al. 41 studied whether different ABO blood groups affected the prognosis of aortic dissection, in which a large portion of their patients did not receive surgery or stent grafts. They demonstrated that patients with non-O blood types had considerably a lower risk of early mortality, especially in patients with acute type A aortic dissection who did not receive standard surgical intervention (Hazards Ratio (HR) 0.579).
In our study, the lack of association between blood type and outcomes after AAA repair might represent a type II error due to the relatively small sample size. However, for a power of 80% and a probability of a type I error of 5%, we estimate that our sample size would be able to detect differences between patients with non-O and O blood types corresponding to an HR of ≥1.57 for MACE and ≥1.74 for mortality at 6 years follow-up, assuming the event rates and censuring we observed in our sample. If an association not identified in our study exists, it is likely of a lower magnitude than these HRs. This study has other limitations. First, our data was collected retrospectively from the electronic health records at our institution, leading to low but variable degrees of missing data. Second, the prevalence of the blood type groups from AAA patients were compared to the Portuguese population. Our hospital, located in the city of Porto, is a referral centre for the North of the country, and most patients in our sample are from this geographical area, which might not be representative of the entire Portuguese population. Third, a selection bias may also be present, as patients with cumulative comorbidities are less likely to be selected for invasive surgical procedures, potentially causing an unequal distribution of blood groups.
Conclusion
We found no association between blood types and the presence of AAA or adverse outcomes following AAA repair. Age, aortic diameter, PAD and COPD were independent predictors of mortality. Aortic diameter, CKD, CVD and the type of surgery were independent predictors of MACE.
Footnotes
Acknowledgements
We would like to acknowledge Brian Claggett from Harvard Medical School, Brigham and Women’s Hospital, for the statistical support.
Author contributions
TM: data curation, investigation, writing original. FSN: formal analysis, investigation, methodology, writing original, JRN: conceptualization. IM: data curation, methodology. JFT: data curation. PVR: supervision, review and editing of final manuscript. MDN: conceptualization, supervision, review and editing of final manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
The study was approved by the Ethics Committee for Health at São João University Hospital (n.º 287/21) and complies with the Declaration of Helsinki.